
A 71-year-old woman with a history of previous left anterior descending artery (LAD) angioplasty, non-ST-elevation myocardial infarction 13 years earlier (treated medically), and hypertension, presented with persistent, midsternal, non-radiating chest pain for several hours, and was admitted to our center during the outbreak of coronavirus disease 2019 (COVID-19) in Poland. She was transported to our hospital by emergency medical service after electrocardiogram (ECG) e-transmission, which demonstrated ST-segment elevation in inferior leads, and ST depression, and inverted T waves in V1-3 (Figure 1 A). During the transport to the hospital, she was started on a loading dose of ticagrelor and unfractionated heparin. On arrival, she was afebrile; blood pressure was 140/95 mm Hg, and heart rate was 88/min. She denied dyspnea and cough. However, the patient and other members of her family had influenza-like symptoms for 2 weeks prior to admission. She was brought to the catheterization laboratory immediately, where coronary angiography was performed and revealed non-obstructive coronary artery disease and no in-stent restenosis in the LAD (Figures 1 B, C). After the procedure, the patient was transferred directly to the department dedicated to patients with suspected or confirmed COVID-19 at our center. The initial and subsequent high-sensitivity troponin I levels were negative. C-reactive protein and D-dimer levels were mildly elevated, whereas other blood test results, including complete blood count, were within the normal range. Transthoracic echocardiogram demonstrated preserved left ventricular ejection fraction of 50% with inferior and septal hypokinesis. A chest X-ray showed no pulmonary opacities (Figure 1 D). Due to previous influenza-like symptoms, a nasopharyngeal swab (PCR testing) was performed and was positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Considering that the patient’s status was good with only mild symptoms, she was discharged from the hospital and transferred to the isolation unit on the third day of admission.
Figure 1
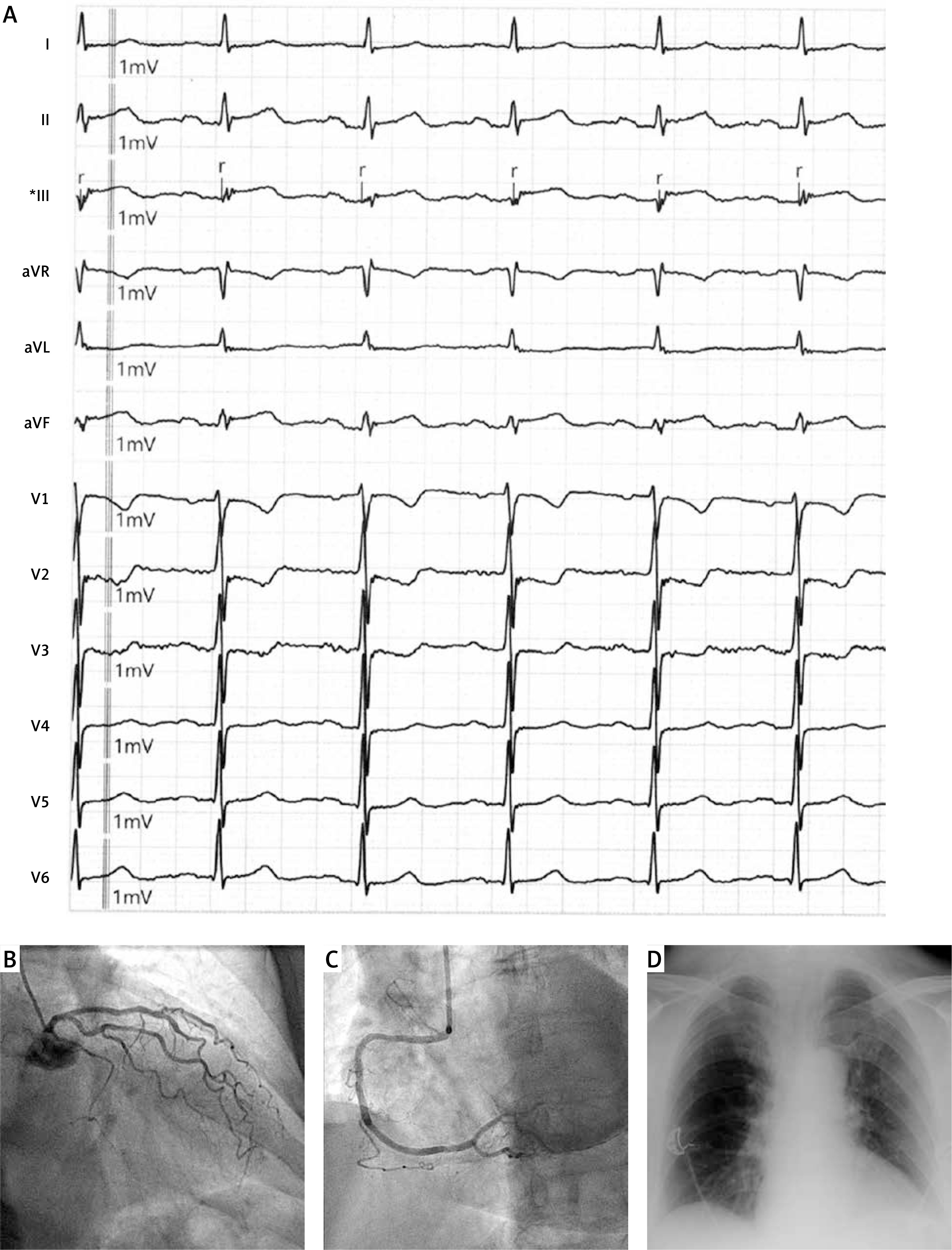
A – 12-lead electrocardiogram demonstrating ST-segment elevation in inferior leads, and ST depression and inverted T waves in V1-3. B – Left coronary angiogram showing non-obstructive stenoses in circumflex and left descending artery and no in-stent restenosis. C – Right coronary angiogram showing non-significant lesions. D – Chest X-ray revealing no pulmonary opacities
The current COVID-19 pandemic is an unprecedented and challenging situation for all medical specialties. While most patients with SARS-CoV-2 infection present with respiratory symptoms, cardiovascular manifestations of COVID-19 are also observed in a substantial proportion of patients and are usually associated with poor prognosis [1, 2]. In the cohort of patients hospitalized for COVID-19 in Wuhan, China, approximately twenty percent of all patients had a cardiac injury, but only 3.4% complained of chest pain [1]. Most frequently, myocardial injury in patients with COVID-19 seems to be associated with myocarditis or cytokine storm [1, 2]. Increased risk of developing type 1 myocardial infarction (systemic inflammation predisposes to plaque rupture) and type 2 (related to oxygen supply and demand imbalance) is also possible [1, 3]. Takotsubo syndrome and spontaneous coronary artery dissection have also been observed in patients with SARS-CoV-2 infection [3, 4]. None of these conditions were found; moreover, the diagnostic criteria for acute pericarditis were not met in this case. Therefore we could not state with certainty that there was a causal relationship between either ischemic ECG changes or an episode of chest pain and COVID-19 in this patient. During the COVID-19 pandemic, the management of patients suspected of acute myocardial infarction needs to be careful and responsible, in order to reduce SARS-CoV-2 spread.







