
We present a case of a 59-year-old man referred to a tertiary cardiology centre for further investigation and treatment from a local hospital. He had a background of dilated cardiomyopathy. He underwent implantation of cardiac resynchronization therapy with a defibrillator (CRT-D) system in another hospital for secondary prevention of sudden cardiac death 18 months before (Figures 1 A, B). The patient reported an intermittent pricking sensation in the left side of the chest for the previous 12 months. The device interrogation showed unstable R-wave sensing values in the range 1.3–2.6 mV and gradually increasing stimulation thresholds on the right ventricular lead (RVL) for the previous 6 months. Impedance trends on all leads were within the normal range and stable. The patient had a single inappropriate shock due to lead noise, followed by right ventricular lead capture loss 2 weeks before the admission.
Figure 1
A, B – Chest X‑ray before the procedure. Lateral projection (B) view suggests a perforation of the heart by cardioverter-defibrillator lead Durata 7122Q65 located on the free wall of the right ventricle (arrow). C, D – Cardiac CT: MPR of right ventricle wall perforation (C) and VRT reconstructions of right ventricle lead perforation (D). Visible tip of the right ventricular lead adjacent to the border of the third bronchopulmonary segment and the lingula of the left lung, with no pericardial effusion or pneumothorax. Image of “dry” cardiac perforation through the cardioverter-defibrillator lead protruding beyond the myocardium by approximately 30 mm (C, D). Arrows indicate lead tip localized externally to the heart and pericardium
CIED – cardiac implantable electronic device, CT – computer tomography, MPR – multiplanar reconstructions, VRT – volume-rendered technique.
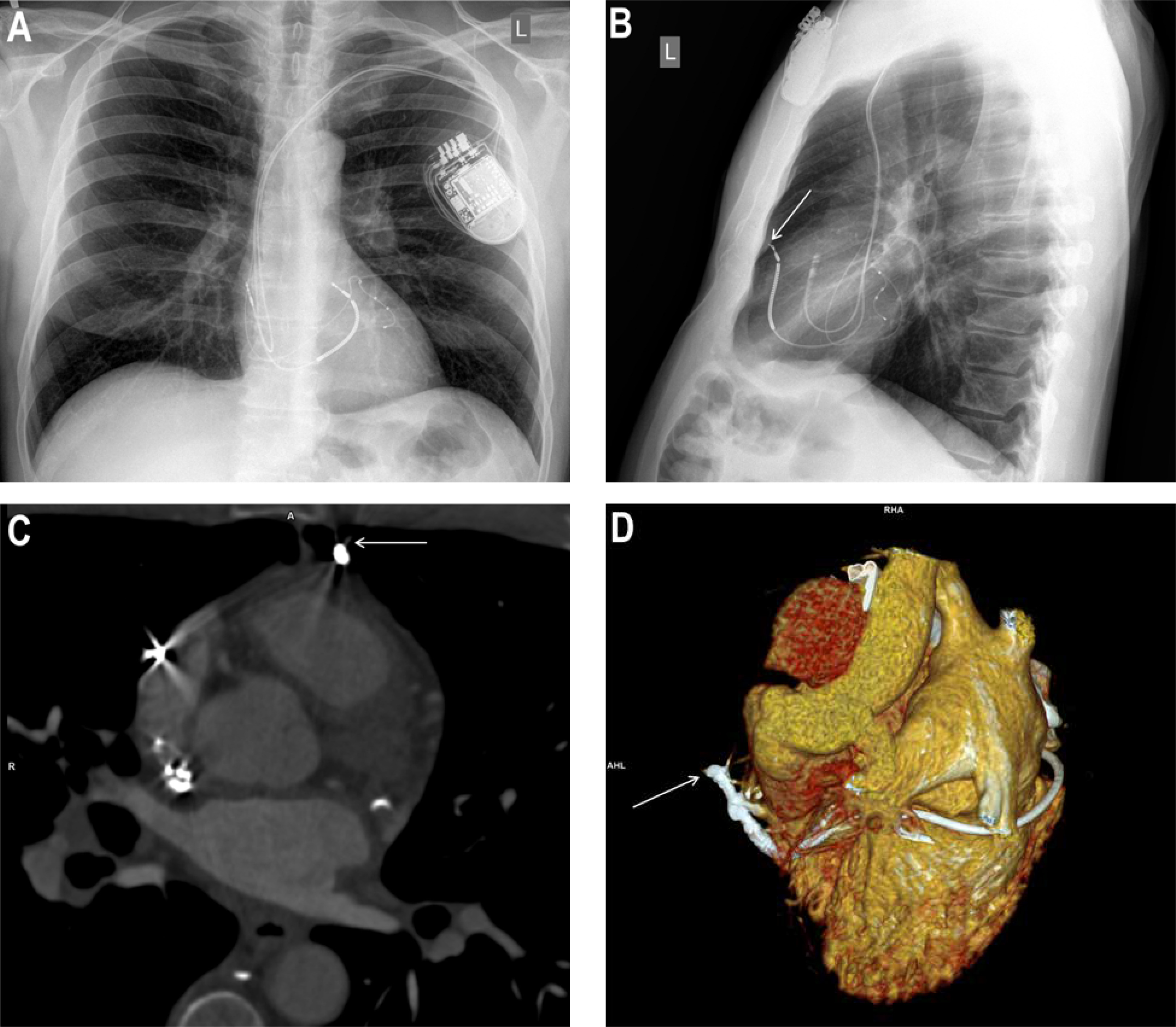
Chest X-ray was suspicious of cardiac perforation with a RVL (Figure 1 B). In transthoracic echocardiography, no increase in the pericardial fluid was observed. In cardiac computed tomography, the tip of the RVL was visible adjacent to the border of the third bronchopulmonary segment and the lingula of the left lung. There was no pericardial effusion or pneumothorax (Figures 1 C, D).
After discussing the possible therapeutic options, the patient agreed to have transvenous extraction of the perforating RVL with simultaneous implantation of a new lead. The procedure was done under general anaesthesia with intraoperative transoesophageal monitoring and a cardiothoracic surgeon on standby. The left subclavian vein accessed, and green polypropylene Byrd dilator sheaths (10.0/12.1F) were used to separate the lead from the adhesions. Intraoperative damage to the atrial electrode was found, so it was extracted using a green Byrd dilator sheath. Then, a new right ventricular cardioverter-defibrillator lead was implanted in the right ventricular apex, and an atrial lead in the right atrial appendage. The procedure was uneventful. No pericardial effusion was present before, during, or after the procedure.
The patient was discharged in stable condition. During more than 3 years of follow-up, the patient remains in good health, and a recent device check showed stable electrical parameters of all leads.
Lead perforations (LP) are rare (0.50%) but serious complications of cardiac implantable electronic device (CIED) implantation [1]. LP following CIED lead implantations are divided into acute (≤ 24 h), subacute (< 1 month), and delayed (> 1 month), according to their occurrence following implantation [2]. The rate of iatrogenic cardiac tamponade after CIED implantation is about 0.20% [3]. Delayed LP tends to present with lower rates of cardiac tamponade due to the self-sealing properties of the ventricular wall by muscle contraction, haemostasis, and subsequent fibrosis [4]. Risk factors for procedure-related iatrogenic cardiac perforation include apical or free wall placement of the RVL, over-torquing active fixation leads, and excessive lead slack as well as little experience of the operator [1]. The 2021 European Society of Cardiology pacing guidelines recommend placement of the lead in the mid-ventricular septum in patients at high risk of perforation, and the use of multiple fluoroscopic views to locate the lead in the right ventricle [5]. In this case, the most likely cause of the right ventricular free wall perforation was improper placement of an ICD lead on the free wall of the right ventricle combined with over-torquing its active fixation mechanism, which remained unrecognized during the implantation time (Figure 1 B).
Chest radiography is not an accurate method for identifying lead perforation. Cardiac computer tomography has been considered the gold standard in the diagnosis of myocardial lead perforation [6]. Because cardiac perforation is an infrequent complication, there is still controversy regarding the optimal therapeutic strategies. We show that transvenous lead extraction of delayed cardiac perforation can be safely performed in a hybrid operating room with cardiosurgical backup.







