
Introduction
The National Cancer Institute’s definition of immunotherapy refers to any treatment that impulses or restores the capability of the immunological system to fight cancer, infections, or other diseases [1]. To be effective immunotherapy needs to increase the quality or quantity of immune active cells, expose additional tumoral protective antigens (i.e. propagation of the antigen) or inhibit the cancer-induced immunosuppressive mechanisms [2].
Immunology cancer treatment investigation has led to the discovery of regulation points between the interaction of antigen-presenting cells, cytotoxic T or immune-cells, and tumour cells. From these T-cell checkpoints, currently studied are cytotoxic T-lymphocyte antigen 4 (CTLA-4), programmed cell death protein 1 (PD-1), and one of its ligands (PD-L1). This knowledge has allowed the creation of monoclonal antibodies, which block the T-cell checkpoint signalling via CTLA-4 and PD-1 or PD-L1, thereby releasing the brakes on T-cell function and bolstering its cytotoxicity. These antibodies have demonstrated clinically important benefits in tumours like melanoma, lung cancer, renal cell cancer, colon cancer, lymphoma, and bladder cancer. However, there are multiple studies in which the utility of these antibodies is being proved, to determine their activity in other conditions [3, 4].
CTLA-4 was discovered in the early 1980s; it is a member of the immunoglobulin superfamily that acts as a negative immune system regulator and plays a key role in the inhibition of antitumour immunity [5]. PD-1 was discovered in 1992 for its high expression during apoptosis in a T-cell hybridoma model. It is expressed in activated T and B cells and thymocytes [6, 7]. Two ligands have been described: PD-L1 and PD-L2 (also denominated B7-H1 and B7-DC, respectively), both of which are type 1 transmembrane glycoproteins with type IgC and IgV extracellular domains [8]. The expression of PD-L1, both in lymphoid tissues and non-lymphoid tissues, suggests that PD-1/PD-L1 pathway might modulate the immune responses in secondary lymphoid tissues as in end-organs [9–14].
Mexico currently disposes of therapeutic effective agents like monoclonal antibodies vs. PD-1 (nivolumab, pembrolizumab) and CTLA-4 (ipilimumab). In spite of the existence of immune un-blockers against PD-L1 ligand (atezolizumab, durvalumab, avelumab) in Mexico they are only available under investigation protocols. Besides this regulation pathway, the immune profile of an individual depends on multiple factors that include extrinsic circumstances such as the intestinal microbiome, the presence of infections, or exposure to environmental carcinogens, as well as the intrinsic properties of the tumour (genetic composition, cytokines secretion, etc.) [12–17]. In Mexico therapy use was initiated in 2012 with ipilimumab and in 2015 with nivolumab and pembrolizumab. Our institution (Médica Sur) was one of the pioneers in the utilisation of these drugs; thus, it is necessary to know the experience of Médica Sur Hospital to determine the clinical characteristics and adverse effects of patients who used some type of immunotherapy for distinct cancer types.
Material and methods
An observational, descriptive, cross-sectional study was performed on 70 patients of Médica Sur Hospital, who received immunotherapy based in ipilimumab, nivolumab, or pembrolizumab. The principal objective was to learn and determine the most frequent clinical and biochemical adverse effects in a period of 6–12 months. The secondary objective was to settle the response to treatment within the different cancer types. Descriptive statistics were used, involving central and dispersion tendency measures; range, average, median, mode, standard deviation, proportion, and percentages.
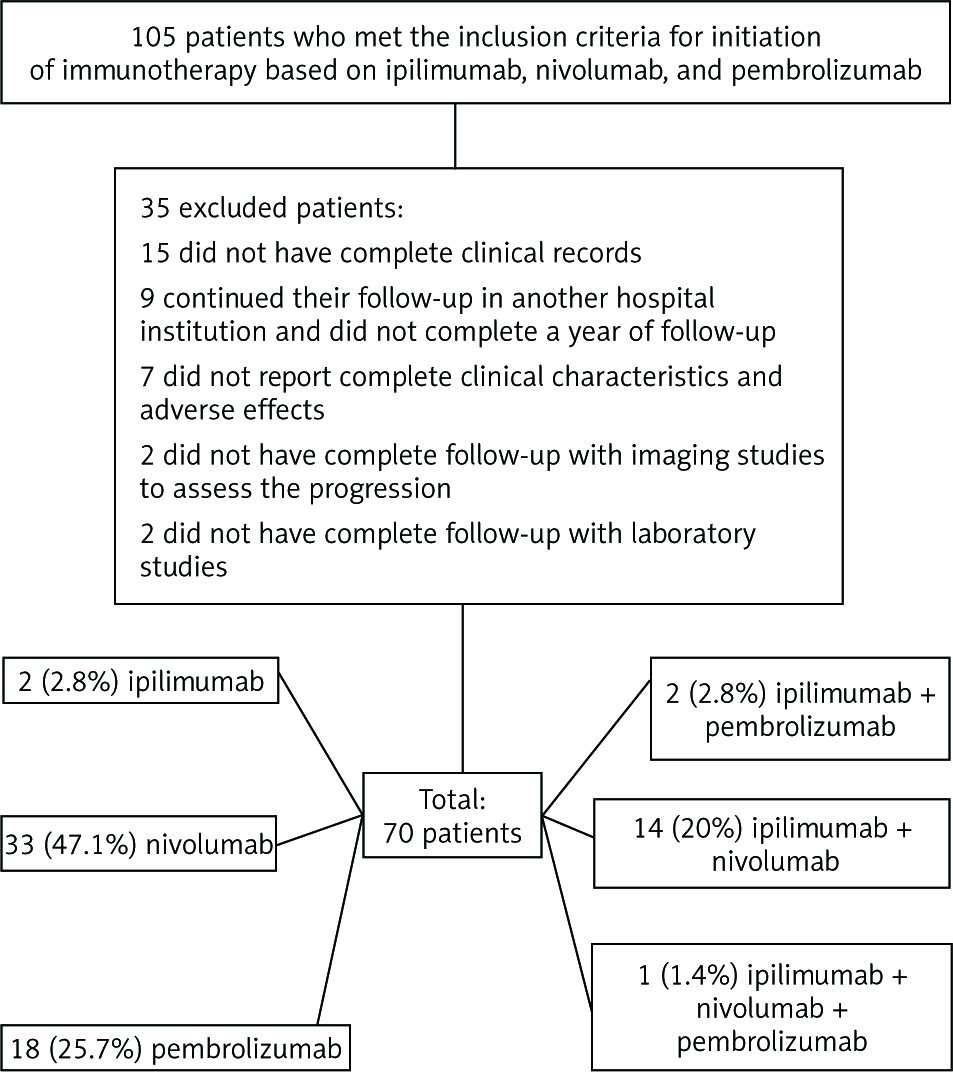
The inclusion criteria including having received treatment with immunotherapy for at least six months for metastatic oncologic disease (lung cancer, renal cancer, melanoma, colon cancer, and bladder cancer); all patients gave written, informed consent that was signed before immunotherapy treatment. Exclusion criteria included having incomplete follow-up by imaging studies and laboratory tests in our institution (Fig. 1).
Results
From a total of 105 patients who were eligible to receive immunotherapy for cancer (based on ipilimumab, nivolumab, and pembrolizumab), 70 (66.6%) patients fulfilled the inclusion criteria established for our study. Two of them (2.8%) received monotherapy with ipilimumab, 33 (47.1%) patients received single nivolumab monotherapy, 18 (25.7%) were treated with pembrolizumab, two (2.8%) received ipilimumab followed by pembrolizumab, 14 (20%) ipilimumab + nivolumab, and one (1.4%) received triple therapy with ipilimumab + nivolumab + pembrolizumab (Fig. 1). Nineteen patients (27.1%) received associated chemotherapy with the immunotherapy.
General characteristics
From the 70 patients included in this study, 42 (60%) were women with an average age of 60.73 ±13.64 years (16–82 years). The average weight was 73.24 ±13.3 kg (45–116 kg). With respect to the Eastern Cooperative Oncology Group (ECOG) scale and validated by the World Health Organisation (WHO) to evaluate the quality of life of patients with cancer, 40 (57.1%) presented an ECOG 0, 26 (37.1%) ECOG 1, three (4.2%) ECOG 2, one (1.4%) ECOG 3, and no patient had ECOG 4.
Regarding to the presented comorbidities that patients had at the beginning of immunotherapy, it was found that 25 (35.7%) did not have any, 28 (40%) had high blood pressure, 18 (25.7%) had type 2 diabetes mellitus, 13 (18.5%) had dyslipidaemia, 3 (4.2%) had ischaemic heart disease, eight (11.4%) had hypothyroidism, eight (11.4%) had chronic obstructive pulmonary disease, one (1.4%) had epilepsy, four (5.7%) had arrhythmias (auricular fibrillation, AV blocks), four (5.7%) had asymptomatic hyperuricaemia, four (5.7%) had benign prostatic hyperplasia, two (2.8%) had stroke, and three (4.2%) had venous thrombosis (PTE/PTV). It is worth mentioning that only 16 patients (22.8%) presented a single comorbidity, 12 (17.1%) two comorbidities, 11 (15.7) three comorbidities, four (5.7%) four comorbidities, and two (2.8%) five comorbidities (Table 1).
Table 1
General characteristics from the study sample
The diseases that received immunotherapy included the following: melanoma – 17 (24.3%), lung adenocarcinoma – 14 (20%), small cell lung cancer – 8 (11.4%), lung epidermoid carcinoma – 5 (7.1%), mesothelioma – 5 (7.1%), epidermoid cancer from the anal canal – 3 (4.3%), clear cell renal cancer – 2 (2.8%), urothelial bladder carcinoma – 2 (2.8%), mucinous appendix adenocarcinoma – 2 (2.8%), epidermoid bladder carcinoma – 1 (1.4%), pelvic leiomyosarcoma – 1 (1.4%), colon adenocarcinoma – 1 (1.4%), gastric adenocarcinoma – 1 (1.4%), gastroesophageal cancer – 1 (1-4%), papillary thyroid cancer – 1 (1.4%), renal adenocarcinoma + prostatic adenocarcinoma – 1 (1–4%), melanoma + lung adenocarcinoma – 1 (1.4%), gallbladder adenocarcinoma – 1 (1.4%), melanoma + lung adenocarcinoma – 1 (1.4%), high-grade osteosarcoma telangiectatic variety – 1 (1.4%), cystic adenoid cancer – 1 (1.4%), epidermoid cervical cancer – 1 (1.4%), and ovarian adenocarcinoma – 1 (1.4%) (Table 2).
Table 2
Pathologies that received immunotherapy
At the beginning of the diagnosis 66 (94.2%) patients had metastatic disease being most frequently at ganglionar level 22 (31%), lung – 14 (20%), bone – 8 (11.4%), liver – 7 (10%), and central nervous system – 5 (7.1%). Of the 70 patients, 45 (64.3%) received surgical treatment associated with their baseline pathology, and 50 (71.4%) subjects received some kind of chemotherapy before immunotherapy.
Concerning mutations, they were only performed in 21 (30%) patients, revealing one (1.4%) positive mutation for KRAS, three (4.2%) positive for EGFR, three (4.2%) positive for BRAF V600E, seven (10%) negative for BRAF V600E, two (2.9%) were negative for EGFR, ALK, and HER2 Neu, one (1.4%) was negative for EGFR, two (2.9%) were negative for BRAF, one (1.4%) was ALK negative, and one (1.4%) was negative for HER2 Neu. A positive PDL-1 was demonstrated in seven (10%) patients.
Initially, before chemotherapy, the functional state ECOG classification was performed for a second time, reporting ECOG 0 – 17 (24.3%), ECOG 1 – 42 (60%), ECOG 2 – 6 (8.6%), ECOG 3 – 3 (4.3%), and ECOG 4 – 2 (2.9%). Within the executed studies, not only made for stratification and disease follow-up but also to corroborate the immunotherapy response to treatment, were the following: axial computed tomography – 46 (65.7%), positron emission tomography – 42 (60%), magnetic resonance – 9 (12.9%), colonoscopy – 3 (4.3%).
As mentioned before, two (2.8%) patients received monotherapy with ipilimumab, 33 (47.1%) with nivolumab, and 18 (25.7%) with pembrolizumab. Combined therapy was applied in 14 (20%) patients with ipilimumab + nivolumab, from which 10 were applied concomitantly and four in a sequential way, two (2.8%) received ipilimumab + pembrolizumab in sequence (first received ipilimumab for melanoma and further nivolumab + pembrolizumab were added in sequence). Nineteen (27.1%) received associated chemotherapy or radiotherapy in spite of immunotherapy: bevacizumab – four (5.7%), radiotherapy – two (2.8%), placlitaxel + cisplatin + bevacizumab – two (2.8%), capecitabine – two (2.8%), etoposide + carboplatin + denosumab – one (1.4%), pemetrexed + oxaliplatin + bevacizumab – one (1.4%), vemurafenib + dabrafenib + trametinib – one (1.4%), interferon – one (1.4%), carboplatin + dacarbazine – one (1.4%), and pemetrexed + carboplatin – one (1.4%) (Table 3).
Table 3
Number of patients according to the applied immuno- therapy
Complications and adverse effects
Fifteen (21.4%) patients presented central nervous system metastasis, from which only one presented it during immunotherapy treatment. Within the manifested complications, the following were presented: cardiac tamponade – two (2.9%), intestinal occlusion – one (1.4%), and haemoptysis – one (1.4%). The clinical and biochemical adverse effects (Table 4) included general effects: fatigue – 32 (42.7%), asthaenia – 30 (42%), adynamia – 28 (40%); gastrointestinal: nausea – eight (11.4%), vomiting – four (5.7%), diarrhoea – eight (11.4%), hyperoxia – eight (11.4%), pancreatitis – one (1.4%), haemorrhagic colitis – one (1.4%); respiratory: pneumonitis – 10 (14.28%), allergic rhinitis – one (1.9%); muscular: myalgias – one (1.4%), endocrinology: hypothyroidism – four (5.71%), hyperglycaemia – one (1.4%), hypophysitis – two (2.9%); skin: rash – seven (10%), pruritus – five (7.14%), vitiligo – two (2.9%), alopecia – one (1.4%); laboratory: TSH elevation – two (2.9%), glucose elevation – one (1.4%), lipase/amylase elevation – one (1.4%), ALT elevation – three (4.28%), AST elevation – three (4.28%), and DHL above superior normal limit – 10 (14.28%). The mean number of days of hospitalisation was 1.27 ±4.48 (0–31 days).
Table 4
Adverse effects
Response to treatment
Speaking of the response to treatment, complete response was presented in seven (10%) patients, from which three (4.28%) were treated with nivolumab, two (2.96%) with pembrolizumab, and two (2.96%) with ipilimumab + nivolumab. Partial response was presented in 11 (15.71%), from which four (5.7%) were treated with nivolumab, one (1.4%) with ipilimumab, one (1.4%) with pembrolizumab, and five (7.14%) with ipilimumab + nivolumab. The disease remained stable in 33 (47.14%), from which one (1.4%) was treated with ipilimumab, 18 (25.71%) with nivolumab, eight (11.4%) with pembrolizumab, and five (7.14%) with ipilimumab + nivolumab. Disease progression was observed in 19 (27.1%); eight patients (11.4%) were treated with nivolumab. Two of them (2.9%) died, one of them had as baseline pathology stage IV lung adenocarcinoma, ECOG 2, and the other one stage IV epithelioid mesothelioma, ECOG 4. Seven patients (10%) progressed with pembrolizumab, and one of them (1.4%) died with stage IV lung adenocarcinoma as baseline pathology, ECOG 3, three (4.2%) with ipilimumab + nivolumab, and one (1.4%) with ipilimumab + pembrolizumab, who died with stage IV malignant melanoma, ECOG 2 (Table 5).
Table 5
Response to treatment according to applied immunotherapy
* two of them (2.9%) deceased, one of themhad as baselinepathologystage IV lungadenocarcinoma, ECOG 2, and the other one stage IV epithelioidmesothelioma, ECOG 4, ** one of them (1.4%) deceased with stage IV, lungadenocarcinoma as baselinepathology, ECOG 3, ***deceased for stage IV malignant melanoma, ECOG 2
Discussion
Since the beginning, two completely human IgG monoclonal antibodies: anti-CTLA-4 – ipilimumab (MDX-010) and tremelimumab (CP-675 206) have been proven as monotherapy also in combination in clinical trials phase II and phase III, since 2001 and 2002 respectively, and it was highlighted that the pattern and duration of the immune response associated with these new modalities differ from those related with cytokines and cytotoxic agents [18, 19].
The earliest positive results with immune checkpoint inhibitors (ICIs) in randomised trials were obtained for metastatic melanoma with ipilimumab; a 2010 published essay demonstrated superiority of ipilimumab as second-line treatment against the comparison pattern based in the gp100 vaccine (average survival of 10.1 and 6.4months, respectively), which permitted its rapid approbation for the regulatory agencies in the US. The approved dosage is 3 mg/kg every three weeks, to complete four applications [20].
The introduction of PD-1 antibodies has its beginning in the evaluation of antitumour activity and the safety of BMS-936558, a specific PD-1 antibody that blocks at a dosage of 0.1–10 mg/kg every two weeks, evaluating the response every eight weeks for the treatment sequence cycle, which produced objective responses in approximately one in every four to one in five patients with small-cell lung cancer, melanoma, or renal cell cancer; the adverse effects profile does not seem to exclude its use [10].
The effectiveness and activity of antibody against PD-L1 (BMS-936559) was validated from a phase I multicentric trial in which durable tumour regression was reported (objective response rate of 6 to 17%) and prolonged stability of the disease (rate from 12% to 41% at 24 weeks) in patients with advanced cancer, including non-small cell lung cancer, melanoma, and renal cell cancer [21].
By virtue of the great reported global survival of metastatic melanoma, the FDA approved the monoclonal antibody vs. CTLA-4 (ipilimumab) in March of 2011, and then approved the humanised monoclonal antibody against PD-1 (pembrolizumab) and PD-1 (nivolumab) in September and December of 2014, respectively [20, 22–24]. A year later the FDA approved the combination (ipilimumab + nivolumab) in a phase III trial (CheckMate 067) for presentation of free survival progression evidence in metastatic melanoma [25–27], and utility of ipilimumab as surgically resectable melanoma treatment was restated [28]. In 2017 (KEYNOTE-006) the multicentric, randomised phase III trial assigned patients in a 1 : 1 : 1 ratio (pembrolizumab every two and three weeks or ipilimumab every three weeks) demonstrating that pembrolizumab maintained its superiority in relation to disease-free and global survival of 28–31% to 24 months vs. 14% with ipilimumab [29]. It should be noted that in the KEYNOTE-001 trial the optimal treatment duration controversy emerges as with a short pembrolizumab treatment it was observed a prolonged complete response after suspension of the treatment [30]. Also, a combination at standard dose of ipilimumab + pembrolizumab was applied in low dosage in a phase I trial (KEYNOTE 0-29), in which increased rates of response and survival improvement were highlighted as being better than with monotherapy, whereby higher rates of toxicity were presented [31].
In 2015 immunotherapy gained great importance in lung cancer due to the approbation of nivolumab in the CheckMate 017 trial, not only for presenting global survival evidence of 9.2 months and best response up to 20%, but also progression-free survival of 3.5 months and lower adverse effect rates of 7%, in comparison with docetaxel as a second-line treatment for non-small cell squamous lung cancer [32]. In the same year, efficacy was proven as a second-line treatment in non-microcytic lung cancer stage IV (non-squamous, adenocarcinoma) over nivolumab, improved response rate of 19%, with a higher global survival of 12.2 months and fewer adverse effects (10%) in comparison with docetaxel in the CheckMate 057 trial [33].
Pembrolizumab also achieves great results in global survival of up to 10.4–12.7 months and fewer adverse effects, at 13-16%, in comparison with docetaxel as second-line treatment for non-small cell stage IV lung cancer with positive PD-L1 in < 50% in the KEYNOTE-010 trial [34]. The last OAK multicentric, randomised, controlled, phase III trial demonstrated improvement in the progression-free survival as globally as with the response rate and less adverse effects with atezolizumab in comparison to docetaxel as second-line treatment in non-small cell lung cancer [35].
In a phase I trial nivolumab at dose of 3 mg/kg every two weeks demonstrated an objective response of 23% and 28% in patients who presented PD-L1 biomarker, with an average global survival of 19.4 months and 19% of serious effects in non-small cell lung cancer [36].
In the KEYNOTE-024 trial, pembrolizumab vs. chemotherapy based on platins for microcytic lung cancer with PD-L1 expression in more than 50% of the tumour cells, it was shown than pembrolizumab had a better response rate in 44.8%, higher progression-free survival of 10.3 months, global survival of 80.2 months, and fewer adverse effects in 26.6%, a pattern that led to incorporating pembrolizumab in the NCCN guides (Version 3.2017) as first-line treatment in patients who fulfil those criteria [37]. In another randomised trial, CheckMate 026, nivolumab was compared with standard platin chemotherapy in non-microcytic lung cancer with PD-L1 expression of at least 1%. As first-line treatment, there was no meaningful superiority for nivolumab and just fewer adverse effects were corroborated as serious 18% [38].
Likewise, there are two assays in which combination of immunotherapy and chemotherapy is valuated: CheckMate 012 (nivolumab at different dosage + chemotherapy based in platins), in which objective responses are observed in 47% and a global two-year survival of 62% [39]. In another trial (KEYNOTE 021) pembrolizumab + QT (carboplatin + pemetrexed) was compared with the same pattern of isolated QT; both arms further received maintenance pemetrexed. The response rates were favourable in 55% due to combination and with similar frequency of serious adverse effects [40].
In a phase III trial that combined platins + etoposide and ipilimumab for microcytic stage IV lung cancer, a discrete improvement was shown in disease-free survival; however, the said combination did not overcome the pattern of isolated chemotherapy [41]. At the end of 2016 CheckMate 032 a comparison was performed between ipilimumab + nivolumab vs. single nivolumab, denoting that the combination of both immunotherapies gave better objective responses in 10–19% with acceptable toxicity in patients with microcytic lung cancer recurrence within six months after first treatment, a pattern which marked the incorporation of this treatment to the NCCN (Version 3.2017) [42].
Recently, in 2015 November, the FDA approved nivolumab for presenting evidence of global survival in renal cell carcinoma as second-line treatment compared to everolimus [43]. Also, promising results were obtained with nivolumab in a phase I trial [44] that included 23 patients with refractory or recurrent Hodgkin’s classic lymphoma. An objective response rate of 87% was obtained and none of the patients showed disease progression during nivolumab therapy. Pembrolizumab is active in other solid tumours, such as lung, head, neck, triple-negative breast cancer, and renal cell carcinoma [25].
Immune checkpoint inhibitors (ICIs) were included in clinical practice as a second-line option after an initial chemotherapy regimen, and in the last year positive results have been reported from randomised trials in which they were compared in the first line with standard chemotherapy. Responses have been surprising and durable, but less than 20–25% in unselected patients, so it is essential that factors predicting efficacy be identified. One such biomarker is PD-L1, but the different methods used to detect it have produced mixed results [45].
The precise pathophysiology of ICI-mediated immune-related adverse effects (irAES) is currently unknown. Some research shows that irAES may result from some combination of autoreactive T cells, autoantibodies, and/or proinflammatory cytokines. The adverse effects are no-irAES or irAES. The early- and later-onset irAES may result from distinct mechanisms that have yet to be elucidated. Typical earlier-onset, common irAES appears to involve generalised epithelial inflammation and may be observed in the form of rash, colitis, and pneumonitis. Later-onset irAES, which is typically less common, can include neurologic events and hypophysitis, among others [46].
In our study, any degree of irAES was generally reported in 50 (71.4%) patients, in 10 (14.2%) of whom it was high grade. The reported incidence of any-grade irAES associated with single-agent ICI treatment ranges widely across agents and trials, from approximately 15 to 90%. With anti-CTLA-4 antibodies (ipilimumab), the overall incidence of any-grade irAES is 72%, and 24% for high-grade irAES [20, 47].
A randomised, double-blind, phase III trial in patients with unresectable or metastatic melanoma revealed a dose-dependent effect in treatment-related AEs for patients receiving ipilimumab at a dose of 3 mg/kg (n = 362) or 10 mg/kg (n = 364). The most common irAES was rash (13–15%), pruritus (22%), diarrhoea (17–27%), and fatigue (10%). High-grade irAES was reported in 18% and 30% of the 3 mg/kg and 10 mg/kg treatment groups, respectively. The most common high-grade AEs, including diarrhoea (6–10%), colitis (2–5%), elevated liver enzymes (2%), and hypophysitis (2%), were all more common at the higher dose of ipilimumab [48]. We reported rash (10%) and pruritus (7.1%) much less frequently than that reported in the literature. Our results are similar to this study with respect to grade 3 irAES except for colitis (1.4%) and diarrhoea (2.9%), which occurred less frequently.
The incidence of any-grade irAES associated with anti-PD-1/PD-L1 bodies was reported in 27–30%, and in 5–8% for high-grade irAES. The most commonly observed AES were dermatology (vitiligo in relation with melanoma) and gastrointestinal (colitis), followed by endocrine (hypothyroidism, hepatic (elevated liver enzymes), and pneumonitis (5–6.7%) events [46–49].
De Velasco et al. recently reported on the incidence of the most common immune checkpoint inhibitor (ICI)-associated irAES in a meta-analysis of 21 randomised phase II/III trials conducted from 1996 to 2016, which included a total of 6528 patients who received monotherapy (atezolizumab, n = 751; ipilimumab, n = 721; nivolumab, n = 1534; pembrolizumab, n = 1522) and 4926 patients in placebo or standard therapy control arms using chemotherapy or biologic agents. When compared to patients in the trial control arms, patients receiving ICIs were found to be at greater risk for any-grade immune-related colitis, AST elevation, rash, hypothyroidism, and pneumonitis. Within this cohort, across all ICIs, the incidence of grade 3/4 events was 1.5% for colitis, 1.5% for liver toxicity, 1.1% for rash, 0.3% for hypothyroidism, and 1.1% for pneumonitis. High-grade colitis and rash were significantly more common among patients on ipilimumab than in those receiving PD-1/PD-L1 inhibitor [50].
A 2018 meta-analysis compared the data on toxicity profiles of PD-1 and PD-L1 inhibitors from 23 studies that occurred between 2013 and 2016 (PD-1, n = 3284; PD-L1, n = 2460).A near-significant trend revealed irAES to be more common with PD-1 vs. PD-L1 blockade (16% vs. 11%; p = 0.07). However, the incidence of severe irAES was not significantly different between PD-L1 and PD-1 inhibitors, (5% vs. 3%, p = 0.4). Pneumonitis occurred twice as often with PD-1 inhibitors (4% vs. 2%; p = 0.01), and hypothyroidism was also more common with PD-1 inhibitors (6.7% vs. 4.2%; p = 0.07) [51].
The combination of CTLA-4 and PD-1/PD-L1 blockade has only been approved for patients with metastatic melanoma. Treatment-related irAES were observed in 95% of patients. In 55% of patients these irAES were of grade 3 or higher [49].
It is worth mentioning that the most frequent adverse effects were the general symptoms (asthaenia, fatigue, adynamia, gastrointestinal [nausea, diarrhoea, and hyporexia] and skin manifestations such as rash and pruritus); however, the adverse effects with major impact in tolerance, follow-up, hospital stay, and mortality related to immunotherapy were pneumonitis, hypothyroidism, hypophysitis, type 1 diabetes, and haemorrhagic colitis. We observed an incidence of pneumonitis in our population almost 2–4 times higher than that in previously published reports in a Caucasian population (pneumonitis 2.6 to 6.7%) [49]. Three cases (4.28%) were classified as high-grade pneumonitis (grade 3), and only two (2.85%) patients had received chest radiotherapy before and during immunotherapy. One of the probable causes of pneumonitis in this group of patients was the presence of lung damage related to tumour burden, exposure to smoking, and the presence of chronic obstructive pulmonary disease or fibrosis.
Pneumonitis associated with checkpoint blockade is a toxicity of variable onset and clinical, radiological, and pathological appearance, which has been observed with anti-PD-1/PD-L1 monoclonal antibodies (MoAbs) and, more rarely, with anti-CTLA-4 MoAbs. It is more common when anti-PD-1/PD-L1 MoAbs are combined with anti-CTLA-4 MoAbs. Several cases of distinct life-threatening respiratory events have been reported under anti-CTLA-4 monotherapy. Acute interstitial pneumonitis/diffuse alveolar damage syndrome (DADS) is the most acute, life-threatening event. Patients with a history of autoimmune disease or who are being actively treated for an autoimmune disease are at risk for worsening of their autoimmune disease while on immune checkpoint blockade. Similarly, patients that have had irAES on ipilimumab are at risk of developing irAES following anti-PD-1 treatment and vice versa. Results from these retrospective series showed a higher rate of grade 3 to 4 toxicity in patients treated with ipilimumab following anti-PD-1 (up to 35%), and patients with grade 3 to 4 toxicity on ipilimumab followed by anti-PD-1 developed grade 3 to 4 irAES in > 20% of cases. The pneumonitis associated with radiotherapy is very frequent, so it is also important to avoid the combination of immunotherapy and radiotherapy, especially mediastinum [47, 50, 51].
It is remarkable that laboratory-reported alterations allowed us to come after the pattern with follow-up studies of thyroid profile to discard hypothyroidism, fast glucose levels to discard type 2 diabetes mellitus, liver function proofs to monitor the values or increases of liver enzymes as ALT and AST, as well as lipase/amylase to evaluate pancreatitis risk, and also imaging studies like cranial TAC/MRI to discard hypophysitis, X-ray/thoracic TAC to discard pneumonitis, and colonoscopy in suspicion of haemorrhagic colitis; all of these correlated with clinical patient symptoms.
Conclusions
Immunotherapy based in ipilimumab, nivolumab, and pembrolizumab is a better combined therapy either with surgery or with chemotherapy in patients with metastatic diseases in clinical stage IV, with recurrence or bad response to baseline treatments in different types of cancer, mostly in melanoma and lung cancer. The most frequent adverse effects generally do not conditionate the suspension of treatment nor hospital-stay prolongation; however, there are some adverse effects that actually have an impact in evolution, hospital-stay, and mortality, such as pneumonitis, hypophysitis, type 1 diabetes mellitus, and haemorrhagic colitis. Hence, it is imperative to obtain a precise image and perform routine biochemical follow-up.






