
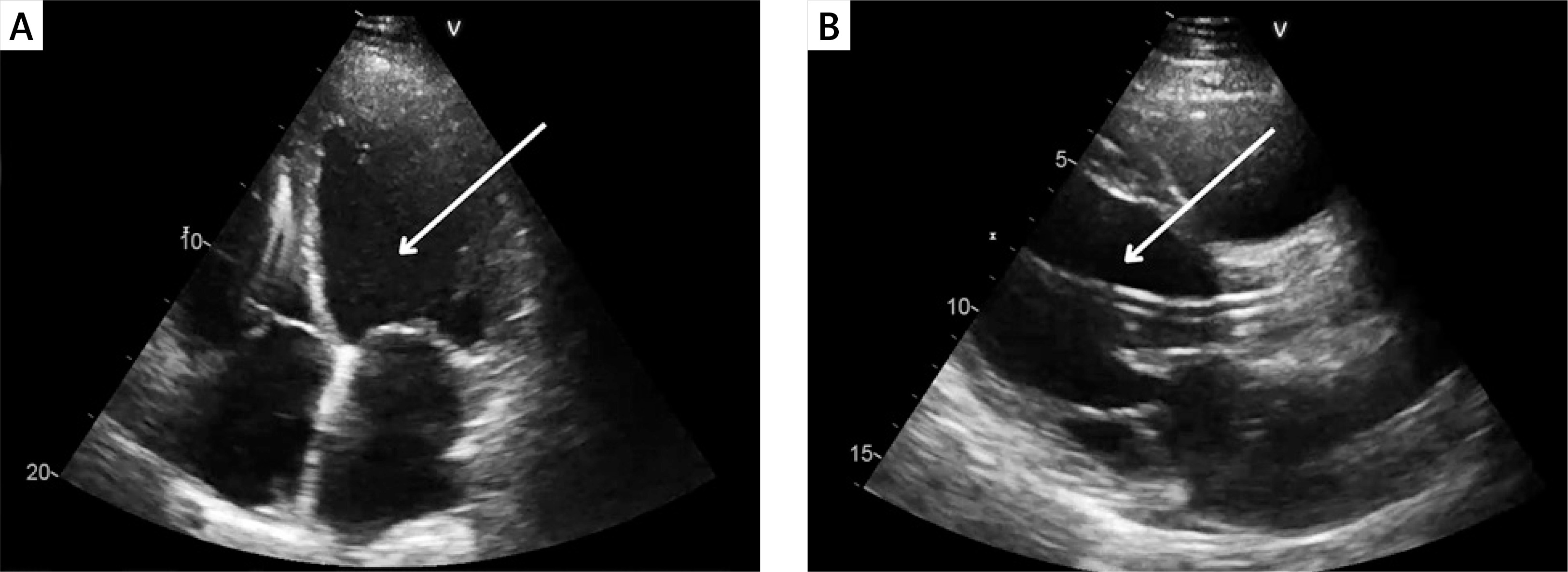
A 51-year-old male with a history of dilated cardiomyopathy, atrial fibrillation, diabetes and cardiac resynchronization therapy was admitted to the cardiology department due to another episode of decompensation of heart failure (HF). On admission, physical examination revealed peripheral oedema and abdominal pain. Blood investigations showed elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) at 4333 pg/ml (norm 0–125 pg/ml). Echocardiography disclosed enlargement of all heart chambers, moderate mitral regurgitation and reduced left ventricular ejection fraction of 19% (Figure 1 A). Despite the standard HF treatment with loop diuretics, deterioration was observed with hypotension and an elevated lactate level of 4.1 mmol/l. The severity of cardiogenic shock was assessed as stage D in the Society for Cardiovascular Angiography and Intervention (SCAI) classification [1]. The patient required infusion of dobutamine and levosimendan. Persistent abdominal pain and increased aspartate transaminase (AST) at 198 U/l (norm < 35 U/l) and alanine transaminase (ALT) at 213 U/l (norm < 45 U/l), prompted a computed tomography scan revealing potential indicators of cholecystitis, which were subsequently confirmed through ultrasonography. The Heart Team (HT) decided on an urgent implantation of an Impella CP device, followed by a cholecystectomy, and subsequent qualification for long-term left ventricular assist device (LVAD) implantation. Impella CP was successfully implanted through the femoral artery. Four days later, an open cholecystectomy with a right subcostal Kocher incision was successfully performed. There was no necessity to modify the standard operation protocol. During the procedure, the patient was supported with dobutamine, noradrenaline and Impella CP set to P5 level. Postoperatively, inotropic agents were progressively reduced until complete discontinuation. Initially anticoagulation was conducted using unfractionated heparin under activated clotting time (ACT), however heparin-induced thrombocytopenia was detected. Heparin was subsequently switched to fondaparinux. The patient was reevaluated by the HT and qualified for LVAD therapy. Eight days after the cholecystectomy, the Impella CP was removed and a HeartMate 3 LVAD was implanted. The patient was discharged 14 days later. This case highlights the critical role of the Impella CP device in initial hemodynamic stabilization and possibility to provide temporary mechanical circulatory support (tMCS) during urgent surgical interventions, as demonstrated by Anderson et al. [2]. Furthermore, it underscores the importance of tMCS in managing cardiogenic shock prior to destination therapy such as LVAD therapy.
Full text
4/2024
vol. 20
Image in intervention
Cholecystectomy during Impella CP support in cardiogenic shock
- Institute of Heart Diseases, Wroclaw Medical University, Wroclaw, Poland
- University Clinical Hospital, Wroclaw Medical University, Wroclaw, Poland
- Voivodship Specialistic Hospital, Slupsk, Poland
Adv Interv Cardiol 2024; 20, 4 (78): 509–510
Data publikacji online: 2024/11/05
Article file
References
Baran DA, Grines CL, Bailey S, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter Cardiovasc Interv 2019; 94: 29-37.
Copyright: © 2024 Termedia Sp. z o. o. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0) License (http://creativecommons.org/licenses/by-nc-sa/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, provided the original work is properly cited and states its license.







