
Introduction
Acute-on-chronic liver failure (ACLF) is a condition marked by the development of one or more organ failures (OFs), with significant short-term mortality (> 15%), and intense systemic inflammation in patients with an acute decompensation (AD) of cirrhosis. Acute decompensation of cirrhosis, which is characterized by the recent development of gastrointestinal haemorrhage, bacterial infection, ascites, hepatic encephalopathy, or any combination of these disorders, is the main cause of hospitalization in cirrhotic patients [1]. ACLF is precipitated in many patients by an acute event, which can be intrahepatic, such as reactivation of hepatitis B virus (HBV) or alcohol intake, or extrahepatic, such as bacterial infections or upper gastrointestinal bleeding. However, no precipitating factor can be identified in up to 40% of patients with ACLF [2].
Until now, there is no consensus definition for ACLF. The most widely studied definition was the European one suggested by the European Association for the Study of the Liver-Chronic Liver Failure (EASL-CLIF) consortium, and hence most data about ACLFwere established from studies based on it [3]. A recent meta-analysis performed on 43,206 ACLF patients derived from 30 studies using the EASL-CLIF ACLF criteria to study the epidemiological features of ACLF showed that the worldwide prevalence and 90-day mortality rate of ACLF were 35%, and 58% respectively, and they differ according to geographical location. The most frequently documented aetiology of liver disease was alcohol; however, regional variations in the rates of alcohol intake were also reported. Infection and gastrointestinal bleeding were the most frequent triggers (35% and 22%, respectively). The most frequent organ failure reported was kidney failure (49%), while respiratory failure was the least frequent (11%) [4].
In up to half of cases, ACLF can improve or even completely resolve, but in the other half, disease progression may result in a life-threatening condition [5]. Early identification of predictors of short-term mortality in ACLF is crucial due to the high mortality rate, to identify patients at risk who will require intensive care management, specific treatments, or emergency liver transplantation [6].
Although ACLF is increasingly being recognized as a distinct condition, most research has been conducted on American, European, and Asian cohorts, where alcoholic and chronic HBV aetiology of liver disease predominates. Few studies from the Middle East, including Egypt, have addressed the patterns of ACLF, where hepatitis C virus (HCV) is the major cause of chronic liver disease [6-9]. Therefore, we conducted our study to shed some light on this syndrome. We aimed to identify the 28-day mortality rate and its predictors in decompensated cirrhotic patients with ACLF and to identify the pattern of ACLF in these patients.
Material and methods
Patients
This prospective observational study was conducted in the Tropical Medicine and Gastroenterology Department, Sohag University Hospitals, Sohag, Egypt, between March 2021 and February 2022. The study protocol was approved by the Medical Research Ethics Committee (MREC) of the Sohag Faculty of Medicine (number: Soh-Med-21-02-12), ClinicalTrials.gov (ID: NCT04790435). Informed written consent was obtained from all participants or their relatives (for comatose patients) before enrolment.
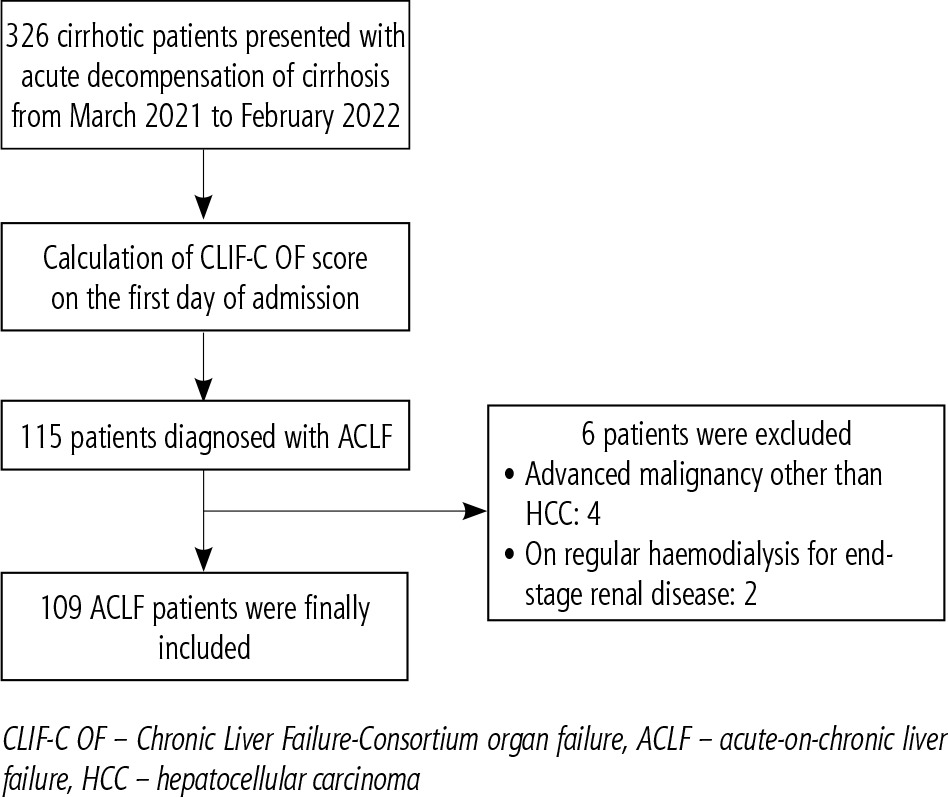
A total of 326 cirrhotic patients (201 males, 125 females) who presented with AD of cirrhosis were evaluated for the presence of ACLF based on the EASLCLIF criteria. As a result, 115 patients with ACLF were enrolled in the study. In all, 4 patients were excluded from the study because they were diagnosed with advanced malignancy other than hepatocellular carcinoma (HCC). Two other patients with ACLF were excluded because they were on regular haemodialysis for end-stage renal disease. In total, 109 patients (33.44%) were finally included after fulfilling the study eligibility criteria (Fig. 1).
We used the European definition as it is the most widely studied one based on the results of the CANONIC study [2]. Organ failures were defined based on the Chronic Liver Failure-Consortium Organ Failure (CLIF-C OF) scoring system, which is based on the original Sequential Organ Failure Assessment (SOFA) score that evaluates six organ systems (kidney, liver, coagulation, brain, circulation, and respiration). Based on how many OFs they had, patients were classified into grades 1, 2, and 3, if they had single, two, or ≥ three OFs, respectively. The diagnosis of ACLF grade 1 was established by one of the following conditions: single renal failure; a single cerebral failure which is associated with a creatinine level in the range 1.5-1.9 mg/dl, as well as a single hepatic, circulatory, coagulation, or respiratory failure all associated with a creatinine level in the range 1.5-1.9 mg/dl and/or mild to moderate hepatic encephalopathy [2].
We excluded patients with no ACLF; acute liver failure; end-stage renal disease on regular haemodialysis; previous liver and/or renal transplant; malignancies other than HCC; and extrahepatic cholestasis.
Methods
All patients underwent a complete medical history and clinical examination. Abdominal ultrasonography was performed and a triphasic computed tomography (CT) scan was done if a heterogenous liver or hepatic focal lesion was detected on ultrasonography to establish the diagnosis of HCC. Liver function tests, prothrombin time (PT) and concentration (PC), international normalization ratio (INR), serum creatinine, complete blood count (CBC), serum sodium and potassium, arterial blood gases, and serology for viral hepatitis (HCV antibodies, hepatitis B surface antigen [HBsAg]) were performed for all patients at admission. An ascitic fluid study was done for all ascitic patients to exclude spontaneous bacterial peritonitis (SBP).
The following scores were calculated:
Child-Turcotte-Pugh (CTP) score: it was based on hepatic encephalopathy, ascites, and serum levels of bilirubin, albumin, and prothrombin time/INR [10].
Model for end-stage liver disease sodium corrected (MELD-Na+): by addition of serum sodium to the original MELD. The following formula was used: MELD-Na+ = MELD score – Na+ – [0.025 × MELD × (140 – Na+)] + 140 [11].
Chronic Liver Failure-Consortium Organ Failure (CLIF-C OF) score: for determination of the grade of ACLF and type and number of OFs [3].
Acute-on-chronic liver failure (CLIF-C-ACLF) score: it was calculated by addition of age and white blood cell count to the CLIF-C OF score. It is calculated according to the following formula: CLIF-C-ACLF score = 10 × [0.33 × CLIF-C OF Score + 0.04 × age, years + 0.063 × ln (WBC count, 109 cells/l) – 2. Both CLIF-C-ACLF and CLIF-C OF scores were calculated online using the website www.efclif.com [12].
All patients underwent 28 days of follow-up from the day of admission to assess the mortality rate.
Statistical analysis
STATA Intercooled program Version 16 was used to analyse the data. The mean and standard deviation or median and range were used to represent quantitative data. If the data were normally distributed, the ANOVA test was used with the Bonferroni post hoc test; otherwise, if the data were not normally distributed the Kruskal-Wallis rank test and Mann-Whitney test were used. The chi-square (χ2) test or Fisher’s exact test was used to compare qualitative data which were presented as numbers and percentages. The Kaplan-Meier plot was applied for survival analysis. To identify the variables influencing survival, univariate and multivariate Cox regression analyses were performed. Excel or the STATA program was used to create the graphs. The p-value was considered significant if it was < 0.05.
Results
Baseline characteristics of the studied population
The baseline demographic and clinical characteristics of the studied patients are presented in Table 1. A total of 109 ACLF patients were included, of whom 29 (26.61%) patients were ACLF-1, 39 (35.78%) ACLF-2, and 41 (37.61%) ACLF-3. The mean age was 63.61 ±11.15 years (range 14-90), and males comprised 65.14% of the study cohort. HCV was the main aetiology of cirrhosis in our patients (80.73%) and across different ACLF grades with no statistical significance.
Table 1
Baseline demographic and clinical characteristics of the studied patients
Hepatic encephalopathy was the major presenting complication of cirrhosis among the studied patients (79.82%), followed by ascites (77.06%), jaundice (68.52%), HCC (41.28%), and upper gastrointestinal bleeding (33.03%). Hepatic encephalopathy, jaundice, and ascites occurred significantly more in ACLF-3 compared to ACLF-1 and 2, while hepatorenal syndrome was significantly lower in ACLF-1 compared to ACLF-2 and 3. No statistically significant difference existed between the various ACLF grades regarding upper gastrointestinal bleeding, HCC, and SBP.
Upper gastrointestinal bleeding (UGIB) and bacterial infections were the triggers of ACLF in 52.29% of cases. However, in 47.71% of cases, no potential trigger was identified. Patients with ACLF-1 had a higher rate of bacterial infections than those with ACLF-2 and 3 (34.48% for ACLF-1, compared to 15.38% and 24.39% for ACLF-2 and ACLF-3, respectively), but without statistical significance.
Renal failure was the most prevalent (73.39%) organ failure, followed by brain (56.88%), circulatory (44.95%), and hepatic (29.36%) failures. Renal failure predominates across different ACLF grades (51.72%, 71.79%, and 90.24% for ACLF grades 1, 2, and 3, respectively), followed by cerebral (31.03%), and hepatic (10.34%) failures in ACLF-1 patients; circulatory (51.28%) and cerebral failures (48.72%) in ACLF-2 patients; and cerebral (82.93%) and circulatory (65.85%) failures in ACLF-3 patients. Renal, cerebral, hepatic, and coagulation failures occur significantly more in ACLF-3 patients compared to ACLF-1 and 2 patients, while circulatory failure was much less frequent in ACLF-1 patients compared to ACLF-2 and 3. Respiratory failure shows no significant difference across different ACLF grades.
Laboratory results and calculated scores of the studied patients are shown in Table 2. As expected, as the grade of ACLF increased patients had more advanced liver disease (Child, and MELD-Na+ scores), more organ failures, higher levels of creatinine, total bilirubin, INR, and median ALT, and lower serum albumin levels and pH.
Table 2
Laboratory results and calculated scores of the studied patients
Antiviral treatment
Out of 95 patients who presented with viral aetiology of cirrhosis, 81 patients (85.26%) received antiviral treatment for either HCV, HBV, or both following the Egyptian National Committee for Control of Viral Hepatitis (NCCVH) protocol. Patients with HCV received a 12-week course of either sofosbuvir/daclatasvir or sofosbuvir/daclatasvir/ribavirin upon diagnosis of HCV (Supplementary Table 2). Cirrhotic patients with HBV were treated with lifelong entecavir, while those with HBV/HCV coinfection received treatment following the same rules as in patients with HBV or HCV mono-infection [13]. The remaining 14 patients (14.74%) did not receive antiviral therapy, as they had recently been diagnosed with cirrhosis during the study. The mean time between starting antiviral therapy and development of ACLF was 30.91 ±12.1 months, being longer in ACLF-1 patients compared to those with ACLF-2 and 3 but without statistical significance.
Predictors of ACLF mortality at 28 days
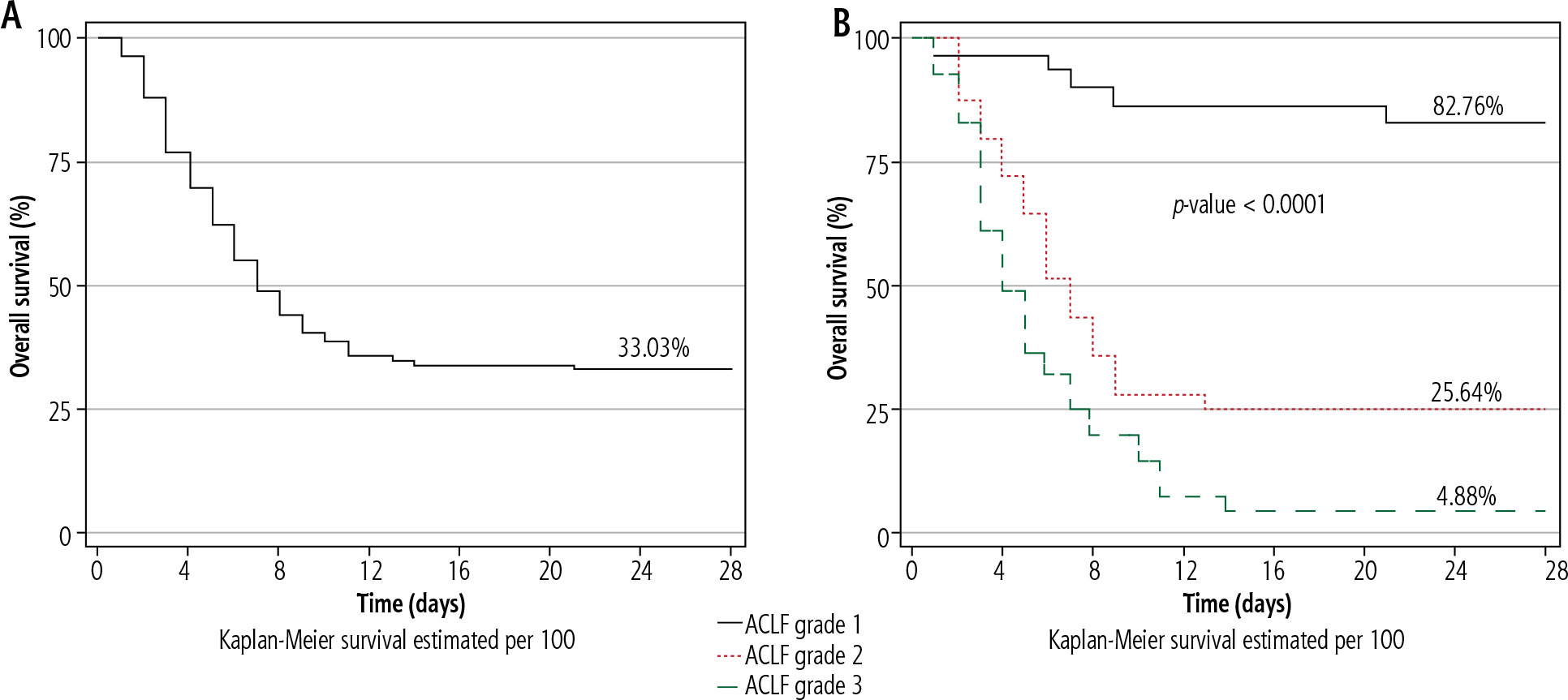
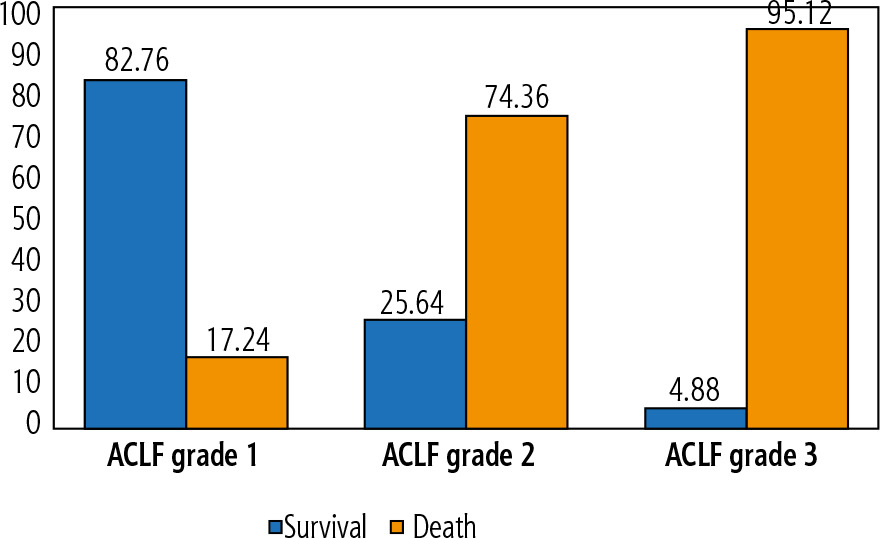
Patients were followed up for a maximum of 28 days or until death. In total, 73 patients (66.97%) died during the 28-day follow-up period (Fig. 2A), and the rate of mortality is directly proportional to the grade of ACLF with statistical significance (17.24%, 74.36%, and 95.12% for ACLF grades 1, 2, and 3, respectively; p < 0.0001) (Figs. 2B and 3). The mean time to death was 5.53 ±3.5 days and become shorter as the grade of ACLF increased but without a statistically significant difference between ACLF grades (p = 0.34).
Fig. 2
Kaplan-Meier plots demonstrating the possibility of overall survival at 28 days: A) All ACLF patients. B) According to the grade of ACLF
On univariate Cox regression analysis (Supplementary Table 1), the presence of hepatic encephalopathy, jaundice, HCC, organ failures (hepatic, coagulation, cerebral and circulatory), ACLF grades 2 and 3, Child class C, high CLIF-C-ACLF, and MELD-Na+ scores, elevated INR, and total bilirubin were significantly associated with 28-day mortality. On the other hand, shifting blood pH to the normal range was significantly associated with a decreased mortality risk. When these significant factors in univariate analysis were entered into the multivariate Cox regression model (Table 3), hepatic encephalopathy, ACLF grades 2 and 3, CLIF-C-ACLF score, total bilirubin, and blood pH were independent predictors for mortality at 28 days.
Table 3
Multivariate and final Cox regression analysis of factors affecting survival
The final Cox regression analysis (Table 3) was applied to the significant factors in the multivariate model and confirmed that the presence of hepatic encephalopathy (HR = 2.96, 95% CI: 1.27-6.94, p = 0.01), ACLF-2 (HR = 6.99, 95% CI: 2.68-18.25, p < 0.0001), and ACLF-3 (HR = 9.34, 95% CI: 3.60-24.74, p < 0.0001) compared with ACLF-1, and elevated total bilirubin (HR = 1.03, 95% CI: 1.00-1.06, p = 0.04), were the most significant predictors for 28-day mortality. On the other hand, shifting blood pH to the normal range was associated with a decrease in the HR of ACLF mortality (HR = 0.03, 95% CI: 0.002-0.44, p = 0.01).
Discussion
Acute-on-chronic liver failure is a major complication that carries a dismal prognosis and is associated with very high short-term mortality in patients with AD of liver disease. Identification of predictors of mortality is crucial to define patients who are in urgent need of intensive care management or emergency liver transplantation [2]. In the current study, we investigated the characteristics and predictors of mortality in patients with ACLF at 28 days.
In this study, the prevalence of ACLF in patients admitted with AD of cirrhosis was 33.44% in one year a frequency slightly higher than that observed by the CANONIC study (30.9%) [2]. Studies conducted in different populations but using the European definition show similar prevalence levels [14-18]. It should be highlighted that based on the definition employed, different studies show different prevalence rates for ACLF [17, 19].
The mean age of ACLF patients in our study was 63.61 ±11.15 years with a median age of 65 years, which was comparable to that reported by Hernaez et al. [17], who noted that the median age of their ACLF patients was 62.31 years, and Dominguez et al. [14], who reported a mean age of 60 ±11 years. However, our cohort was older than that reported by several studies including the CANONIC study [6, 9, 18, 20]. Most of our ACLF patients were males (65.14%), and this coincides with most reports [6, 9, 14, 18, 20, 21]. This male predominance could be attributed to the increased prevalence of known aetiologies of cirrhosis (e.g., viral hepatitis) and hence ACLF among men.
In our cohort, 80.73% of patients had HCV as an underlying cause of their liver disease. Our findings are consistent with those of several studies conducted in Egypt, where HCV was the major cause of liver disease [6, 9, 22]. Egypt had the highest prevalence of HCV infection worldwide [22]; however, recently, a lower percentage of HCV prevalence (4.6%) was observed following the implementation of several national programmes to reduce HCV infection with the use of direct-acting antivirals (DAAs) [13]. Reports from the Western world revealed that alcohol followed by HCV were the main causes of chronic liver disease [2, 14, 17, 20], while HBV was the main cause in most Asian countries [15, 16, 21]. So, the aetiology of liver disease varies according to geographical location.
Contrary to prior studies [6, 9, 14, 17, 18], we found that UGIB was the most common trigger of ACLF (25.69%), followed by bacterial infections (23.85%). The higher incidence of UGIB in our cohort could be attributed to the higher prevalence of HCC (41.28%) and portal vein thrombosis (31.19% of all ACLF patients and 62.22% of HCC patients). Moreover, patients’ noncompliance with portal pressure-lowering drugs and variceal therapeutic endoscopies may be a contributing factor [6]. On the other hand, the higher incidence of bacterial infections reported in previous studies from European and American cohorts can be explained partly by the predominance of active alcoholism. Multiple abnormalities in the adaptive and innate immune systems of individuals with alcoholic liver disease make them vulnerable to infection. It is noteworthy that infection is not included in the Asia-Pacific Association for the Study of Liver (APASL) definition as a trigger of ACLF, so data about bacterial infections are lacking from several parts of Asia [23]. No trigger of ACLF could be identified in 47.71% of cases, which is higher than in previous reports (20-45%) [2, 6, 14, 24]. The inability of the testing methodology or existing diagnostic tools to detect infection or drug-induced liver injury (DILI) could be a possible reason for the failure to detect a triggering factor in ACLF. Additionally, damage-associated molecular patterns (DAMPs) emerging from damaged hepatocytes or bacterial products produced from bacterial translocation may help to clarify the mechanisms of inflammation in ACLF without a clinically apparent precipitating event [1].
One of the major features of ACLF is the presence of organ failures, either single or multiple, which is variable among different studies in terms of type and frequency. Here we observed that the most frequent organ failure was renal (73.39%), followed by cerebral (56.88%), circulatory (44.95%), and hepatic (29.36%); moreover, renal failure predominates in all ACLF grades. Kidney failure is the most prevalent OF, according to previous studies using the European criteria of ACLF, while liver failure is much less frequent, which could be attributed to the extremely rigorous liver OF criteria (total bilirubin > 12 mg/dl) and the overly permissive kidney OF criteria [19]. In contrast to previous research, the prevalence of respiratory failure in our patients was extremely low. However, this may be under-estimated as patients with respiratory failure are usually admitted to intensive care units with mechanical ventilation from the start.
We observed that the 28-day mortality rate was 66.97%, and it is directly proportional to the grade of ACLF, which is consistent with the findings of Verdelho et al. [20] (68.97%) and Dominguez et al. [14] (62.1%). Several studies have reported lower mortality rates than ours, ranging from 25.52% to 48.66% [2, 17, 21, 24]. Reports from Egypt show much higher figures, ranging from 74.3% to 100% [6-9]. The high 28-day mortality rate in our cohort might be attributed to several factors. First, 73.39% of the patients had ACLF-2 and 3, which were associated with higher mortality than ACLF-1. Second, most patients had HCV as an underlying cause of their liver disease; Mahmud et al. [19] concluded that patients with HCV had the highest short-term mortality. The third factor is the difficult implementation of liver transplantation in our cohort of patients, and the lack of an artificial liver support system (ALSS) in our centre. However, ACLF is now well recognized as a reversible process, and the implementation of a proper management protocol for these patients in our centre may reduce overall mortality [12].
To address predictors of 28-day mortality among ACLF patients, a Cox regression analysis was carried out. The final multivariate Cox regression analysis revealed that the presence of 2 or more organ failures, hepatic encephalopathy, elevated total bilirubin, and low blood pH were the most significant independent predictors of 28-day mortality. Several studies have been conducted to investigate factors that predict short-term mortality amongst ACLF patients, with variable results. It is now well established that the existence and the number of OFs as identified with the CLIF-C OF score are strongly linked with 28-day mortality [2, 17, 25]. Furthermore, compared to liver-specific prognostic scores (Child-Pugh, MELD, and MELD-Na+ scores), the CLIF-C-ACLF score was much more efficient in predicting 28-day mortality, as it considers the extrahepatic OFs, which have an important impact on ACLF mortality [26]. Contrary to our results, Méndez-Guerrero et al. [25] recently demonstrated that the type of organ failure per se can predict ACLF mortality, where renal and cerebral failures were independently predictive of 28- and 90-day mortality and strongly associated with higher mortality.
Previous reports support our findings and reveal that hepatic encephalopathy [21, 24, 27] and elevated serum total bilirubin [27, 28] can predict ACLF mortality. Total bilirubin is an important element in liver-specific prognostic scores and is used to define liver failure in ACLF, so it is plausibly associated with ACLF mortality [28]. Drolz et al. [29] demonstrated that metabolic acidosis and acidaemia were independently predictive of mortality at 28 days, which matched our findings. We did not find any role for triggers of ACLF to influence mortality, which agrees with previous research [2, 30]. The main limitations of our study were the short-term follow-up period and that it was a single-centre study.
Conclusions
Acute-on-chronic liver failure is a common condition in our centre among patients with AD of cirrhosis with male predominance and very high mortality at 28 days. The presence of 2 or more OFs, hepatic encephalopathy, elevated serum bilirubin, and low blood pH were the most significant independent predictors of 28-day mortality in our cohort. Due to the potential reversibility of ACLF, it is crucial to identify and diagnose the condition early for proper management and early referral to a liver transplant facility, which could reduce such high mortality.





