
Introduction
The COVID-19 pandemic has been going on for more than 2 years now and has changed the face of today’s world forever. High inflation, economic collapse and social isolation are the results of the emergence of a new virus type for which the world was not prepared. But COVID-19 is first and foremost a health system problem, a paralysis of the functioning medical system and a huge increase in deaths, not only directly related to the virus [1, 2].
In 2021, over half a million people died in Poland, the highest number since World War II. It should be noted that in 2021 69,000 Poles died as a result of COVID-19 infection. Therefore, it should be considered whether transforming the health system into one that primarily treats a single infectious disease will not lead to disastrous health consequences for chronic patients who are not infected with COVID-19. Delaying diagnosis and intervention has almost always irreversible life- and health-threatening consequences [1].
At present in most countries, only the most urgent surgical procedures are performed, so the overall number of operations has fallen drastically [1, 3]. Poland is no exception, but the same applies to the whole of Western Europe [4]. It is a very well-known fact that every postponement of elective cardiac surgery or cardiology intervention increases the risk that the patient’s condition will worsen [3]. Therefore, any postponed elective surgery can suddenly become an emergency surgery.
Before the upcoming 5th wave of the COVID-19 pandemic, the authors would like to analyze the past year of the pandemic, to show the real impact of the virus and the health system changes on the state of cardiac surgery care, based on reliable medical and statistical data.
Aim
The aim of the study is to evaluate patient characteristics, patient morbidity, type of procedures, length of hospital stay, early mortality, and outcomes of surgical treatment for heart diseases during 1 year of the COVID-19 pandemic compared with the corresponding pre-pandemic year.
Material and methods
This was a retrospective, observational, single-center study of 2881 consecutive patients who underwent all types of cardiac surgery procedures between 1st March 2019 and 28th February 2021. The time interval from 1st March 2019 to 29th February 2020 was designated as the pre-pandemic control period and the time between 1st March 2020 and 28th February 2021 as the COVID-19 pandemic study period.
We collected: baseline demographic data (age, sex), European System for Cardiac Operative Risk Evaluation score (EuroSCORE II), diabetes, body mass, hypertension, chronic kidney disease, extracardiac arteriopathy, chronic lung disease, left ventricular ejection fraction (EF), cardiac rhythm, Canadian Cardiovascular Society (CCS) and New York Heart Association functional (NYHA) class. Also the extracorporeal circulation time (ECC), aortic cross-sectional time (ACC), extubation time, and intensive care unit (ICU) time were recorded. The total hospitalization time, type of surgery, and the time interval between patient qualification for surgery, defined as the date of coronary angiography, and the date of admission to the cardiac surgery department were noted.
In addition, we analyzed the number of cases in each month and compared the pre-pandemic number of procedures with the heart surgery cases detected during the coronavirus period in Poland.
Endpoints
The primary efficacy endpoint was early postoperative mortality rate (< 24 h). In-hospital mortality together with in-hospital complications and length of stay in the intensive care unit (ICU) and hospital stay (HLoS) are reported.
Statistical analysis
Descriptive statistics were used and all data were reported as mean ± standard deviation or median and interquartile range (IQR). Continuous variables were tested for normal distribution using the Shapiro-Wilk test. Data were expressed as mean ± standard deviation or median (interquartile range) unless otherwise stated. To assess differences between two continuous variables, Student’s t-test (for normally distributed values) or the Mann-Whitney U-test (for non-normally distributed values) was used. Categorical variables were expressed as number and percentage. For categorical variables, the c2 test was used. Statistical analysis was performed using Statistica 12.0 (StatSoft, Tulsa, OK, USA). A two-sided p-value of 0.05 was considered statistically significant.
Results
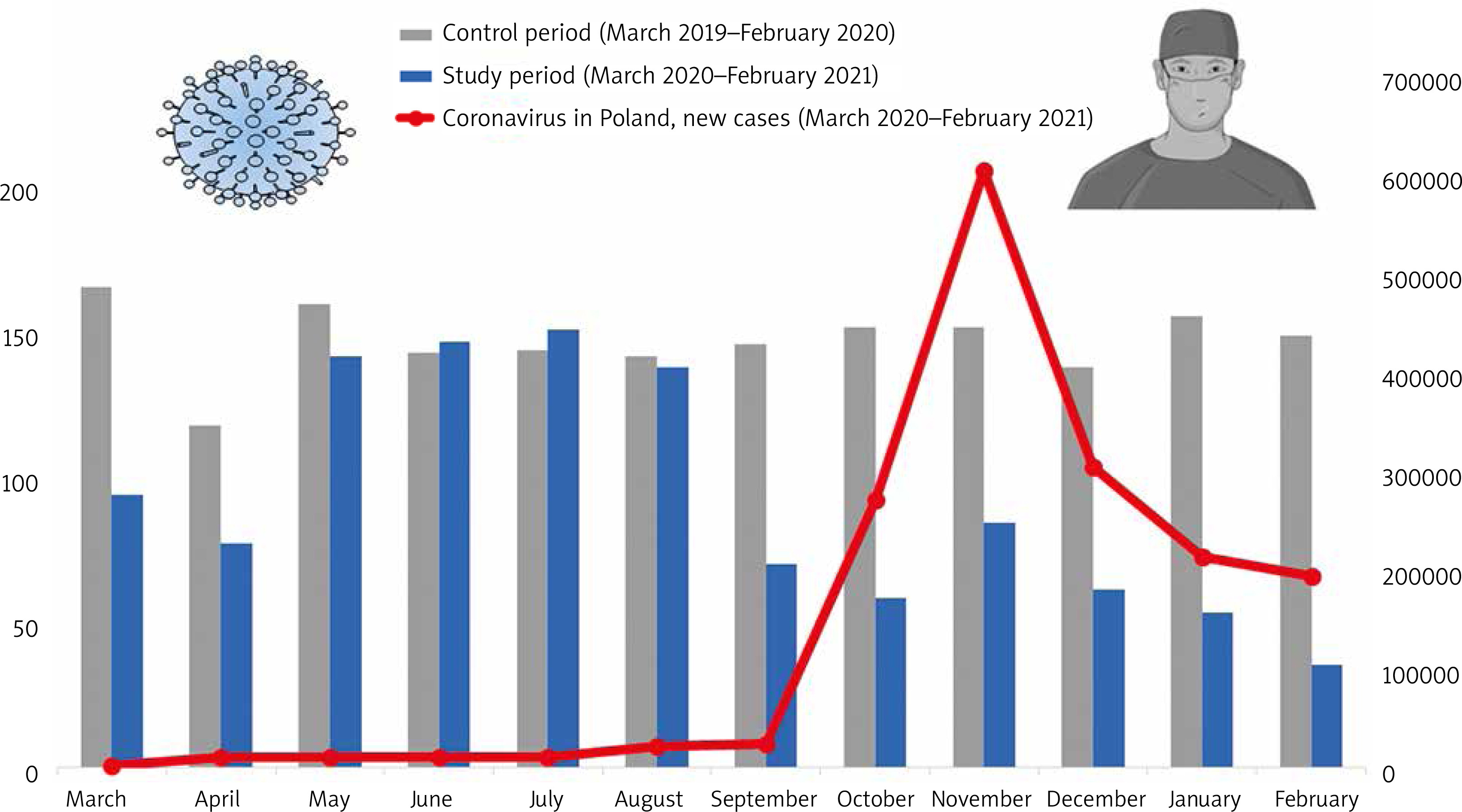
During the control period (between March 1st 2019 and February 29th 2020), the total number of all cardiac surgery procedures was 1778. Compared with the COVID-19 pandemic period (between March 1, 2020 and February 28, 2021) the total number of all cardiac surgery procedures was 1127 (decrease of 37%). A detailed direct comparison between the number of cardiac surgical procedures in each period and the new coronavirus cases detected in Poland in each month is presented in Figure 1. The lowest disproportion between the two groups was observed from May to August 2021. The highest disproportion rate occurred with the increase in viral infections in the autumn and winter months of 2021 (Figure 1).
Figure 1
Direct comparison between the number of cardiac surgical procedures in each period and the number of new coronavirus cases detected in Poland
Patients who underwent surgery during the pandemic period had a higher operative risk based on the EuroSCORE II and had a higher number of comorbidities, including diabetes, hyperlipidemia, atrial fibrillation, left ventricular ejection fraction, chronic lung disease and left ventricular stenosis. The detailed characteristics are shown in Table I.
Table I
Patients’ characteristics
| Baseline characteristics | Pre-COVID-19 period 1st March 2019 – 29th February 2020 (n = 1778) | COVID-19 period 1st March 2020 – 28th February 2021 (n = 1127) | P-value |
|---|---|---|---|
| Age (median [IQR]) [years] | 67 [61–73] | 67 [60–72] | 0.2140 |
| Male gender | 1273 (71.6%) | 811 (73.5%) | 0.2790 |
| BMI (median [IQR])[kg/m<sup>2</sup>] | 28.0 [25.3–31.2] | 27.7 [24.9–31.0] | 0.1157 |
| EuroSCORE II (median [IQR]) | 1.26 [0.90–1.92] | 1.39 [0.99–2.10] | < 0.0001 |
| Diabetes | 210 (11.8%) | 231 (22.3%) | < 0.0001 |
| Hypertension | 1702 (95.7%) | 1085 (96.3%) | 0.5736 |
| Hyperlipidemia | 982 (55.2%) | 830 (73.6%) | < 0.0001 |
| Atrial fibrillation | 95 (5.3%) | 201 (17.8%) | < 0.0001 |
| Poor mobilitya | 146 (8.1%) | 56 (5.0%) | 0.0011 |
| Severe pulmonary hypertension (PA systolic > 55 mm Hg) | 6 (0.01%) | 5 (0.01%) | 0.8854 |
| Renal impairment | 144 (8.3%) | 87 (7.7%) | 0.7658 |
| Dialysis (regardless of CC) | 5 (0.3%) | 2 (0.2%) | 0.8670 |
| Peripheral artery disease | 19 (1.1%) | 11 (1.0%) | 0.9584 |
| History of stroke/TIA | 13 (0.7%) | 9 (0.8%) | 0.6016 |
| Chronic lung disease | 1138 (64.0%) | 654 (58.0%) | 0.0014 |
| LVEF (%) (median [IQR]) | 50 [48–60] | 50 [45–55] | 0.0001 |
| LM disease | 281 (15.4%) | 290 (25.8%) | 0.0001 |
| Previous MI | 514 (28.9%) | 237 (27.8%) | 0.5359 |
| Previous PCI | 374 (21.0%) | 237 (21.0%) | 0.9656 |
| NYHA: | 0.0001 | ||
| NYHA 0 | 84 (4.7%) | 26 (2.3%) | |
| NYHA I | 764 (43.0%) | 443 (39.3%) | |
| NYHA II | 851 (47.9%) | 554 (49.2%) | |
| NYHA III | 54 (3.0%) | 58 (5.1%) | |
| NYHA IV | 44 (2.5%) | 42 (3.7%) | |
| CCS: | 0.0001 | ||
| CCS 0 | 92 (5.2%) | 109 (8.9%) | |
| CCS 1 | 627 (35.3%) | 332 (27.1%) | |
| CCS 2 | 951 (53.5%) | 528 (43.0%) | |
| CCS 3 | 65 (3.7%) | 107 (8.7%) | |
| CCS 4 | 24 (1.3%) | 38 (3.1%) | |
| ACS | 19 (1.1%) | 13 (1.1%) |
a Defined according to EuroSCORE II as severe impairment of mobility secondary to musculoskeletal or neurological dysfunction;
IQR – interquartile range, BMI – body mass index, PA – pulmonary artery, CC – creatinine clearance, TIA – transient ischemic attack, LVEF – left ventricle ejection fraction, CAD – coronary artery disease, VD – vessel disease, MI – myocardial infarction, PCI – percutaneous coronary intervention, NYHA – New York Heart Association, CCS – Canadian Cardiovascular Society, ACS – acute coronary syndrome.
During the COVID-19 pandemic period, the average waiting time for surgery was 76 days in comparison to 54 days in the non-pandemic period, i.e. 22 days longer (40.7% increase). There were 184 emergency operations performed during the non-COVID-19 period and 433 emergency operations in the pandemic period, i.e. 249 more operations (135% increase) (Table II).
Table II
Comparison of hospitalization factors between March and February in each year
Discussion
The COVID-19 pandemic is one of the most dramatic events of the 21st century, claiming millions of lives around the world. As we write this article, we are facing the 5th wave of the pandemic and the number of virus infections is increasing daily. Compared to the first year, the pandemic peak of COVID-19 has shifted by several months in the second year of the pandemic. In addition, a new variant of the virus has emerged, Omicron, with a higher incidence potential. In Poland, more and more units are being converted into departments that exclusively treat COVID-19 patients. Unfortunately, due to the severe course of the disease, many more intensive care beds are being allocated for patients with severe COVID-19. In Poland, according to government data, on 21 January 2022, 46% of all available respirators were already occupied by patients with COVID-19. Unfortunately, some of these respirators belonged to cardiac surgery departments before the pandemic. It should be noted that many cardiac surgery departments were forced to postpone all non-emergency admissions and procedures due to local COVID-19 restrictions [3].
Cardiovascular diseases are the most common cause of death in Poland. Thanks to the high level of health care, a large number of cath labs and the availability of cardiac surgery centers, the percentage of cardiovascular deaths has systematically decreased. This is the merit of the entire healthcare system, including us – cardiac surgeons [5].
The cardiac surgery patient belongs to a special group of patients that requires special attention. These patients need specialized treatment in a highly qualified center with access to modern forms of cardiovascular therapies [6, 7]. A cardiac surgery patient also needs intensive care in the postoperative period, and the patient’s convalescence involves many specialists from different fields: anesthetists, cardiologists, nurses, scrub nurses, physiotherapists, psychologists and medical technicians [8, 9]. The COVID-19 pandemic has forced a reduction in the number of operations, the transfer of some staff to newly established units and the provision of some medical equipment (e.g. ECMO machines) to fight the coronavirus [3]. As the pandemic progressed, the waiting time for admission to the cardiac surgery unit increased from several weeks to several months. While waiting for surgery, the patient’s condition deteriorates, which means that we operate later on very stressed patients with a higher surgical risk. As we warned in our previous paper, longer times between the beginning of symptoms and hospital admission leads to a higher risk of ischemic lesions [1]. If the patient is not stable he or she needs to be admitted immediately, and usually it is already a little late, which might lead to complications and require a longer stay in the intensive care unit. A longer stay in the ICU blocks the next planned operations, increasing the waiting time. In many departments this is very difficult situation.
The authors would like to emphasize that the data presented in the results section are from a non-COVID-19 hospital in a macroregion with one of the highest incidence rates of COVID-19 in Poland [10]. However, unlike other larger provinces, there is only one adult cardiac surgery center in Lesser Poland. Therefore, every case of an infected COVID-19 patient on the surgical department temporarily paralyzed the work of the cardiac surgery department [11]. Nevertheless, help for the patients was provided without interruption. Importantly, we were able to show that, after the peak of the COVID-19 pandemic, the hospitalization rates returned to those observed in previous years in the same periods or it was even higher in the months when infection levels were low. Considering the data published by other authors, the fact that there was no increase in admissions may suggest more deaths of unmanaged patients at home during the lockdown periods [4, 11].
We must ask ourselves what we should expect after the COVID-19 pandemic period. We believe that there will be many patients treated at increased surgical risk, with much worse symptoms of their cardiac disease and probably a worse long-term prognosis. It may turn out unfortunately that the percentage of deaths from cardiovascular diseases will significantly increase.
Conclusions
We have confirmed a sharp decline in the number of cardiac procedures performed in the first year of the COVID-19 pandemic in comparison to the pre-pandemic times. Patients waited much longer for surgery and had a higher surgical risk during the pandemic period. Urgent interventions were performed much more frequently during the COVID-19 pandemic.









