
Summary
While provisional side branch stenting is the prominent strategy for distal left main bifurcations, double kissing (DK) crush has favorable outcomes over provisional stenting in selected patients. DK culotte stenting seems to have better outcomes than other bifurcation stenting techniques in bench tests. For the first time, it was demonstrated that the DK culotte technique had lower incidence of target lesion failure compared to the DK crush technique in left main bifurcation lesions.
Introduction
Left main coronary artery (LMCA) disease is a life-threatening condition originating from the large amount of ischemic myocardium. The incidence of unprotected LMCA disease is approximately 5–7% of patients undergoing invasive coronary angiography [1]. The clinical importance of unprotected LMCA (ULMCA) disease is due to the mortality rate, which is up to 50% under medical therapy alone at 3 years [2]. Although coronary artery bypass grafting (CABG) surgery is superior to percutaneous coronary intervention (PCI) in terms of target lesion revascularization (TLR) in studies conducted with first generation drug-eluting stents [3–5], PCI has been shown to be comparable to CABG in new generation drug-eluting stents in recent years [6, 7]. In the double kissing (DK) crush V trial, it was demonstrated that DK crush stenting was superior to provisional stenting in ULMCA disease by reducing target lesion failure (TLF), mainly driven by reduced target vessel myocardial infarction (TVMI) and TLR [8]. In subsequent meta-analyses, it was observed that the DK crush technique improved clinical outcomes compared to other techniques [9]. Thus, DK crush technique has been a frequently used 2-stent strategy, especially in distal left main bifurcation lesions, in recent years.
Culotte stenting is one of the most commonly practiced bifurcation stenting techniques in true coronary bifurcation lesions (CBL). To achieve contemporary DK culotte technique, various modifications of culotte stenting have been implemented. In bench test analysis, DK culotte stenting had better stent configuration and side branch (SB) osteal area compared to other 2-stent techniques including DK crush stenting [10–12]. In a study, DK culotte had lower rate of major adverse cardiac events (MACE) and TLR compared to mini-culotte technique in non-LMCA bifurcations [13]. For this reason, in recent years, DK culotte has become one of the frequently preferred methods, including LMCA revascularization. Unsurprisingly, in a study evaluating patients with ULMCA disease, DK culotte had low MACE incidence with high technical success [14]. However, there is still no randomized trial showing the clinical outcomes of DK culotte stenting in LMCA bifurcation lesions.
Aim
In our study, we aimed to evaluate the clinical outcomes of DK crush and DK culotte techniques in unprotected left main bifurcation lesions.
Material and methods
The present study was a multicenter, retrospective, observational registry which was conducted in 9 heart centers. Patients with ULMCA disease undergoing percutaneous coronary intervention were included in this study. Each participant had to be followed for the clinical outcomes. This trial was approved by the local ethic committee and conducted in accordance with the principles of the Declaration of Helsinki.
Patient population
Patients with unprotected distal left main true bifurcation lesions (Medina classification 1,1,1 or 0,1,1 or 1,0,1) presenting with chronic coronary syndrome or acute coronary syndrome (unstable angina pectoris or non-ST segment elevation myocardial infarction) were enrolled into the study. The exclusion criteria were as follows: history of coronary artery bypass grafting surgery, heart failure with ejection fraction < 40%, chronic total occlusion or calcification requiring calcium modification, PCI for stent restenosis, presenting with cardiogenic shock and ST segment elevation myocardial infarction, history of hematological disorder or malignancy, end stage renal or liver disease, active bleeding, pregnancy, and life-expectancy of < 1 year.
Revascularization strategies
Patients undergoing PCI for unprotected distal left main bifurcation lesion with DK crush or DK culotte techniques were enrolled. Patients treated with provisional stenting or 2-stent techniques other than DK crush or DK culotte were excluded from the study. Additionally, patients in whom the difference between main vessel (MV) and SB reference diameters was ≤ 1 mm were also excluded. Bifurcation techniques were briefly described as follows according to the guideline recommendations [15]. In the DK crush technique, after both branches were wired, SB stent was implanted with a minimal protrusion (2–3 mm protrusion) while a non-compliant coronary balloon (NCB) sized 1 : 1 to the distal MV (DMV) reference diameter was kept uninflated in the MV at the level of the carina. After, SB optimization was performed, balloon crush was performed with an NCB. Then, proximal optimization technique (POT) crush was performed with an NCB sized 1 : 1 to the proximal main vessel (PMV) diameter. After the SB was rewired through a non-distal strut, first kissing balloon dilatation (KBD) was performed with NCBs. The MV stent was implanted, and then POT was performed. After the SB was rewired through a central strut, the second KBD was performed with NCBs. The procedure was terminated with the final POT. In the DK culotte technique, after the SB stent was implanted from the PMV to the SB with a minimal protrusion (2–3 mm), SB optimization was performed. Then, POT was performed. The MV was rewired through the distal strut and then the first KBD was performed. After the MV stent was implanted, the second POT was performed. Then, the SB was rewired through a distal strut. The second KBD was performed and the procedure was terminated with the final POT. For both techniques, MV and SB stents and NCBs were sized 1 : 1 to the MV and SB reference vessel diameters, respectively. POT was performed with an NCB sized 1 : 1 to the PMV diameter. All procedural steps and standardized techniques were evaluated by independent cardiologists. All patients received dual antiplatelet therapy including at least 81–100 mg/day of acetylsalicylic acid and P2Y12 receptor inhibitor and P2Y12 receptor inhibitor for at least 1 year. Intravascular ultrasound imaging (IVUS) usage was according to the operator decision as well as the use of glycoprotein IIb/IIIa receptor inhibitors.
The use of quantitative coronary analysis (QCA) was not mandatory and was performed at the operator’s discretion. The QCA analysis was conducted using the CAAS bifurcation software (Pie Medical Imaging, Maastricht, the Netherlands). At least two orthogonal angiographic views were used to obtain optimal bifurcation anatomy and the widest bifurcation angle besides the evaluation of the minimal lumen area, reference vessel diameters and percent diameter stenosis for each segment of the PMV, DMV, SB, and 5 mm beyond the treated segments [16].
Complex or non-complex LMCA bifurcation was defined according to the DEFINITION (Definitions and impact of complEx biFurcation lesIons on clinical outcomes after percutaNeous coronary IntervenTIOn using drug-eluting steNts) criteria [17]. SB lesion length ≥ 10 mm and SB diameter stenosis ≥ 70% were major criteria. Additional required minor criteria were as follows: > mild calcification, multiple lesions, bifurcation angle < 45° or > 70°, MV reference diameter < 2.5 mm, main vessel lesion length ≥ 25 mm, thrombus-containing lesions. Additionally, the SYNTAX (Synergy between PCI with Taxus and Cardiac Surgery) score calculator (www.syntaxscore.com) was used to obtain the SYNTAX score of each patient.
Study endpoints
Patients were followed up at the hospital admission during the follow-up period of 3 years or by telephone contact for those who had no hospital admission. The primary endpoint of the study was TLF as a composite endpoint of TLR, TVMI, and cardiac death. The TLR was defined as the ischemia-driven revascularization of the MV and/or SB with percutaneous intervention or CABG surgery [16]. A death was defined as cardiac death if a specific cardiac cause was identified, or if the death occurred without clear evidence of a non-cardiac cause. A composite event of peri-procedural MI or spontaneous MI was defined as a TVMI according to the fourth universal definition of myocardial infarction unless there was clear evidence of non-target vessel MI [16, 18]. Peri-procedural MI was defined as a > 5 times elevation of cardiac troponin values in patients with normal baseline values or a change from the baseline level of > 20% in patients with elevated baseline levels, plus at least one of the following: (a) new ischemic electrocardiographic findings, (b) new pathological Q wave, (c) ischemic evidence on imaging, (d) flow-limiting complication on angiographic evaluation. Spontaneous MI was defined as detection of a rise and/or fall of cardiac troponin values with at least one value above the normal limit in addition to at least one of the mentioned criteria above or new STEMI.
Statistical analysis
Fisher’s exact test and the Pearson χ2 test were used for categorical variables. The distribution of variables was analyzed by the Kolmogorov-Smirnov test. For variables with a normal distribution, mean ± standard deviation (SD) was used while median (25th–75th percentiles) was used for variables without a normal distribution. The data were expressed as n (%) for categorical variables. Student’s t-test and the Mann-Whitney U test were used for variables with and without a normal distribution, respectively. The statistical analyses of the endpoints were analyzed using the Kaplan-Meier method (with the log-rank test), and Cox regression analysis was used to analyze outputs of hazard ratio (HR) and 95% confidence interval (CI). Statistical analysis was performed using the computer (IBM SPSS Statistics for Windows (IBM Corp., Armonk, New York, USA). A p-value < 0.05 was considered statistically significant.
Results
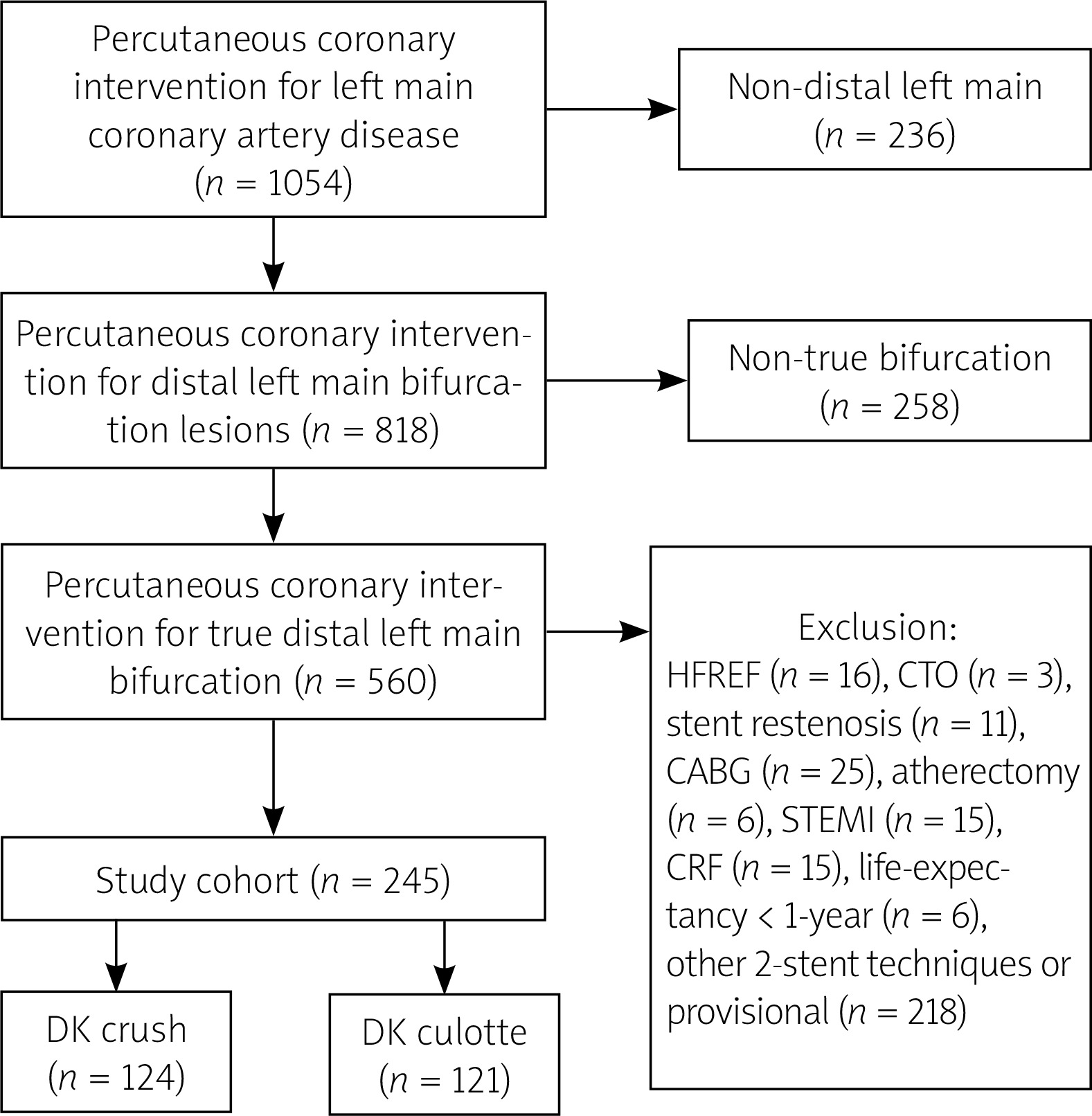
The study was conducted in 9 high-volume tertiary heart centers. The flow chart of the study is presented in Figure 1. A total of 5673 PCI procedures were evaluated and 1054 PCI of LMCA were screened. Then, 236 patients with a non-distal bifurcation lesion and 258 patients with a non-true distal bifurcation lesion were excluded. Additionally, 315 patients were excluded from the study (25 with history of coronary artery bypass grafting surgery, 218 treated with provisional technique or other 2-stent techniques, 16 with reduced ejection fraction heart failure, 3 with chronic total occlusion, 6 with calcification requiring calcium modification, 11 with stent restenosis, 15 with ST segment elevation myocardial infarction, 15 with end stage renal failure, 6 with life expectancy of < 1 year). Finally, a total of 245 patients with unprotected distal LMCA bifurcation lesions treated with DK culotte (121 patients) or DK crush (124 patients) technique were enrolled in this study.
Figure 1
Study flow chart. Inclusion and exclusion criteria of the study
CABG – coronary artery bypass grafting, CRF – chronic renal failure, CTO – chronic total occlusion, DK – double kissing, HFREF – heart failure with reduced ejection fraction, STEMI – ST segment elevation myocardial infarction.
The sample size of the study was estimated based on the DK crush V trial [8] and a study by Mukhopadhyay et al. [14] in which the cumulative major adverse cardiac event (MACE) at 1-year follow-up occurred in 5.0% of patients with DK crush and 2.2% with DK culotte technique. Thus, our sample size was calculated as 887 with 80% power and 0.1 margin of error. However, we did not reach a sufficient number of patients. Unfortunately, this causes statistical limitations in the study results.
The mean age of the patients was 63 ±12 and 23.3% of patients were female. The baseline clinical and demographic variables of the patients are shown in Table I. There were no differences in terms of age, gender, laboratory parameters, history of hypertension, diabetes mellitus, previous PCI, atrial fibrillation, smoking status, medication usage, clinical presentation, symptom status, and ejection fraction.
Table I
Baseline clinical and demographic variables
[i] ACEI – angiotensin converting enzyme inhibitor, ARB – angiotensin receptor blocker, CCS – Canadian Cardiovascular Society, DK – double kissing, HDL – high-density lipoprotein, LDL – low-density lipoprotein, Non-STEMI – non-ST segment elevation myocardial infarction, OAC – oral anticoagulation, PCI – percutaneous coronary intervention, USAP – unstable angina pectoris.
Angiographic and procedural features
Angiographic and procedural characteristics of patients are presented in Table II. The severity of coronary artery disease was similar between groups with a 3-vessel disease incidence of 33.9% in the DK culotte group and 37.1% in the DK crush group. On the other hand, the SYNTAX score was also comparable. The incidence of intra-aortic balloon pump usage, arterial access site, and glycoprotein IIb/IIIa usage did not differ between groups. The mean bifurcation angle was 69 ±12° in the DK culotte group and 68 ±14° in the DK crush group. The diameter stenoses of the PMV, DMV, and SB were similar, as were the lesion lengths of the MV and SB. The incidence of final KBD and POT was 97.5% and 99.2% in the DK culotte group vs. 94.4% and 99.2% in the DK crush group, respectively. The IVUS usage ratio was 19.0% in the DK culotte group and 20.2% in the DK crush group. There was no difference in terms of complex bifurcation (38.0% in DK culotte group and 40.3% in DK crush group) lesions. The mean procedural time was lower in the DK culotte group compared to the DK crush group (65 ±26 min, 73 ±29 min; p = 0.048).
Table II
Angiographic and procedural features
[i] CAD – coronary artery disease, DK – double kissing, DMV – distal main vessel, IABP – intra-aortic balloon pump, IVUS – intravascular ultrasound, MV – main vessel, PMV – proximal main vessel, POT – proximal optimization technique, SB – side branch, SYNTAX – Synergy between PCI with Taxus and Cardiac Surgery.
Clinical outcomes
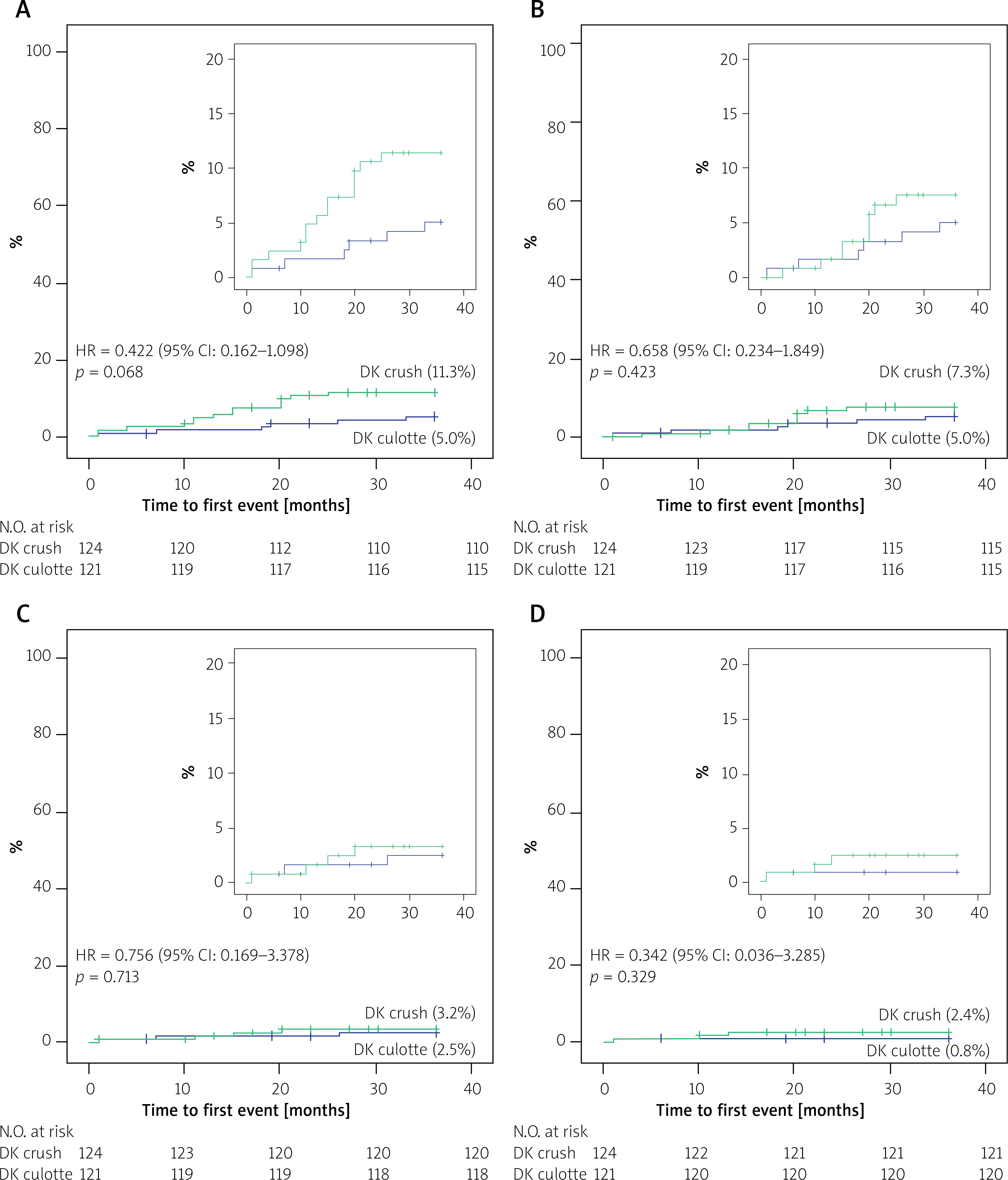
The primary endpoint of the study was target lesion failure (TLF) as a composite endpoint of TLR, TVMI, and cardiac death. The angiographic follow-up was obtained in 45 (37.1%) patients in the DK culotte group and 53 (42.7%) patients in the DK crush group. The clinical outcomes were compared between groups adjusted for diabetes mellitus, SYNTAX score, IVUS usage and lesion complexity. One-year TLF was similar in both groups with an incidence of 1.7% in the DK culotte group and 4.8% in the DK crush group (HR = 0.506, 95% CI: 0.098–2.621; p = 1.16). There was no difference in 1-year TLR (1.7% vs. 1.6%, HR = 3.355, 95% CI: 0.290–38.81; p = 0.98), TVMI (1.7% vs. 1.6%, HR = 1.121, 95% CI: 0.151–8.309; p = 0.98), or cardiac death (0.8% vs. 1.6%, HR = 0.391, 95% CI: 0.040–3.835; p = 0.57). The number of patients with 3-year TLF was lower in the DK culotte group, without statistical significance (5.0% vs. 11.3%, HR = 0.557, 95% CI: 0.211–1.471; p = 0.06). There was also no difference in terms of 3-year TLR (5.0% vs. 7.3%, HR = 0.907, 95% CI: 0.310–2.651; p = 0.42), TVMI (2.5% vs. 3.2%, HR = 0.762, 95% CI: 0.160–3.627; p = 0.71), or cardiac death (0.8% vs. 2.4%, HR = 0.733, 95% CI: 0.063–8.550; p = 0.32) (Table III, Figure 2).
Table III
Clinical outcomes
Discussion
In the present study, clinical outcomes of DK crush and DK culotte stenting in unprotected distal left main bifurcation lesions were compared for the first time. The 3-year clinical outcomes of DK culotte stenting were comparable to DK crush stenting. The number of patients with TLF was lower in the DK culotte group than the DK crush group in unprotected distal left main bifurcations.
The optimal treatment strategy of the distal left main bifurcation lesions has been investigated in several randomized trials. While provisional stenting is a highly effective strategy for true distal left main bifurcation lesions [19], a planned 2-stent strategy may be preferred over the provisional technique when an SB disease is extensive and/or a high anatomical complexity is present [9, 20]. The DK crush technique is recommended by guidelines when the target vessel is an unprotected true distal left main bifurcation [20]. In the DK crush V trial, provisional stenting was compared to DK crush technique in 482 patients with unprotected distal left main bifurcations [8]. The DK crush technique had a lower rate of TLF, which was mainly driven by TVMI and TLR, compared to provisional stenting at 3-year follow-up regardless of whether the bifurcation lesion was complex. In the DK crush III trial, DK crush technique had a lower rate of MACE compared to culotte technique at 3-year follow-up [21]. The incidence of TLR and MI was also lower in the DK crush technique than culotte. In the EBC MAIN trial, a planned 2-stent strategy was compared to stepwise provisional stenting in distal true left main bifurcations [19]. There was no difference in terms of primary composite endpoint. However, DK crush technique was performed in only 5% of the patients, whereas more than 85% of patients were treated with culotte or T/T and small protrusion (TAP) techniques. In the light of the foregoing data, DK crush, which is one of the optimal 2-stent strategies according to the guideline recommendations, had more favorable outcomes than provisional stenting and other traditional 2-stent strategies.
DK culotte is the other contemporary 2-stent technique which is recommended by guidelines. To achieve contemporary DK culotte technique, various modifications of culotte stenting have been implemented over the years. In the culotte strategy, SB osteal restenosis may be higher than expected due to the napkin ring formation and SB osteal stenosis. With the DK culotte technique, the stent configuration was ensured to be more optimal. In a bench test analysis, DK culotte was associated with shorter metal carina length and smaller SB osteal stenosis as well as decreased malapposition compared to culotte technique [11]. In the other bench test, DK culotte had lower malapposition rates compared to DK crush technique [12]. In the MOBBEM study, culotte had better stent configuration in terms of stent apposition compared to other 2-stent strategies [10]. However, the adherence to guideline recommendations to achieve contemporary 2-stent techniques was found to be the main determinant of the endpoints [12]. Thus, it is expected that the results with contemporary techniques that comply with current guideline recommendations will be better than traditional bifurcation stenting techniques. Therefore, in recent years, the results of the DK culotte technique on bifurcation lesions have become a subject of interest. In a retrospective data, DK culotte had lower rates of MACE and TLR compared to mini-culotte technique in non-left main bifurcation lesions [13]. In a subgroup analysis of a Lower Silesia culotte Bifurcation Registry, the number of patients with TLF and MACE was lower in DK culotte technique compared to culotte in left main bifurcation in acute coronary syndrome [22]. On the other hand, in an optical coherence tomography (OCT) guided PCI study, the 1-year MACE was only 2.2% in the DK culotte technique in distal left main revascularization [14], which was 7 times higher with culotte technique in the DK crush III trial [21]. Therefore, the DK culotte technique has become an increasingly preferred strategy among invasive cardiologists in the treatment of true bifurcation lesions. Additionally, DK culotte had favorable outcomes over DK crush in non-left main bifurcation lesions [23]. However, no randomized study has yet been conducted with DK culotte. In our study, the 1-year TLF of DK culotte was comparable with the DK crush technique. Nevertheless, large scaled, randomized trials are needed to evaluate the clinical outcomes of DK culotte technique in true CBLs, especially in LMCA disease.
It was a retrospective and non-randomized trial, constituting a major limitation. Additionally, the borderline statistical significance of the primary endpoint, the potential for underpowering, and the lack of core lab analysis were also major limitations. Therefore, it was not possible to explain the superiority of one technique over the other, while the results were comparable for both techniques. Additionally, the operator’s experience may have been misleading. However, the 3-year results of the DK crush technique in our study were similar to the 3-year results of the DK crush V trial. It means that the DK crush technique was performed as well as possible. On the other hand, the retrospective design of the study inherently introduces selection and performance bias due to the operators’ experience and preferences. However, in our study, there was no difference between the two groups in terms of parameters that could affect the results, such as lesion characteristics, anatomical complexity, and bifurcation features. The use of intravascular imaging was lower than expected, which was another major limitation that could have affected the clinical outcomes. The relatively small sample size was a further limitation. However, the lack of a significant difference in demographic and angiographic characteristics between the groups limits the possible impact on the results.







