








Introduction
Femoropopliteal in-stent restenosis (FP-ISR) is a challenging issue to treat considering the poor short-term patency and high possibility of target lesion revascularization (TLR) [1]. Debulking treatment has been attempted to improve patency by reducing the restenotic tissue burden. However, only a few studies using debulking devices have reported good results [2]. Drug-coated balloons (DCBs) are an emerging therapeutic means and several randomized controlled trials have shown their superiority compared to plain old balloon angioplasty (POBA) in FP-ISR treatment [3, 4]. The debulking of in-stent lesions may potentially improve DCB effects by reducing the thrombus or hyperplastic tissue and advancing paclitaxel dosage transit to the intima [5]. Multiple studies have demonstrated that debulking plus DCB has better results than debulking alone [6, 7], yet few studies have been published comparing debulking plus DCB with DCB alone in FP-ISR treatment. This paper aims to complete this comparison treating Tosaka III FP-ISR from our center’s experience in 1-year follow-up.
Aim
The aim of this study was to compare clinical outcomes of debulking plus DCB with DCB alone in Tosaka III FP-ISR treatment in a Chinese population.
Material and methods
Patient population and clinical characteristics
This is a single-center, retrospective study and ethical approval was obtained from the hospital review board and human investigations committee (protocol number: 2021152). Patients with Tosaka III FP-ISR lesions treated with debulking plus DCB or DCB alone from January 2017 to August 2020 were enrolled. The inclusion criteria were as follows: (1) patients aged 45 years or older; (2) subacute or chronic symptoms with Rutherford category III–IV; (3) the presence of Tosaka III FP-ISR lesions; and (4) the lesions can be treated with the available debulking devices and Acotec Orchid DCB. According to the standard protocols, the patients’ characteristics such as age, gender, morbidities, risk factors and Rutherford classification were collected. Patients with normal renal function also had computed tomographic angiography (CTA) to further assess the operation-detailed strategy including arterial anatomy, total occlusive lesions, calcified lesions, stent fracture, etc. The ankle-brachial index (ABI) measurements were taken as a physical examination.
Endovascular procedures
Before the endovascular procedure, all the patients were prescribed dual antiplatelet therapy of aspirin 100 mg/day and clopidogrel 75 mg/day for at least 3 days. Patients were treated by an experienced team in the endovascular suite under local anesthesia or intravenous sedation when necessary. During the procedures, 6–8 French sheaths were used for artery access. Retrograde popliteal or below-the-knee access was acceptable when the antegrade approach failed. True luminal or sub-neointimal recanalization was performed on in-stent total occlusions (using a 0.035 or 0.018-inch hydrophilic guidewire). Debulking devices, including a 2.3 or 2.5 mm excimer laser (Spectranetics, USA), or a 6F Rotarex catheter (Straub Medical, Switzerland), were employed at the discretion of the endovascular specialists. At least one plain balloon was used for vessel preparation before DCB dilations. All patients were treated with Orchid DCB (Acotec, China) coated with 3.0 μg of paclitaxel per mm2 and magnesium stearate as the excipient. The diameter of the DCB was equal to or 0.5 mm larger than the plain balloon. The length of all the DCBs used was sufficient to cover the entire lesions. A successful procedure was defined as residual stenosis < 30%. After DCB angioplasty, bailout stenting (including stent-in-stent and stent distally or proximately to the ISR lesion) was deployed according to the endovascular surgeon’s judgment based on the evidence of in-stent fracture and flow-limited dissection at the proximal or distal segment of the stent as to the optimal treatment of the lesions. Self-expanding stents (Medtronic, USA; Bard, USA; Biotronik, Germany) were available in diameters of 4–6 mm and in lengths up to 150 mm. Associated below-the-knee lesions were allowed to be treated with a plain balloon in order to obtain good runoffs.
Follow-up
All patients were prescribed dual antiplatelet therapy for at least 6 months after the procedure, which was changed to one agent after that. All patients underwent color coded Doppler ultrasound (CDUS) and ABI surveillance after 3, 6, and 12 months and subsequently annually after the procedure, or any time when suffering limb discomfort. The deadline for follow-up was August 2021, when the scheduled follow-up for all patients was longer than 12 months.
Endpoints and periprocedural data
The main outcome measure was 12-month primary patency defined by freedom from restenosis of the target lesion during follow-up. Restenosis was defined as > 50% diameter reduction based on the criterion of a proximal systolic peak flow velocity ratio > 2.4 detected by CDUS [8]. Other outcome measures were freedom from 12-month CD-TLR, technical success rate, periprocedural complications such as death, limb-threatening ischemia, embolization and hematoma. Lesion length and bailout stent implantation were also recorded in the procedure.
Ethics approval
The study was performed in accordance with the Declaration of Helsinki. The Institutional Review Board of Xuanwu Hospital, Capital Medical University, Beijing, China, approved the study and informed consent was waived because of the retrospective nature. Protocol number: 2021152.
Statistical analysis
Statistical analysis was performed using SPSS version 19.0 (IBM SPSS, Armonk, NY, USA). Comparison of the categorical variables between the two groups was performed using a chi-square (χ2) test (using Fisher’s test when n < 30). Comparison of continuous variables was investigated using the t-test for independent-samples. Time-to-event end-point analysis was performed using the Kaplan-Meier (log-rank) method. P-value < 0.05 indicated a statistically significant difference.
Results
Patient characteristics
Eighty consecutive patients were included in this retrospective study. All of them were successfully treated by the endovascular approach with subsequent completion of scheduled follow-up. The subjects were divided into two groups on the basis of the procedure method: debulking + DCB group (n = 39) and DCB group (n = 41). In order to distinguish the debulking approach, the debulking + DCB group was then divided into the subgroups LA + DCB and RA + DCB. Overall patients were aged between 51 and 88 years (mean age: 70.83 ±9.04 years). The baseline demographic and concomitant disease characteristics were similar in the two groups and two subgroups (Tables I and II).
Table I
Baseline characteristics in patients treated with debulking plus DCB vs. DCB alone
Table II
Baseline characteristics in patients treated with LA plus DCB vs. RA plus DCB
Follow-up results and operative details
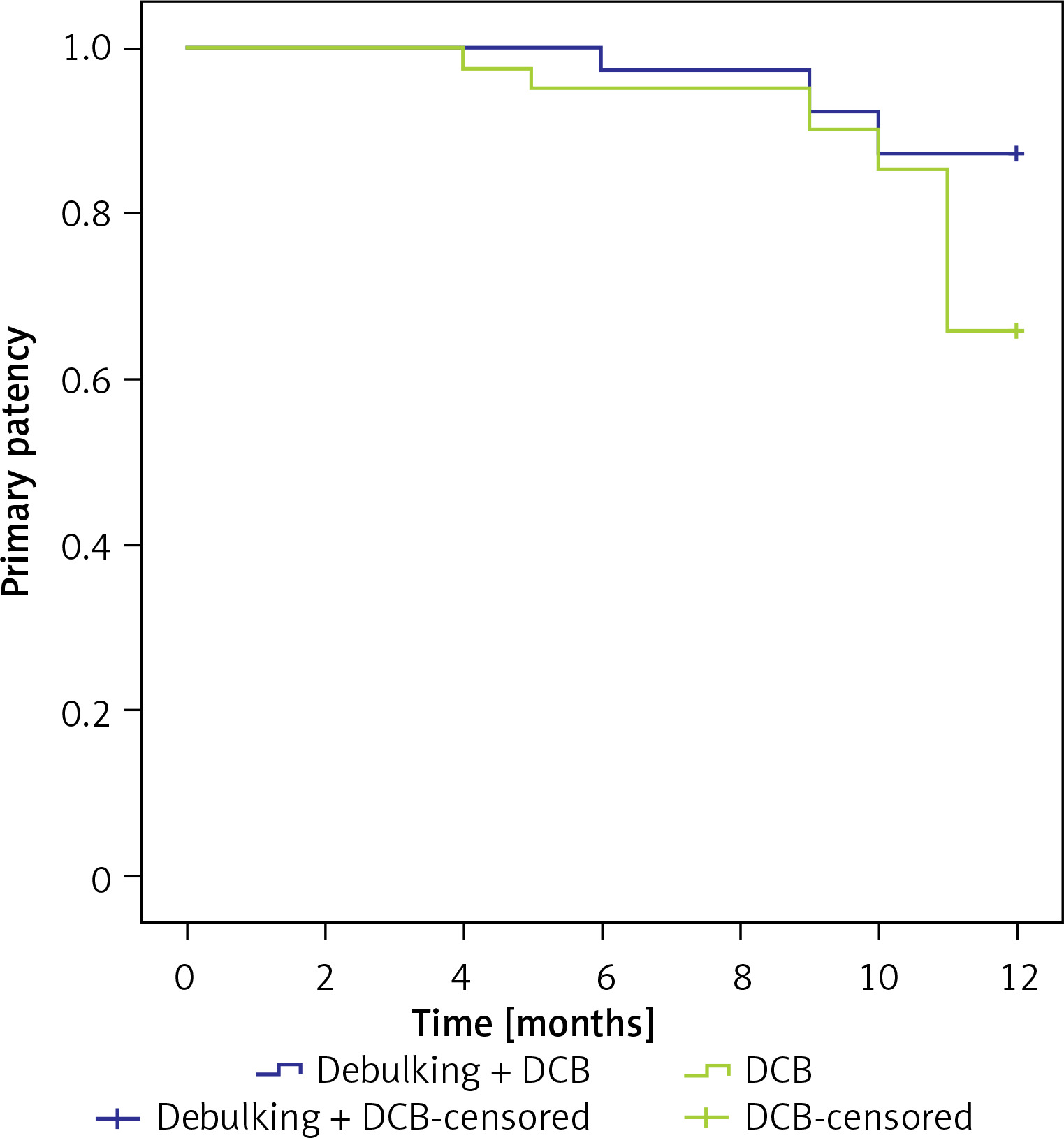
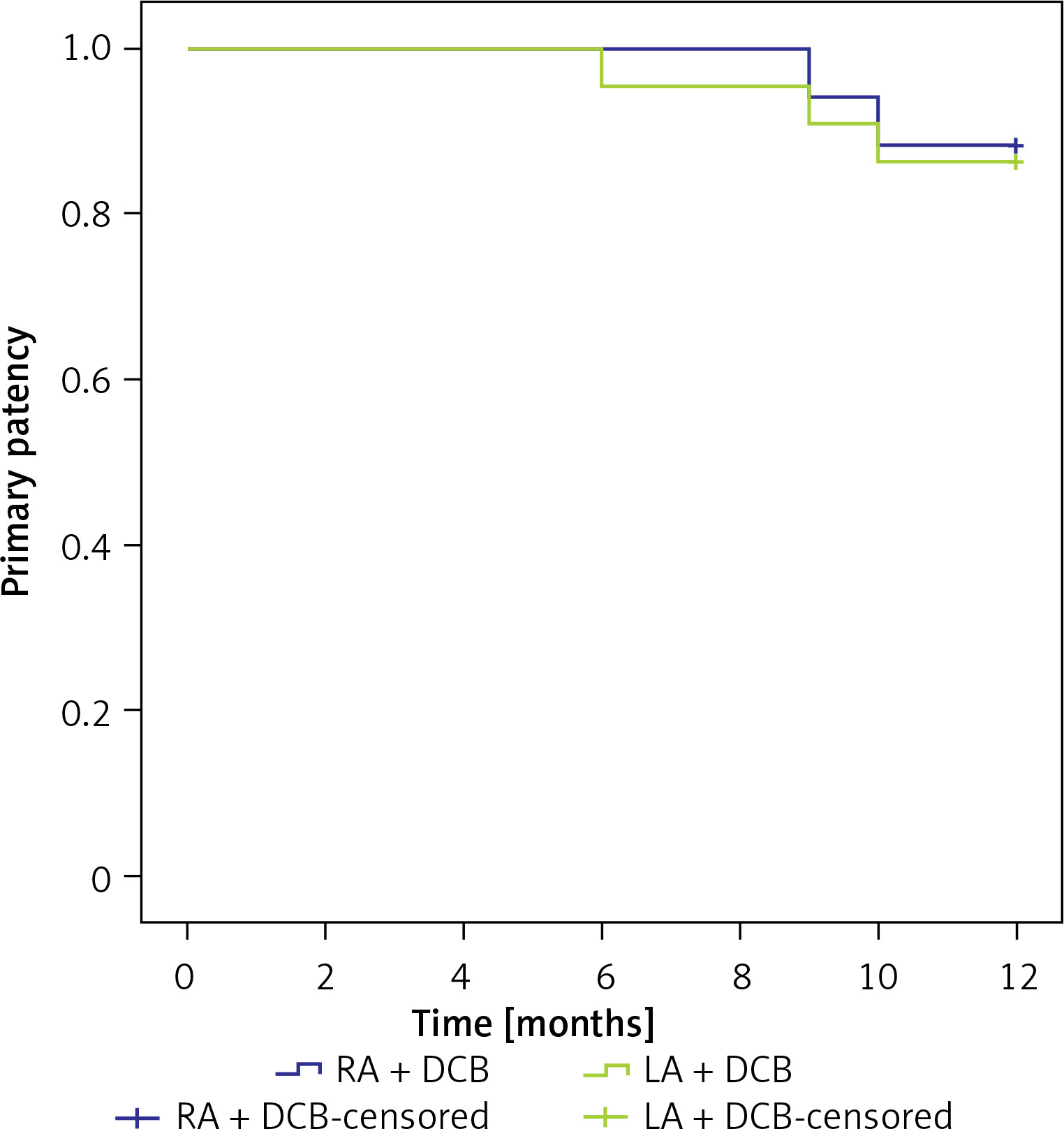
Measurement results and operative details are shown in Tables III and IV. Rutherford classification improved by at least one scale in 81.3% (65/80) of limbs at 1 year follow-up. The mean ABI was 1.00 ±0.29, increasing significantly from the baseline value of 0.55 ±0.28 (p < 0.001). The twelve-month primary patency rate was 87.2% (34/39) in the debulking + DCB group, and 65.7% (27/41) in the DCB group (Figure 1), with a significant difference (p = 0.039). In the analysis of subgroups, the 12-month primary patency rates in the LA + DCB and RA + DCB group were 86.4% (19/22) and 88.2% (15/17) respectively (Figure 2), with no significant difference (p = 0.842). There was no significant difference between the two groups and subgroups in the 12-month f-CD-TLR (p = 0.172 and 0.820). One patient suffered acute thrombosis 2 days after the procedure and received re-intervention by in-stent catheter-directed thrombosis and bailout stent. Embolization was seen in a below-the-knee artery and removed by a 4F catheter in 2 patients in the DCB group, 1 patient in the LA + DCB group, and 3 patients in the RA + DCB group. Three hematomas were all healed by conservative observation and pressure therapy.
Table III
Outcome measures in patients treated with debulking plus DCB vs. DCB alone
Table IV
Outcome measures in patients treated with LA plus DCB vs. RA plus DCB
Discussion
Tosaka III FP-ISR (in-stent occlusion) remains a significant clinical challenge for endovascular specialists compared with treatment for Tosaka I (FP-ISR < 5 cm) and II (FP-ISR > 5 cm) lesions. Stent implantation triggers reorganization of the atherosclerotic plaque and durative barotrauma to the intima layer, which leads to complex pathophysiological processes initiating smooth muscle cell migration, proliferation, and over-production of extracellular matrix. The resulting intimal hyperplasia causes in-stent lumen loss that causes the occurrence of clinical restenosis or occlusion [9]. Inadequate antithrombotic treatment, lack of response to drugs, elastic characteristics, poor below-the-knee runoff, length and fracture of the stent, and control of cardiovascular risk factors are some of the predictors associated with low patency in previous studies [10]. Although bypass surgery is still considered good treatment of Tosaka III FP-ISR, many patients are not candidates for the traditional surgery due to severe comorbidities or high surgical risk.
In 2012, Tosaka et al. reported the results of POBA for FP-ISR, proposing the Tosaka classification system to define the patterns of restenosis. In their observation, totally occluded stents (class III ISR) were associated with an increased risk of recurrent ISR/occlusion and revascularization, compared to the re-stenotic groups (classes I and II ISR). This confirms the inadequacy of POBA and the need for better endovascular techniques to improve the results in Tosaka III FP-ISR lesions.
Debulking devices, including Strub Rotarex, excimer laser, Jetstream Silverhawk and others, have been confirmed to be feasible for FP-ISR treatment with various results of primary patency and f-TLR, and superior to those of conventional POBA [11–14]. To some extent, debulking techniques could improve the results of FP-ISR treatment by acquiring more lumen gain compared with POBA. However, a systematic review and meta-analysis including 12 studies with 743 patients showed that the 12-month primary patency of debulking treatment was 58.3% and the f-TLR was 68.2% [2]. Therefore, debulking techniques still revealed relatively high restenosis rates and are not considered to be routine ISR management.
DCB, first used in percutaneous coronary intervention, delivers pharmaceutical ingredients, usually paclitaxel, to de novo or ISR lesions, which could inhibit smooth muscle cell proliferation and therefore reduce or delay the restenosis [15]. In the following years, DCB was tentatively used in the treatment of de novo or ISR FP lesions. In comparison to POBA, DCB had a higher patency rate and f-TLR at 6- and 12-month follow-up in FP-ISR management, and there was no difference in the incidence of amputation, all-cause adverse events and mortality [16]. In the IN.PACT Global Study ISR Cohort [17], a total of 131 subjects with 149 ISR lesions were included and mean lesion length was 17.17 ±10.47 cm, including 34.0% total occlusions (Tosaka III ISR). The overall 12-month primary patency was 88.7% and freedom from clinically driven TLR was 7.3%. There were no major amputations or deaths, and a low (0.8%) thrombosis rate. Moreover, several studies suggested that debulking plus DCB angioplasty has a distinct superiority compared to debulking alone [7, 18].
However, the comparisons of debulking plus DCB versus DCB alone for Tosaka III FP-ISR lesions are few. In 2013, a single-center, prospective, randomized study compared debulking using laser atherectomy plus DCB versus DCB alone including 48 patients. In the debulking + DCB group, the primary patency rate at 12 months was 66.7%, significantly higher than 37.5% in the DCB only patients [19]. The patency rate was not good and perhaps the reason could be that the early DCB product was not effective due to the fabrication process and usage method (only 1 min DCB dilatation in this study, compared to 3 min in the recent standard). In our study, the debulking + DCB and DCB groups both had good early-term patency. 12-month primary patency of the debulking + DCB group was better than that in the DCB group (87.2% vs. 65.9%, p = 0.039).
Our study has a number of limitations. First of all, selection bias cannot be completely excluded. Second, this was a retrospective study and it should be evaluated in the context of retrospective research and its limitations. In addition, it involved only a relatively small group of patients and 1-year follow-up; more subjects and longer-term follow-up perhaps might have led to different conclusions.
Conclusions
Both debulking plus DCB and DCB alone are safe and effective for Tosaka III FP-ISR lesions. Combined treatment with debulking and DCB angioplasty is correlated with better outcomes in 1-year primary patency for Tosaka III FP-ISR lesions. High-quality randomized clinical trials are needed to evaluate these two methods.