
Summary
Resting Pd/Pa, contrast medium Pd/Pa ratio (cFFR), fractional flow reserve (FFR), quantitative flow ratio (QFR), and instantaneous wave-free ratio (iFR) were measured in 110 intermediate coronary lesions. Mean baseline Pd/Pa was 0.93 ±0.05. Mean cFFR value was similar to FFR value (0.83 ±0.09 vs. 0.81 ±0.09; p = 0.13) and QFR (0.81 ±0.1; p = 0.69) and iFR (0.90 ±0.07; p = 0.1). A total of 46 (41.8%) vessels had FFR ≤ 0.80, 50 (45.5%) vessels had cFFR ≤ 0.83, 44 (40.0%) vessels had QFR ≤ 0.80, and 38 (34.5%) vessels had iFR ≤ 0.89. An excellent agreement between cFFR and resting Pd/Pa, FFR, QFR, and iFR was confirmed (intraclass correlation coefficients of 0.83, 0.99, 0.98, and 0.88, respectively). The optimal cutoff value of cFFR was 0.83 for prediction of FFR ≤ 0.80 with sensitivity, specificity, and accuracy of 96.9%, 97.8%, and 97.3%, respectively. 100% sensitivity was observed for a cutoff value of 0.82 and 100% specificity for a cutoff value of 0.84; AUC = 0.998 (0.995–1.00); p < 0.001.
Introduction
Fractional flow reserve (FFR) obtained after the achievement of pharmacologically induced maximal hyperemia has been demonstrated not only as a gold standard for the assessment for intermediate coronary stenosis severity in the cathlab but also as a parameter improving prognosis in terms of revascularization with a fixed cut-off value of 0.8 [1–6]. Recent data confirmed the non-inferiority of instantaneous wave-free ratio (iFR) to FFR in terms of lesion severity assessment along with long-term clinical outcomes [7, 8]. Quantitative flow ratio (QFR) assessment, on the other hand, involves an advanced algorithm that enables fast computation of pressure decreases in intermediate coronary artery disease (CAD) without any invasive physiologic measurements or pharmacologic hyperemia induction, and its diagnostic performance has already been confirmed [9, 10]. Radiographic contrast medium, routinely used during coronary angiography, has been demonstrated to induce hyperemia, e.g. during the check of pressure wire placement [11]. Pd/Pa ratio registered by pressure wire during submaximal reactive hyperemia induced by intracoronary injection of contrast medium may be sufficient for the assessment of the physiological severity of stenosis in a large number of cases, avoiding the need of adenosine administration. The CONTRAST study, comparing the ability of contrast medium Pd/Pa ratio (cFFR) to predict FFR versus resting indices, showed that cFFR was superior to resting Pd/Pa and iFR for predicting FFR while resting Pd/Pa and iFR provided equivalent diagnostic accuracy [12]. Several studies showed a good correlation of cFFR with FFR [13, 14].
Aim
In our study, we sought to investigate the performance strength of cFFR against FFR, iFR, and a novel tool, QFR, as a comprehensive assessment of intermediate CAD.
Material and methods
Patients with stable CAD with angiographically ambiguous lesions (40–90% diameter stenosis by visual assessment) in a major epicardial coronary artery, who were scheduled for FFR, were prospectively and consecutively enrolled. Baseline clinical data were collected. Ethics approval was granted from the institutional ethics review process and all patients gave written informed consent.
Study protocol
Coronary angiography was performed with the standard femoral or radial approach based on individual operator preferences. The acquisition was done at 15 fps for the best image quality. The s5/s5i console and Verrata Pressure Guide Wire (Philips Volcano Corporation, San Diego, California) were used in all cases. Data acquisition included an electrocardiographic signal recording. Firstly, the pressure wire was advanced distally to the index lesion. After confirmation of wire position and waiting until the return of Pd/Pa ratio to the baseline value, cFFR was assessed in the following pattern. A single rapid manual injection of 3 ml of radiographic contrast medium through a contrast dye filled guiding catheter (+ 2 ml additional volume of contrast dye) (Visipaque 320, GE Healthcare, USA) was performed and the minimal cFFR value obtained was recorded (in general within the first 10 s). Each injection of contrast medium was duplicated to test the reproducibility of cFFR. After any injection of contrast medium, flushing of the guiding catheter with saline was performed to avoid pressure damping due to contrast medium viscosity. The pressure wire was pulled back to the left main or ascending aorta to check for potential pressure drift. Afterwards, the wire was advanced once again distally to the evaluated lesion and after its position check, saline flush of the guiding catheter and another 60 s of wait, iFR was calculated using fully automated algorithms in a typical way [15]. After iFR assessment, we started adenosine administration through a femoral vein at a rate of 140 [µg/kg/min] for a minimum of 3 min. The detailed, meticulous methodology of the FFR/iFR procedure was previously described [16–18]. The pressure wire pullback maneuver was mandatory to check for pressure drift. Computation of QFR was performed offline, using a software package (Medis Suite 2.1.12.2, Medis Medical Imaging System, Leiden, the Netherlands) by an independent corelab analyzer blinded to iFR, FFR, and cFFR results [10, 19]. The analysis was conducted twice by each analyzer and the mean value (from four calculations) was used for further analysis. The intra- and inter-observer variability were determined using the intraclass correlation coefficient (ICC). The limited intra- and interobserver variability for measuring the QFR was confirmed by ICC of 0.991 (95% CI: 0.988–0.993) and 0.990 (95% CI: 0.987–0.992), respectively.
Quantitative coronary angiography (QCA) was performed by an independent corelab analyzer blinded to the results of FFR, using the edge detection system (CAAS 5.7 QCA system, Pie Medical).
Statistical analysis
Categorical variables were expressed as numbers of patients (percentages). Continuous variables were expressed as mean ± standard deviation (SD). Non-normally distributed data were reported as median (interquartile range (IQR)). The agreement among tested methods was assessed by the Bland-Altman plot method and ICC. Data are presented as the unadjusted area under the ROC curve (AUC) with 95% CI. All tests were 2-tailed, and a p-value < 0.05 was considered statistically significant. All statistical analyses were performed using Statistica 13.3 (TIBCO Software Inc., Palo Alto, CA, USA).
Results
Forty-four patients with 110 intermediate coronary stenoses were enrolled. Patient characteristics are presented in Table I. Lesion characteristics are shown in Table II. Mean baseline Pd/Pa was 0.93 ±0.05. Mean cFFR value was similar to FFR value (0.83 ±0.09 vs. 0.81 ±0.09; p = 0.13) and QFR (0.81 ±0.1; p = 0.69) and iFR (0.9 ±0.07; p = 0.10, Figure 1). A total of 46 (41.8%) vessels had FFR ≤ 0.80, 50 (45.5%) vessels had cFFR ≤ 0.83, 44 (40.0%) vessels had QFR ≤ 0.80, and 38 (34.5%) vessels had iFR ≤ 0.89. Resting Pd/Pa, FFR, QFR, and iFR were strongly correlated with cFFR (Figure 2). An excellent agreement between cFFR and resting Pd/Pa (ICC 0.83, 95% CI: 0.76–0.88), FFR (ICC = 0.99, 95% CI: 0.98–0.99), QFR (ICC: 0.98, 95% CI: 0.97–0.98), and iFR (ICC = 0.88, 95% CI: 0.82–0.92) was confirmed. However, cFFR showed stronger agreement between cFFR and FFR than between cFFR and iFR in Bland-Altman analysis (Figures 3 A and B). The optimal cutoff value of cFFR was 0.83 for prediction of FFR ≤ 0.80 with sensitivity, specificity, and accuracy of 96.9%, 97.8%, and 97.3% respectively. 100% sensitivity was observed for a cutoff value of 0.82 and 100% specificity for a cutoff value of 0.84; AUC = 0.998 (0.995–1.00); p < 0.001, Figure 4 A). The optimal cutoff value of cFFR was 0.84 for prediction of iFR ≤ 0.89 with sensitivity, specificity, and accuracy of 79.2%, 92.1%, and 83.6% respectively. 100% sensitivity was observed for a cutoff value of 0.73 and 100% specificity for a cutoff value of 0.91; AUC = 0.89 (0.83–0.95); p < 0.001 (Figure 4 B). The optimal cutoff value of baseline Pd/Pa was 0.93 for prediction of FFR ≤ 0.80 with sensitivity, specificity, and accuracy of 92.2%, 80.4%, and 87.3% respectively. 100% sensitivity was observed for a cutoff value of 0.85 and 100% specificity for a cutoff value of 0.98; AUC = 0.92 (0.87–0.97); p < 0.001. The optimal cutoff value of baseline Pd/Pa was 0.93 for prediction of iFR ≤ 0.89 with sensitivity, specificity, and accuracy of 91.7%, 94.7%, and 92.7% respectively. 100% sensitivity was observed for a cutoff value of 0.91 and 100% specificity for a cutoff value of 0.97; AUC = 0.98 (0.95–1.00); p < 0.001.
Figure 1
Mean values of resting Pd/Pa, contrast fractional flow reserve (cFFR) and fractional flow reserve (FFR), quantitative flow ratio (QFR) and instantaneous wave-free ratio (iFR)
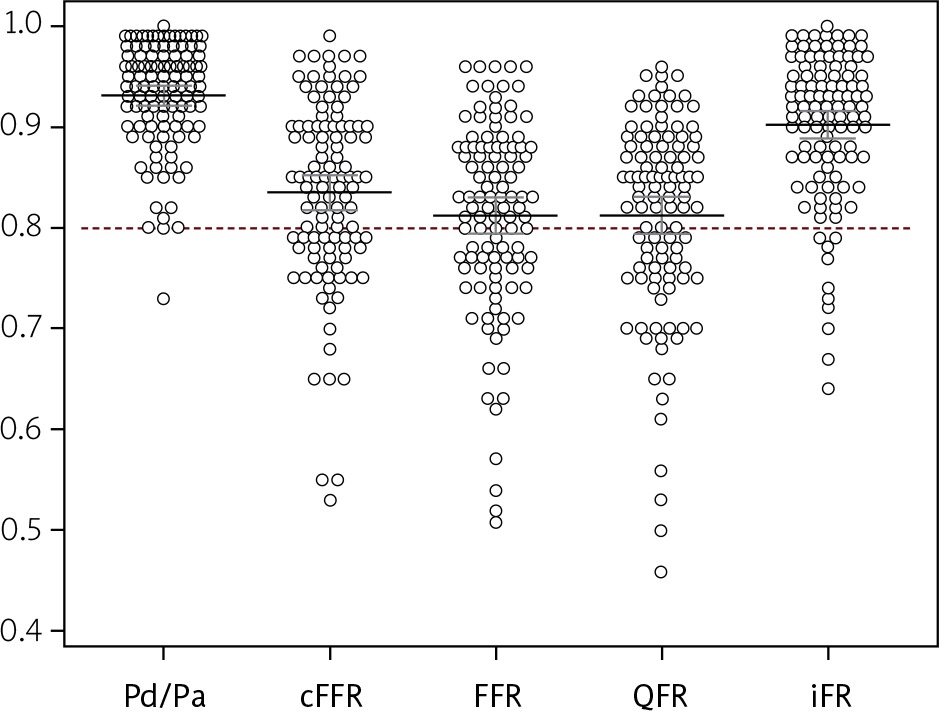
Figure 2
cFFR comparisons. Correlation between resting Pd/Pa (A), fractional flow reserve (FFR, B), quantitative flow ration (QFR, C) instantaneous wave-free ratio (iFR, D) and contrast fractional flow reserve (cFFR)
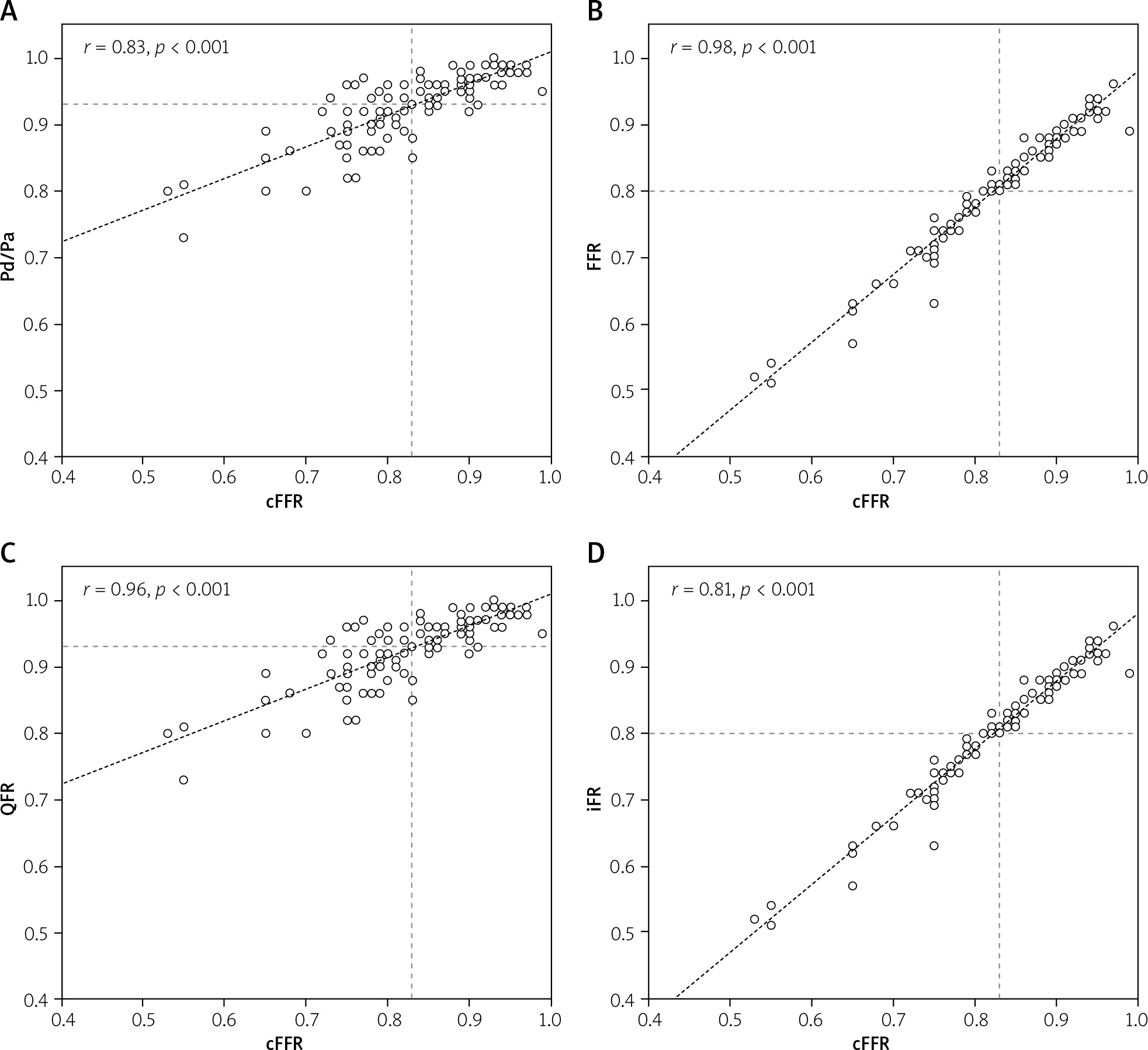
Figure 3
Bland-Altman plots for the agreement between contrast fractional flow reserve (cFFR) and fractional flow reserve (FFR, A) and instantaneous wave-free ratio (iFR, B)
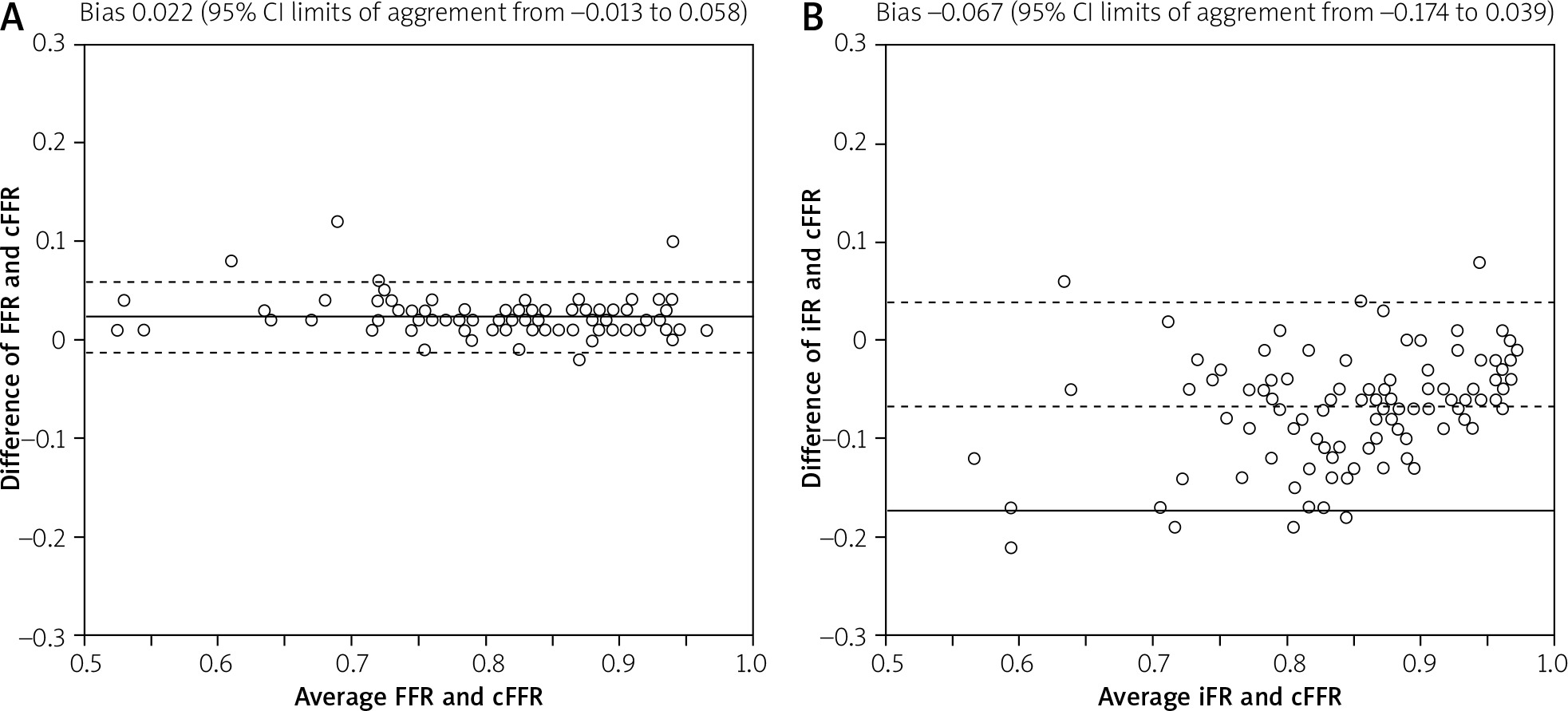
Figure 4
Receiver operating characteristic curve calculated using the threshold cut-off value of contrast fractional flow reserve (cFFR) for fractional flow reserve (FFR) of ≤ 0.80 (A) and instantaneous wave-free ratio (iFR) ≤ 0.89 (B)
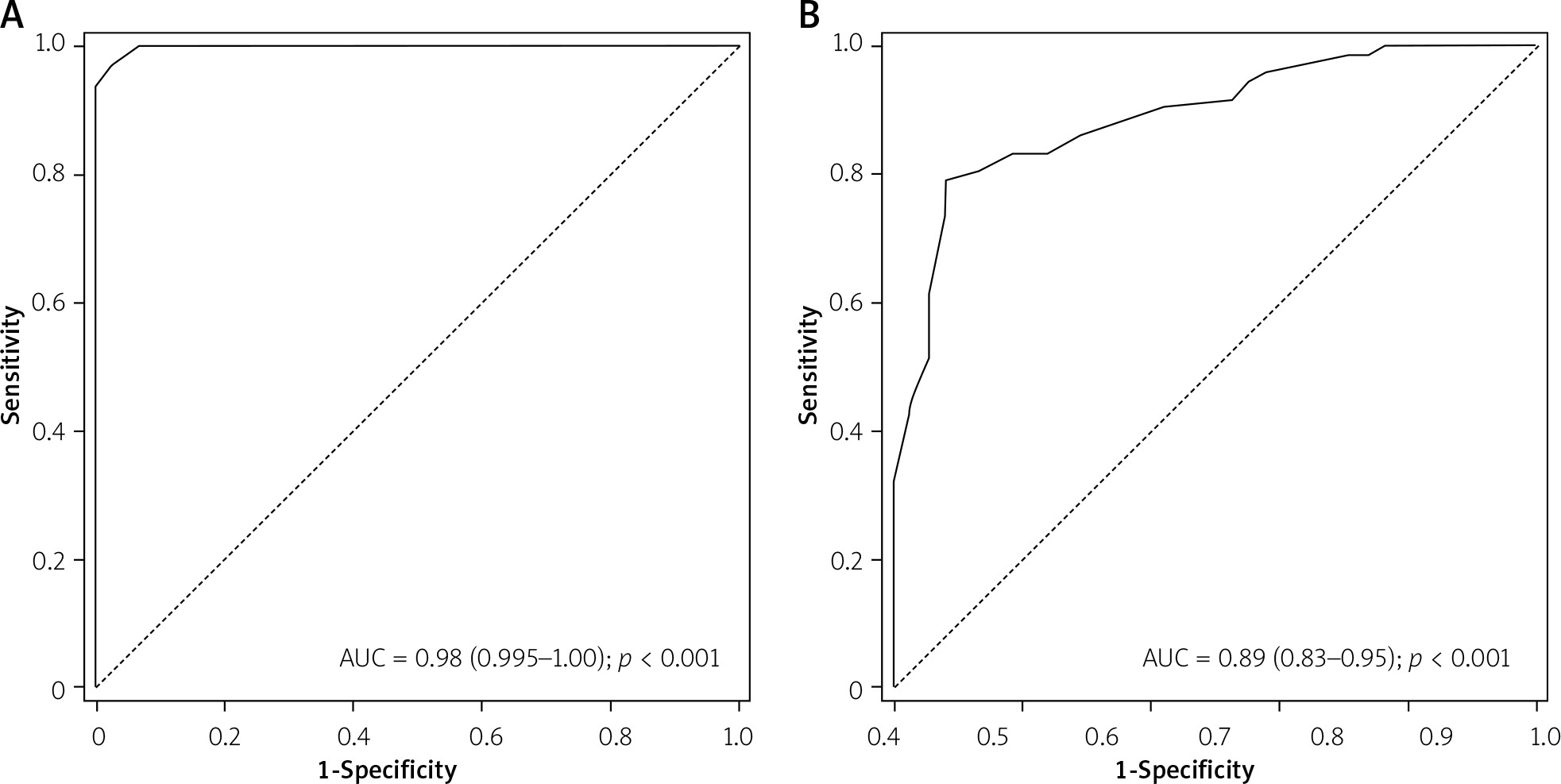
Table I
Study population and procedural data (n = 44)
[i] Values presented as number (percentage), mean ± standard deviation or median (interquartile range). CABG – coronary artery bypass grafting, CCS – Canadian Cardiovascular Society, LVEF – left ventricle ejection fraction, NYHA – New York Heart Association, PCI – percutaneous coronary intervention, TIA – transient ischemic attack.
Table II
Lesion characteristics (n = 110)
Discussion
The results of our study showed that cFFR, calculated as Pd/Pa after the induction of submaximal hyperemia using the intracoronary bolus of standard radiographic contrast dye, may be accurate in predicting FFR values of borderline coronary lesions. Moreover, cFFR is able to predict the iFR values in assessing intermediate coronary stenosis. Most interestingly, we found a significant correlation of cFFR with a novel index – QFR – which is calculated based on 3D-QCA and corrected TIMI frame count algorithms. Our results suggest that the use of the cut-off value of 0.82 for cFFR could be a reasonable option in patients who have contraindications to the administration of adenosine, or the assessment of iFR is not possible in the cathlab.
Despite its demonstrated value in guiding coronary revascularization, the rate of adoption of FFR in real-world clinical practice remains rather low [3]. FFR assessment requires maximal hyperemia induced by a vasoactive agent such as adenosine, which may cause some adverse effects during infusion or intracoronary injection (e.g. complete atrioventricular block, chest pain, dyspnea). Also, adenosine is still quite expensive. Furthermore, to overcome financial difficulties or side effects associated with the use of adenosine, a new adenosine free index based on measurement of the resting gradient called iFR was introduced. Importantly, iFR has been shown as non-inferior to FFR in terms of lesion severity assessment along with long-term clinical outcomes [7, 8]. Pd/Pa ratio registered by pressure wire during submaximal reactive hyperemia after an intracoronary bolus of contrast medium may be sufficient for evaluation of the physiological significance of stenosis, avoiding the need of adenosine administration. In the RINASCI study, a strong correlation between cFFR and FFR values was observed (r = 0.94) with a close agreement at Bland-Altman analysis (95% CI of disagreement: –0.029 to 0.072). ROC curve analysis showed excellent accuracy of the cFFR cut-off of ≤ 0.83 in predicting an FFR value ≤ 0.80 (AUC 0.97 (95% CI: 0.91–0.99, specificity 96.1%, sensitivity 85.7%)) [20]. In our study, two lesions had a cFFR value of 0.82 and another two lesions had a value of 0.83, but when assessed with FFR, the lesions were classified as non-significant (FFR value 0.83 and 0.84, respectively). On the other hand, in our study cFFR ≥ 0.88 also predicted negative FFR values (> 0.8). In the MEMENTO–FFR study, resting Pd/Pa and cFFR were significantly higher than FFR (0.93 ±0.05 vs. 0.87 ±0.08 vs. 0.84 ±0.08, respectively; p < 0.001) [21]. A strong correlation and a good agreement in Bland-Altman analysis between cFFR and FFR were observed (r = 0.90; and 95% CI of disagreement: from –0.042 to 0.11) [20]. ROC curve analysis showed excellent accuracy (89%) of the cFFR cut-off of ≤ 0.85 in predicting an FFR value ≤ 0.80 (AUC 0.95 (95% CI: 0.94–0.96)), significantly better than that observed using resting Pd/Pa (AUC = 0.90, 95% CI: 0.88–0.91; p < 0.001) [21]. In a study by Topcu et al. cFFR correlated well with FFR (r = 0.89) and showed good agreement in Bland-Altman analysis (mean bias was 0.027, 95% limits for agreement from –0.038 to 0.092) [22]. The CONTRAST study [12] compared the ability of cFFR vs. resting Pd/Pa and iFR to predict FFR. The results showed that cFFR was superior to resting Pd/Pa and iFR in predicting FFR while iFR and resting Pd/Pa provided equivalent diagnostic accuracy. In our study, the results clearly confirm that cFFR correlated strongly with FFR and QFR values. cFFR’s correlation with iFR was weaker, but still significant. In practice, it means that without the use of adenosine or any other hyperemic agent but using cFFR, a physician has a simple and always available tool to evaluate the functional significance of coronary stenosis, much better than that which we can obtain using resting Pd/Pa. Moreover, iFR assessment is not available in every cathlab worldwide. QFR showed a strong prediction ability of FFR and iFR in previous studies [9, 10, 18, 23–26]. However, QFR is assessed offline in the majority of cases and requires some time for evaluation. In a study by Sejr-Hansen et al., the authors compared online and offline QFR in patients presenting with acute coronary syndromes, yielding similar results and good diagnostic performance with staged FFR as a reference, and a moderate diagnostic performance with staged iFR [27]. In our study, surprisingly, cFFR correlated well with QFR, even more strongly than with iFR, even though QFR and iFR are both non-hyperemic methods. However, this aspect requires further investigation, as no more data so far are available.
Our study has several limitations. First, the most important limitation was the small sample size. Second, while assessing cFFR, 3 ml of contrast medium was administered manually instead of automatically. However, manual administration is more common in daily practice.







