
Summary
The complete agreement between the fractional flow reserve (FFR) and the instantaneous wave-free pressure ratio (iFR) assessment observed in the presented population suggests that in the group of patients with severe aortic stenosis the choice of an invasive method to assess the physiological significance of the stenosis in the coronary artery is not crucial – both iFR and FFR give comparable results. Perhaps, from this perspective, the iFR test, due to the lack of the necessity to induce hyperaemia, may prove to be a safer alternative, especially in patients with a higher risk of conduction disorders.
Introduction
Coronary heart disease and aortic stenosis
Coronary heart disease is widespread – the lifetime risk of this disease approaches 25% of persons aged 30 years without a known cardiovascular disease [1]. Among patients with coronary heart disease, some are diagnosed with severe aortic stenosis. This group is not large, although it increases with patients’ age from just over 1% in the group of patients aged 60 years to about 10% after the age of 80 years [2]. The clinical picture of both diseases is slightly different, but the risk factors may be similar.
In patients diagnosed with severe aortic stenosis (defined as valve area < 1 cm2, jet velocity > 4 m/s, and/or mean transvalvular gradient > 40 mm Hg) simultaneously with suspected or diagnosed coronary heart disease, coronary angiography is performed as part of the qualification for final treatment. Based on the coronary angiography results, revascularization is indicated when there is evidence of significant obstruction of the coronary blood flow. For intermediate lesions, obtaining coronary artery physiologic data can facilitate clinical decision-making regarding the need for revascularization [3, 4].
Fractional flow reserve
The fractional flow reserve (FFR) is a measure of the pressures proximal and distal to the stenotic lesions at a maximal flow. Maximal blood flow (hyperaemia) is most commonly induced by intravenous or intracoronary administration of adenosine. The ratio of distal coronary pressure to aortic pressure during maximal hyperaemia is called the FFR. A normal value is 1, while values < 0.80 are associated with provoked ischaemia [5].
Instantaneous wave-free pressure ratio
An adenosine-independent pressure index of coronary stenosis severity has been developed as a substitute for FFR [6], called the instantaneous wave-free pressure ratio (iFR). The cut-off point for iFR measurements is mostly chosen at 0.89.
Quantitative flow ratio
Quantitative flow ratio (QFR) analysis was performed using Medis QAngio XA 3D 2.0 software. The vessel stenosis was evaluated using calculation of the flow velocity of the contrast through the lesion in a coronary vessel, based on 3-dimensional quantitative coronary angiography (3D QCA). The cut-off point for QFR measurements was chosen at 0.80. QFR analysis was performed by KCRI CoreLab (Krakow, Poland).
Aim
In patients with severe aortic stenosis, the left ventricle’s blood pressure values may differ compared to patients with normal valve function of the left arterial outlet. This pressure may translate into the force recorded in the epicardial arteries. It may influence the physiological assessment of the severity of stenosis, especially by FFR during induced hyperaemia. The study aim was to compare the assessment results of the physiological significance of coronary artery stenosis using the FFR method with iFR and QFR.
Material and methods
Data were collected on all patients hospitalized in the years 2019–2020 at the 2nd Department of Cardiology, University Hospital in Krakow, diagnosed with severe aortic valve stenosis and ischaemic heart disease with border changes in the coronary arteries. All patients were qualified for invasive physiological assessment of coronary artery stenosis. The cut-off for FFR as well as for QFR was 0.80, and for iFR it was 0.89. Off-line QFR analysis of previously assessed coronary arteries was performed using Medis QAngio XA 3D 2.0 software – the analyst performing the QFR assessment did not know the result of the FFR/iFR assessment. The study was a retrospective registry of patients diagnosed according to local standards, so ethics committee approval was not required.
Statistical analysis
Categorical variables are presented as numbers and percentages. Continuous variables were expressed as mean and standard deviation (SD). Differences between groups were compared using the Wilcoxon test for continuous variables. Pearson’s χ2 test compared categorical variables. Two-sided p-values < 0.05 were considered statistically significant. All calculations were done with JMP®, Version 15.0.0 (SAS Institute Inc., Cary, NC, USA).
The true-positive rate (TPR) was calculated as a proportion of true positive and condition positive. The false-positive (FPR) rate was calculated as a proportion of false positive and condition negative. The false-negative rate (FNR) was calculated as a proportion of false negative and condition positive. The true-negative rate (TNR) was calculated as a proportion of true negative and condition negative. Condition positive is defined as the sum of a true positive and a false negative. Condition negative is defined as the sum of a true negative and false positive.
Results
Between 1.2019 and 12.2020, 12 patients with severe aortic stenosis and borderline lesions in the coronary artery, qualified for physiological assessment, were hospitalized in the 2nd Department of Cardiology, University Hospital in Krakow.
We collected the baseline demographic and angiographic data with a physiological assessment of coronary circulation for all 12 patients and 13 vessels. There were 6 (50%) women, and the the mean age was 73.8 ±7.5 years. The mean left ventricular ejection fraction was 52 ±15%. The mean aortic valve area was 0.80 ±0.16 cm2. The mean aortic valve area indexed to the body surface area was 0.44 ±0.07 cm2/m2. The mean maximal transvalvular gradient was 64.6 ±20.2 mm Hg, and the mean mean transvalvular gradient was 38.4 ±12.8 mm Hg.
The left anterior descending artery was assessed in 12 of 13 cases (92%). Additionally, one circumflex artery was investigated in our group. FFR assessment was performed in 12 vessels, 5 vessels were assessed by iFR, and QFR was used to analyse all 13 vessels.
In the whole group, 12 vessels from 13 were assessed by FFR. Five of them were haemodynamically significant. The detailed distribution of FFR/iFR and QFR results are presented in Figures 1 and 2.
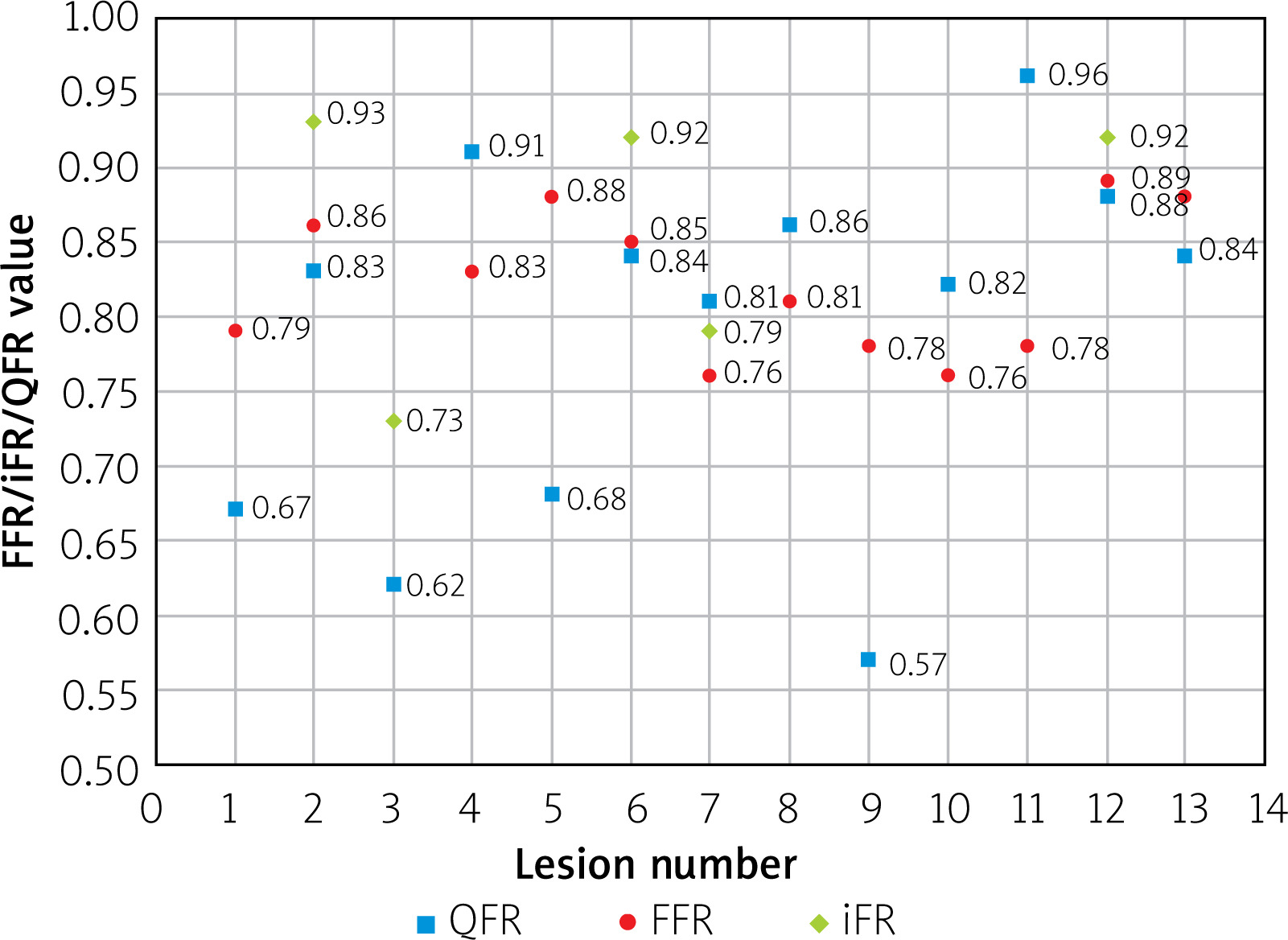
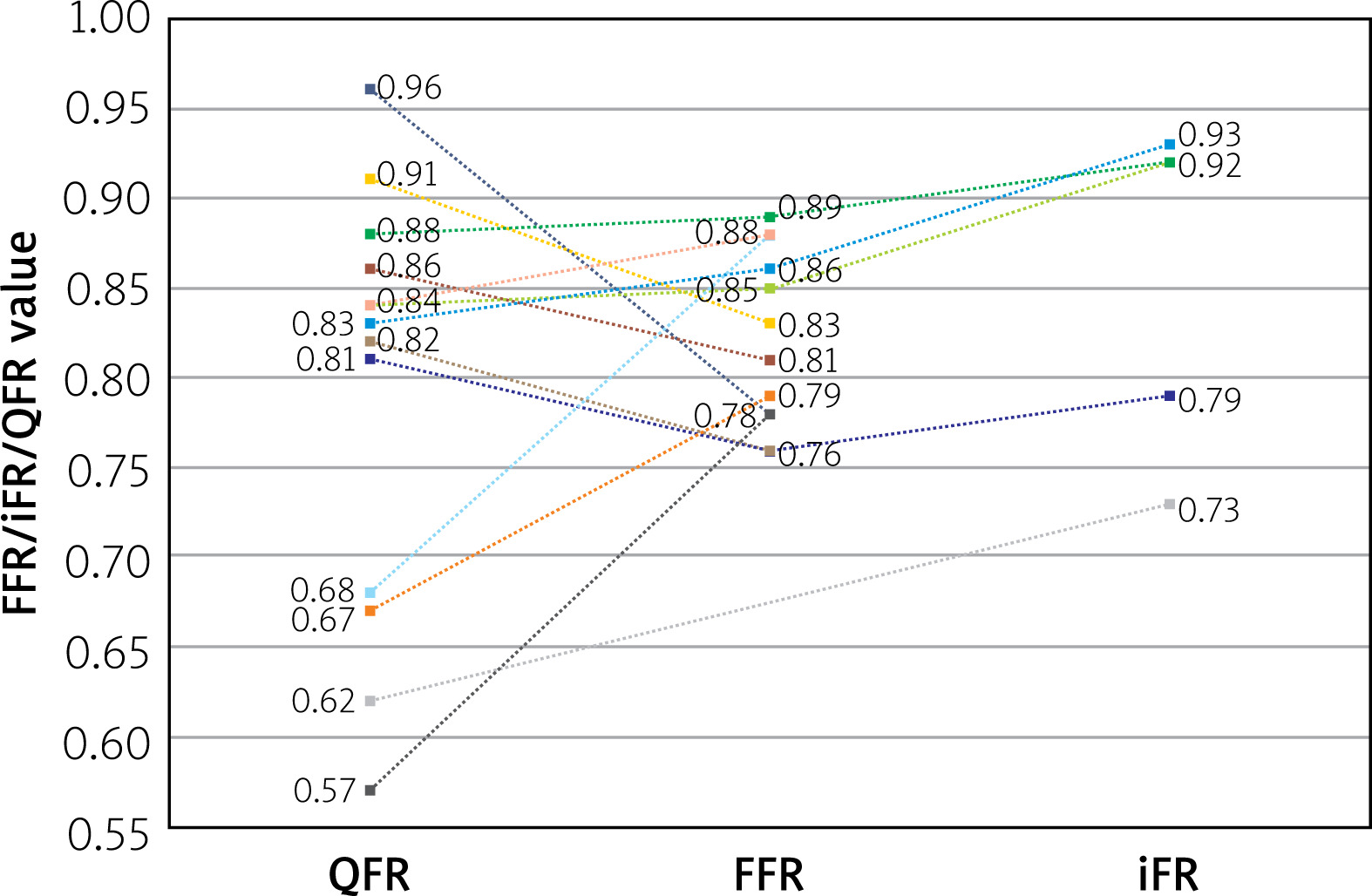
In comparison to FFR, all iFR measurements were concordant with FFR – when FFR indicated significant stenosis, iFR did not exceed 0.89. For non-significant lesions, all iFR measures were over 0.89. The total agreement between FFR and iFR was 100%.
QFR analysis indicated 4 significant lesions and 9 non-significant. The total agreement between QFR and FFR/iFR assessment was 69%. In the group of significant lesions, 3 of 4 were assessed as significant in FFR/iFR assessment, i.e. 75% agreement. In the group of non-significant lesions, 6 were evaluated as non-significant in FFR/iFR analysis, i.e. 67% agreement.
When we assume FFR/iFR results as a reference, the contrast-QFR assessment achieved the following parameters: TPR 0.75, FPR 0.33, FNR 0.25, and TNR 0.67.
Comparing the group with concordant results of FFR/iFR measurements with QFR, it was observed that in this group, the percentage of men tended to be higher (56% vs. 33%, p = 0.5050); patients tended to be older (74.1 vs. 73 years; p = 0.5778) with a lower ejection fraction of the left ventricle (48.6% vs. 60.0%; p = 0.1417) and higher aortic valve area (0.83 vs. 0.73 cm2; p = 0.7540), in comparison to the group in which the results of FFR/iFR measurements were different from QFR. However, all the observed differences were statistically not significant.
Discussion
Analysing the obtained results, we can see that in patients with severe aortic stenosis, who undergo an invasive physiological assessment in coronary arteries, only stenoses located in the left anterior descending artery (LAD) were assessed. One assessment of the circumferential branch was made in a patient diagnosed with LAD, probably due to the prognostic significance of LAD revascularization.
One of the reasons for the observed differences between the FFR/iFR and QFR assessments is that QFR analysis was performed retrospectively based on standard angiographic recordings, which were not always optimally performed for QFR assessment. Currently published studies indicate good agreement of the QFR assessment with the results of the assessment of invasive changes in the coronary vessels in a similar group of patients [7–9].
Particular attention is paid to the complete agreement of the FFR with the iFR assessment. This fact may suggest that in the group of patients with severe aortic stenosis, the choice of an invasive method to assess the physiological significance of the stenosis in the coronary artery is probably not crucial – iFR and FFR give comparable results. Perhaps from this perspective, the iFR test, due to the lack of necessity to induce hyperaemia, will prove to be a safer alternative, especially in the group of patients with a higher risk of conduction disorders.
The following limitations of the presented analysis should be taken into account: the study group was small, and the obtained results did not allow for a clear assessment of the equivalence of the iFR and FFR assessments in the diagnosis of coronary artery disease in patients with severe aortic stenosis.







