
Introduction
Computed tomography (CT)-guided lung biopsy, which includes both core needle biopsy (CNB) and fine needle aspiration biopsy (FNAB), has been widely used in diagnosis of lung nodules and masses with the diagnostic accuracy > 90% [1–5].
In recent years, treatment modalities for lung cancer have not only included conventional chemo- and radiotherapy, but also encompassed the application of individual molecular target therapies [6–8]. The common tested genes include the epidermal growth factor receptor (EGFR) gene and the anaplastic lymphoma kinase (ALK) fusion gene [6–8]. The tyrosine kinase inhibitor (TKI) gefitinib could be potentially used as the first-line treatment for patients with non-small-cell lung cancer who display EGFR gene mutation, and the TKI gefitinib could effectively prolong the progression-free survival (9.2 vs. 6.3 months, p < 0.001) when compared to patients who received the conventional chemotherapy for treatment [9]. Therefore, CT-guided lung biopsy has been widely used for molecular testing [10–21]. However, the adequacy rates for the molecular tests (83–99%), positive rates of EGFR mutations (34–72%) and ALK translocation (5–9%) have been found to significantly vary among these studies [10–21]. These differences may be attributed possibly to the use of different types of needles (fine or core needles) or different lesion sizes. Therefore, a proper meta-analysis is needed to make an explicit conclusion for the clinical application of CT-guided biopsy in molecular tests.
Aim
In this meta-analysis, we aimed to evaluate the potential clinical effectiveness of CT-guided lung biopsy in molecular tests.
Material and methods
Study selection
We explored the related studies from the PubMed, Embase, and Cochrane Library until July 2021. This meta-analysis was registered at https://inplasy.com/ (Number: INPLASY202180059). The research strategy used was: ((((computed tomography[Title/Abstract]) OR (CT[Title/Abstract])) AND ((lung[Title/Abstract]) OR (pulmonary[Title/Abstract]))) AND (biopsy[Title/Abstract])) AND (((molecular[Title/Abstract]) OR (gene[Title/Abstract])) OR (genic[Title/Abstract])).
The inclusion criteria were as follows: (a) the studies included the contents of CT-guided lung biopsy for molecular tests; and (b) the studies should contain at least one of the following endpoints: adequacy rates for molecular testing, positive rates of EGFR mutations, ALK translocation, and Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations. The exclusion criteria were: (a) studies which did not report the type of needles used; (b) case reports; (c) animal studies; and (d) reviews.
Quality assessment
All included studies were non-randomized controlled trials, which were assessed by at least two independent investigators with the Newcastle–Ottawa scale [22]. The 9-point Newcastle-Ottawa scale was assessed in the aspects of selection (4 points), comparability (2 points), and exposure (3 points), with assessments of high (≥ 7), moderate (4–6), and low (< 4) qualities.
Data extraction
For this analysis, two investigators independently extracted data from these studies, and a third investigator was included to resolve any discrepancies. First authors, publication years, countries, sample sizes, gender distributions, age, and lesion size were regarded as the baseline data. The endpoints in this study included adequacy rates for molecular tests, positive rates of EGFR mutations, ALK translocation, and KRAS mutations. Among these, the adequacy rates for molecular testing were considered as the primary endpoint.
Statistical analysis
Stata v12.0 was used to calculate the pooled adequacy rates for molecular tests, positive rates of EGFR mutations, ALK translocation, and KRAS mutations. The random-effects model was generated. Heterogeneity was calculated using the Q test and the I2 statistic, with I2 > 50% being indicative of significant heterogeneity. The sources of heterogeneity were detected using meta-regression, subgroup analysis, and sensitivity analysis. The subgroup analyses were performed based on the different needle types (fine or core needles) used, mean lesion sizes (< or ≥ 4 cm), and countries (Asian or Western). Additionally, the Egger test was used to evaluate the potential risk of publication bias by Stata v12.0. A high risk of publication bias was considered if the p-value was > 0.05.
Results
Study characteristics
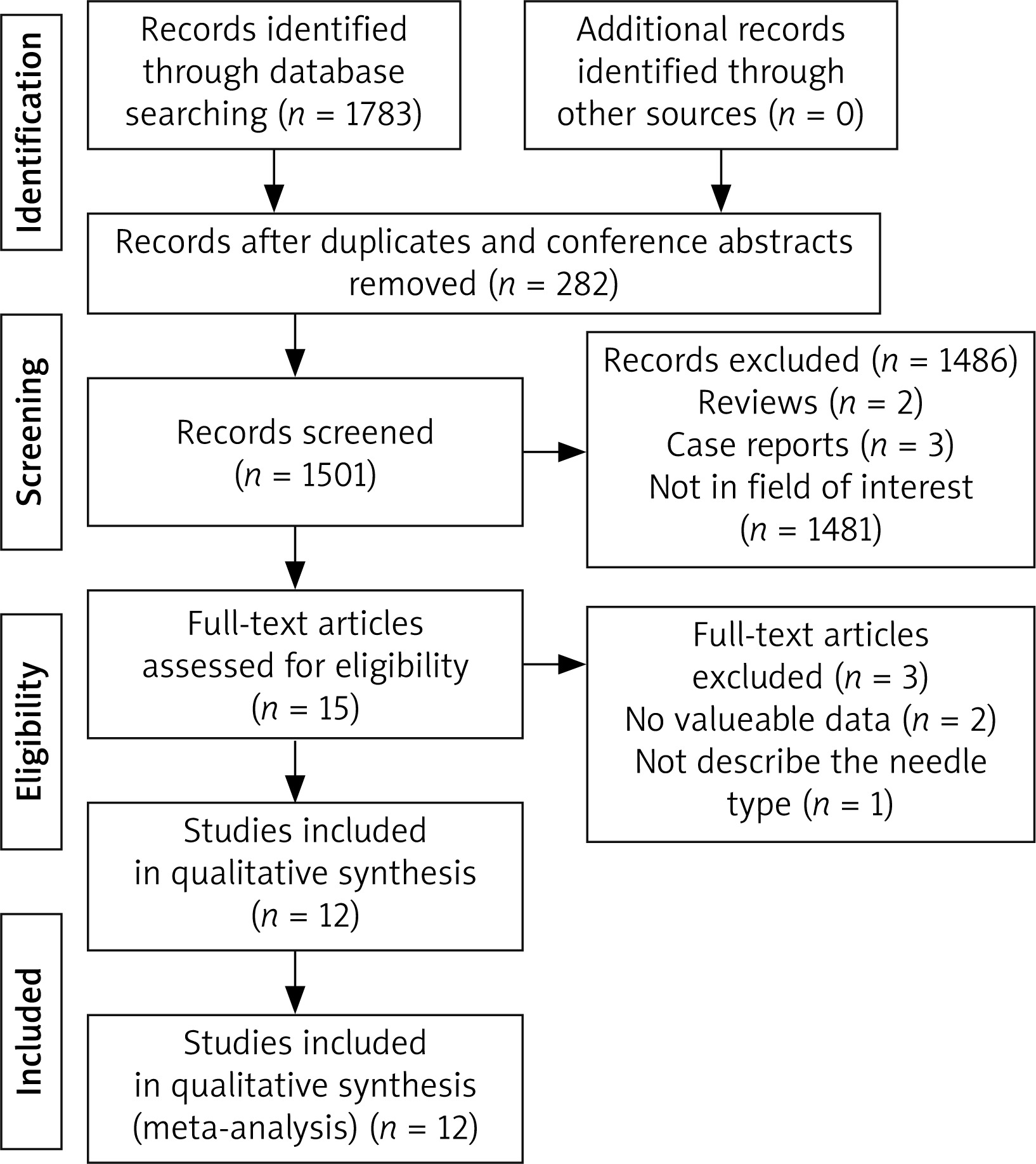
Initially, we explored a total of 1783 studies that were potentially relevant to the present analysis. Thereafter, 282 duplicate studies were excluded from the analysis. Based on the selection criteria, 15 studies were assessed for eligibility. Among these 15 studies, 3 were excluded because of a lack of data about endpoints (n = 2) and insufficient information about the needle types used (n = 1). Finally, 12 studies were included in this meta-analysis (Table I, Figure 1).
Table I
Characteristics of studies included in meta-analysis
| Studies | Year | Country | Total patient number | Gender (male/female) | Patients with molecular test | Mean age [years] | Size of lesion [cm] | NOS |
|---|---|---|---|---|---|---|---|---|
| Zhuang [10] | 2011 | China | 43 | 16/27 | 43 | 62 | 4 | 8 |
| Cheung [11] | 2010 | Taiwan | 47 | 24/23 | 47 | 64.6 | 4 | 8 |
| Hou [12] | 2013 | China | 40 | 29/11 | 40 | 32-81 | 3.3 | 8 |
| Hsiao [13] | 2013 | Taiwan | 332 | 199/153 | 134 | 65.3 | 4.9 | 8 |
| Wang [14] | 2013 | China | 228 | 93/135 | 228 | 62.1 | 3.4 | 8 |
| Chen [15] | 2014 | China | 353 | 228/125 | 236 | 59 | 4 | 8 |
| Coley [16] | 2015 | USA | 210 | Not given | 115 | Not given | Not given | 6 |
| Florentine [17] | 2015 | USA | 216 | 103/113 | 22 | 70 | Not given | 7 |
| Lian [18] | 2017 | China | 250 | 156/94 | 250 | 63 | Not given | 7 |
| Tian [19] | 2017 | China | 560 | 323/237 | 176 | 51.8 | 1.8 | 8 |
| Beck [20] | 2017 | Korea | 196 | 72/124 | 100 | 67.7 | 4.1 | 8 |
| Porrello [21] | 2019 | Italy | 42 | Not given | 23 | Not given | Not given | 6 |
All studies included were retrospective. Moreover, 10 studies could be considered as of high quality [10–15, 17–20], while 2 studies were regarded as having moderate quality [16, 21]. A total of 2559 patients underwent CT-guided lung biopsy and 1414 of them received molecular testing.
Moreover, among the 12 studies, 9 were from Asia and 3 were from Western countries. Two studies used fine needles [10, 14], 7 used core needles [11–13, 15, 19–21], and 3 employed both fine and core needles [16–18]. The sizes of the needles ranged from 16G to 20G. Five studies only tested EGFR mutations [10–14], 5 studies tested EGFR mutations and ALK translocation [15, 17–19, 21], and 2 studies tested EGFR mutations, ALK translocation, and KRAS mutations [16, 20] (Table II).
Table II
Characteristics of CT-guided biopsy
| Studies | Types of needles | Size of needles | Contents of molecular tests | Adequacy for molecular test | Positive EGFR mutation | Positive ALK translocation | Positive KRAS mutation |
|---|---|---|---|---|---|---|---|
| Zhuang [10] | Fine | 18 and 20G | EGFR | Not given | 53% | – | – |
| Cheung [11] | Core | 18 and 20G | EGFR | Not given | 72% | – | – |
| Hou [12] | Core | 18 and 20G | EGFR | Not given | 38% | – | – |
| Hsiao [13] | Core | 18 and 20G | EGFR | 99% | 60% | – | – |
| Wang [14] | Fine | 18 and 20G | EGFR | 96% | 43% | – | – |
| Chen [15] | Core | 16G | EGFR, ALK | 99% | Not given | Not given | – |
| Coley [16] | Core, Fine | 20 and 22G | EGFR, ALK, KRAS | 96% | Not given | Not given | Not given |
| Florentine [17] | Core, Fine | 20G | EGFR, ALK | 95% | Not given | Not given | – |
| Lian [18] | Core, Fine | 16–20G | EGFR, ALK | 83% | 50% | 7% | – |
| Tian [19] | Core | 18G | EGFR, ALK | 95% | 43% | 8% | – |
| Beck [20] | Core | 20G | EGFR, ALK, KRAS | 96% | 34% | 5% | 6% |
| Porrello [21] | Core | 16–18G | EGFR, ALK | Not given | 44% | 9% | – |
Adequacy rate for molecular tests
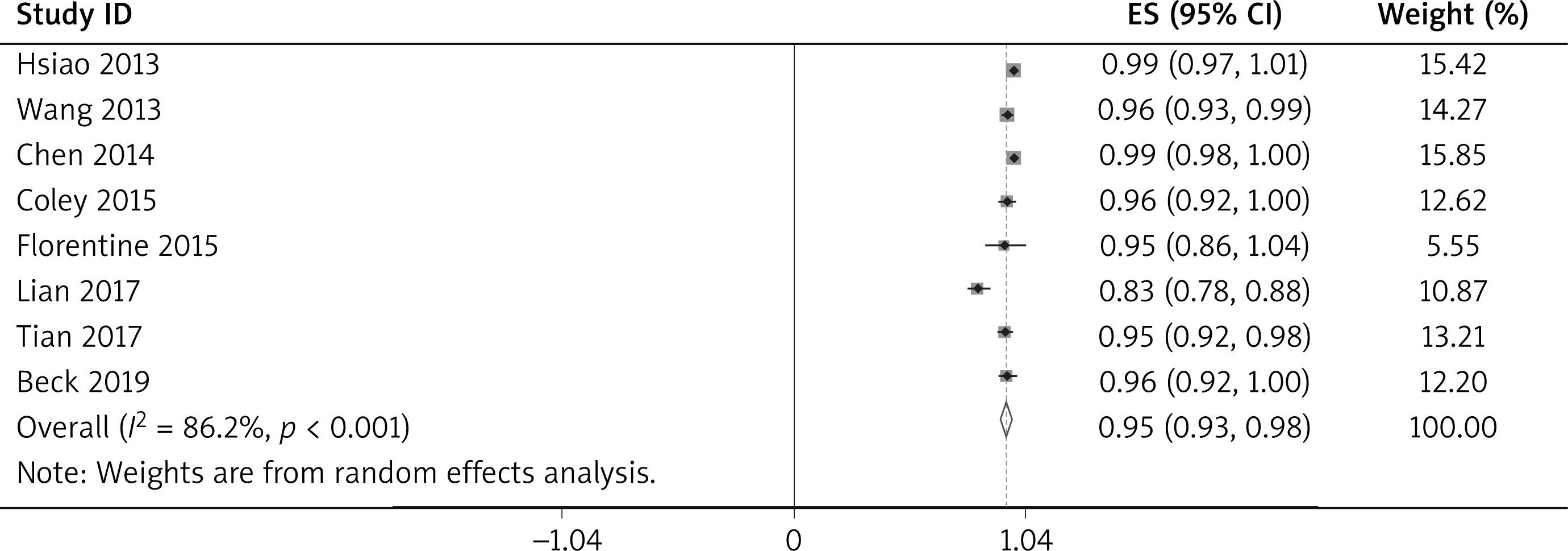
It was found that eight studies with 1261 patients reported the adequacy rates for molecular tests [13–20]. The pooled adequacy rate for molecular tests was 95% (95% CI: 93–98%, Figure 2). Significant heterogeneity was detected among these studies (I2 = 86.2%, p < 0.001). A high risk of publication bias was also found (Egger test: p = 0.043).
The meta-regression analysis indicated that the adequacy rate for molecular testing was not directly associated with the needle types used (p = 0.338, 95% CI: –0.25–0.11), lesion sizes (p = 0.729, 95% CI: –0.12–0.15), or countries (p = 0.452, 95% CI: –0.10–0.19).
The subgroup analyses are shown in Table III. The pooled adequacy rates for molecular tests were 98%, 96%, and 91% based on the use of a core needle, fine needle, or both types, respectively. Significant heterogeneity was only detected in the subgroup in which both types of needles were used (I2 = 94.7%, p < 0.001). The pooled adequacy rates for molecular tests were 99%, 96%, and 91% based on the different mean lesion sizes (≥ 4 cm, < 4 cm, and unknown, respectively). Significant heterogeneity was only detected in the unknown subgroup (I2 = 94.7%, p < 0.001). The pooled adequacy rates for molecular tests were 96% and 96% based on patients belonging to Asian and Western countries, respectively, but significant heterogeneity was only detected in the subgroup of patients in Asian countries (I2 = 90%, p < 0.001).
Table III
Subgroup analysis in adequacy for molecular test
The sensitivity analysis data showed that the significant heterogeneity disappeared (I2 = 50%, p = 0.060) when the study by Lian et al. [18] was removed.
Positive rates of EGFR mutations
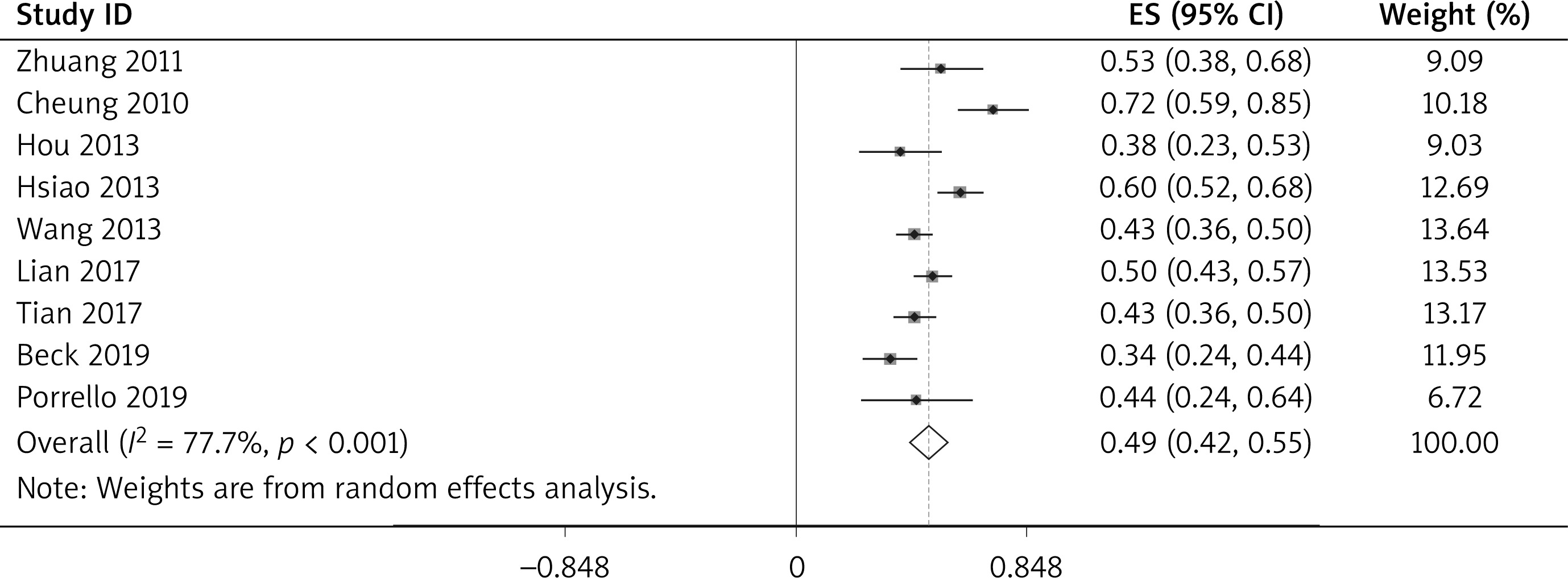
Nine articles with 971 patients reported positive rates of EGFR mutations [10–14, 18–21]. The pooled positive rate of EGFR mutation was 49% (95% CI: 42–55%, Figure 3) and significant publication bias was found (Egger test: p = 0.727).
The meta-regression analysis found that the positive rates of EGFR mutations were not associated with the needle types used (p = 0.655, 95% CI: –0.29–0.20), lesion size (p = 0.349, 95% CI: –0.13–0.31), or the countries (p = 0.590, 95% CI: –0.60–0.38).
The subgroup analyses are shown in Table IV. The pooled positive rates of EGFR mutations were 49%, 47%, and 44% based on the application of a core needle, fine needle, and both of them, respectively. Significant heterogeneity was only detected in the core needle subgroup (I2 = 87.8%, p < 0.001). The pooled positive rates of EGFR mutation were 53%, 43%, and 49% based on the different mean lesion sizes (≥ 4 cm, < 4 cm, and unknown, respectively). Significant heterogeneity was only detected in the subgroup of lesion size ≥ 4 cm (I2 = 88.4%, p < 0.001). The pooled positive rates of EGFR mutations were 48% and 44% based on patients in Asian and Western countries, respectively. Significant heterogeneity was only detected in the subgroup of Asian countries (I2 = 80.4%, p < 0.001).
Table IV
Subgroup analysis in positive rate of EGFR mutation
The sensitivity analysis showed that significant heterogeneity always existed after removing any of these included studies.
Positive rates of ALK translocation
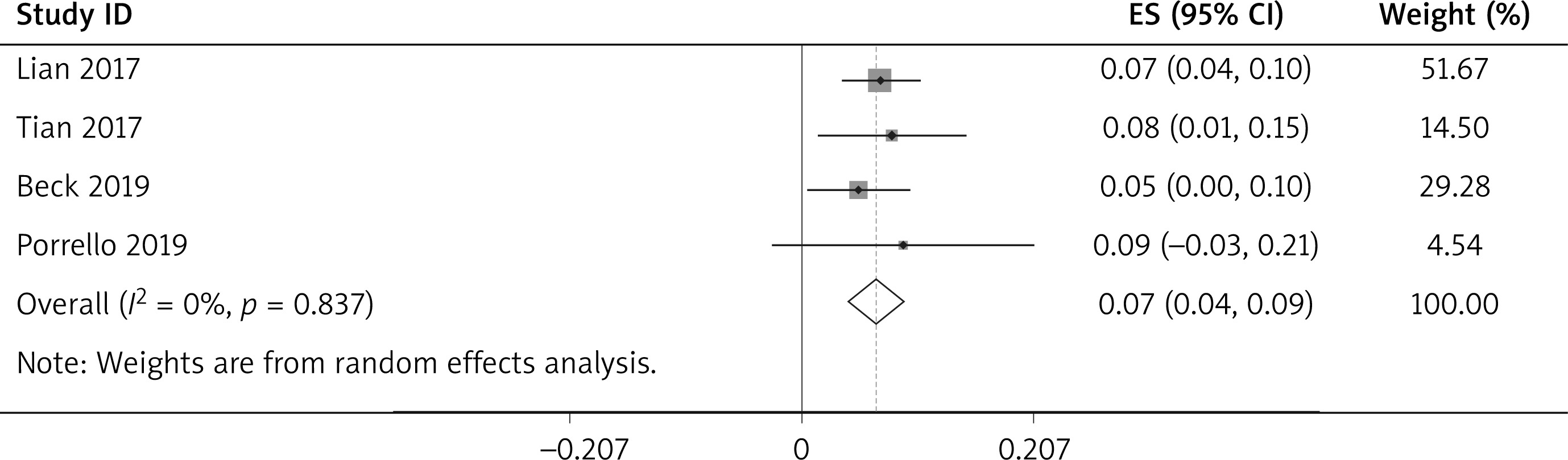
Four articles with 383 patients reported the positive rates of ALK translocation [18–21]. The pooled positive rate of ALK translocation was 7% (95% CI: 42–55%, Figure 4). However, no significant heterogeneity was detected among these studies (I2 = 0%, p = 0.837). A low risk of publication bias was found (Egger test: p = 0.576) among the analyzed reports.
Positive rates of KRAS mutation
Only 1 article reported a positive rate of KRAS mutation, at 6% [20].
Discussion
In this meta-analysis, we systematically evaluated the potential clinical effectiveness of lung biopsy in molecular tests. First of all, the pooled adequacy rate for molecular tests from CT-guided biopsy was observed to be 95%. This result indicated that CT-guided lung biopsy can serve as an effective method for molecular tests. Kim et al. [23] reported that no significant differences could be found in mutant EGFR detection rates (29.5% vs. 28.9%, p > 0.05) between biopsy and resected samples. A study of surgical specimens and small tissue biopsies revealed up to 80% agreement in gene mutation analysis data of lung cancer [24].
When we performed the subgroup analyses based on the different needle types used and lesion sizes, the pooled adequacy rates for molecular tests were all found to be greater than 90% in each group. The meta-regression also indicated that both FNAB and CNB were sufficient for conducting the molecular tests. Furthermore, the adequacy rate for molecular tests was also not significantly influenced by the lesion sizes or countries of origin.
However, significant heterogeneity was detected (I2 = 86.2%, p < 0.001) for the endpoint of adequacy rate for molecular tests. Among these subgroups, significant heterogeneity was detected in the subgroups of both the needle types used, unclear lesion size, and studies conducted in Asian countries. The sensitivity analysis showed that Lian’ study [18] might be the source of potential heterogeneity. Among all included studies, only Lian et al. [18] reported the adequacy rate for molecular tests < 90%. In Lian’s study, both fine and core needles were used, and they did not report the mean size of the lesions detected [18]. Moreover, except for the needle types, lesion sizes, and countries, the other factors which might possibly influence the adequacy for molecular tests include operators’ experience, pathologists’ experience, quality of samples, and the condition of contamination by the presence of non-cancer cells [10]. Further prospective studies are still needed to evaluate the exact contribution of these additional factors.
The EGFR is over-expressed in 40–80% of patients with non-small cell lung cancer (NSCLC), especially in Asian patients [10]. It has been reported that targeted therapy using EGFR inhibitors has shown higher clinical response rates in the subgroup of patients with the following characteristics: women, non-smokers, adenocarcinoma, and East Asian origin [10, 11]. Thus, EGFR mutations have been commonly tested for patients with NSCLC.
In this meta-analysis, the pooled positive rate of EGFR mutations was 49%, which indicated that almost half of the NSCLC patients might potentially benefit from the use of EGFR inhibitor therapy. The meta-regression and subgroup analyses showed that positive rates of EGFR mutations were not associated with the needle types used, lesion sizes, or countries of origin. However, significant heterogeneity was detected (I2 = 77.7%, p < 0.001). Although the subgroup analysis revealed significant heterogeneity in the groups of core needle, mean lesion ≥ 4 cm, and Asian countries, the sensitivity analysis did not precisely indicate the particular study which was the main source of heterogeneity. Moreover, in addition to the factors mentioned above, EGFR mutations may also be attributed to gender, smoking condition, histological types and tumor stages [18].
The ALK fusion gene is another driver gene implicated in the pathogenesis of NSCLC [18]. The overall response rate of crizotinib in the phase I clinical trial on treatment of ALK positive NSCLC patients was reported to be approximately 64% [25]. In this meta-analysis, the pooled positive rate of ALK translocation was 7% without exhibiting any significant heterogeneity (I2 = 0%, p = 0.837). The low heterogeneity might be attributed to the following factors: (a) the number of included studies for determining this endpoint was relatively small; and (b) the range of the positive rates of ALK translocation was small (5% to 9%). Lian et al. [18] also found that the rates of positive ALK were comparable between FNAB and CNB groups (6.5% vs. 4%, p > 0.05). It has been previously reported that stage IV NSCLC was found to be associated with a higher rate of ALK translocation [18].
The KRAS mutation rate was only reported in 1 included study [20]. The most frequent KRAS mutations are detected in pancreatic cancer [26]. Further studies regarding the status of KRAS mutations in NSCLC are needed.
This meta-analysis has some major limitations. First, all included studies were retrospective in nature with high heterogeneity in adequacy rate for molecular testing and EGFR mutations. Although some subgroup analyses have been performed, several other important factors (such as gender, age, operator experience, tumor stage, and pathological types) which also could significantly influence the results were not included for subgroup analyses because we could not stratify the data based on these factors from the included studies. Second, significant publication bias was found in the endpoint of adequacy rate for molecular tests. It also needs to be highlighted that during the course of this study (2010–2020) there were several new developments related to biopsy procedures and techniques of molecular tests. Third, no control group was included in this meta-analysis, and therefore we could not precisely compare the CT-guided lung biopsy to other approaches that have been adopted in molecular tests.









