




Introduction
Pre- and peri-operative evaluation plays a crucial role for the survival of the patient and to date many studies have been conducted in order to find effective strategies to improve mortality and morbidity [1]. In this study we investigated the reduction pathways of risk factors in coronary bypass patients via two biomarkers (copeptin and NT-proBNP) with respect to EuroSCORE II [2].
The European System for Cardiac Operative Risk Evaluation Score II (EuroSCORE) is based on the results of 19 000 cardiac surgery procedures and is currently utilized in pre- and peri-operative risk evaluation. EuroSCORE I was launched in 1999 and revised as EuroSCORE II in 2012 [1, 2]. The scoring system is still claimed to be valid for Taiwan individuals but not applicable for Chinese and Indian citizens who have had valve surgery [3–5]. The Society of Thoracic Surgeons (STS) might have the most comprehensive database among all scoring systems with a population of over 80 000 patients due to its over 800 member institutions worldwide [6].
If the correlation of the scoring system is analyzed in terms of biomarkers we do not detect any clinically significant predictive biomarker. No differential scoring subgroup is available in EuroSCORE on isolated coronary bypass surgery patients. If we prefer to utilize STS scoring we can leverage adenosine diphosphate (ADP) inhibitors, angiotensin receptor blockers (ARBs), glycoprotein IIb/IIIa and routine hemogram parameters. Regarding all these one can definitely claim that a predictive biomarker is an unmet need in this therapeutic area.
Before the cardiac settlement the physician can make use of certain agents in the circulation in order to have guidance on heart failure, cardiac ischemia and organ dysfunction including renal, cerebral, pulmonary or splanchnic dysfunction. In general there are two major parameters to monitor: inflammation and stress (both oxidative and general). The presence of an inflammatory state, increased hormones due to general stress and probable oxidative stress during bypass should be investigated before the operation. As a standard procedure troponin levels and brain natriuretic peptides (BNP) are routinely processed in each institution. BNP is initially synthesized from preproBNP, further cleaved to proBNP, and subsequently to the biologically active BNP and the inactive N-terminal prohormone-B-type natriuretic peptide (NT-proBNP). Copeptin and NT-proBNP may be classified as new compared to troponin and BNP but there is still room for novel biomarkers to implement for a dynamic response during the pre- and peri-operative period to utilize as a window of opportunity. Biomarkers not only guide the surgeon during bypass but they also provide clues for the prognosis of the patient and the medical team [7].
Copeptin and NT-proBNP have been investigated in order to identify the risk of cardiovascular diseases in previous studies. Although these biomarkers have been analyzed separately, studies investigating both of them in a single protocol are limited.
Aim
In this study we aimed to interpret copeptin and NT-proBNP levels in patients who had undergone coronary surgery with respect to EuroSCORE. The predictivity of copeptin and NT-proBNP levels for mortality and post-operative complications have been evaluated in isolated cardiac surgery cases.
Material and methods
This retrospective study was conducted between January 2017 and January 2020 with 680 individuals who had undergone cardiac surgery. Only patients who were eligible for an isolated coronary operation (n = 484) were enrolled for further analysis. Cases of valvular surgery, aortic surgery, prophylactic intra-aortic balloon pump usage before coronary vascularization, and coronary vascularization after myocardial infarction were excluded from the study. All cases of elective coronary surgery were included in our study. Samples of copeptin and NT-proBNP were collected prior to surgery. The EuroSCORE II values, pre-operative baseline demographics (age, gender, BMI) and post-operative clinical parameters (inotropic drug usage, duration of bypass operation and intra-aortic balloon pump (IABP) utilization) were obtained from the hospital patient registry (Table I).
Table I
Baseline demographics of the patients
We investigated the correlation between pre-operative copeptin and NT-proBNP levels with respect to mortality and post-operative complications via EuroSCORE II in the 484 enrolled patients. In terms of analyzing mortality the first 30 days were taken into account and duration of hospital stay was considered for prognosis. The statistical significance of copeptin and NT-proBNP with respect to EuroSCORE II ≥ 2 was studied.
Blood sampling and biomarker measurements
Blood samples were obtained from all patients and were processed within the same day. Automatic measurements were conducted in order to analyze copeptin via a Roche Cobas 800 Diagnostics (Mannheim, Germany) device. The levels of NT-proBNP were measured via an electrochemical irradiation method with a Cobas E4111 (Roche Diagnostics, Mannheim, Germany) device.
This retrospective study has been reviewed and approved by an ethics committee and informed consent has been obtained from all the enrolled patients.
Statistical analysis
The patient data were analyzed via the program IBM SPSS for Windows 23.0. Categorical data of frequency, percentage and median were identified as descriptive values. The Mann-Whitney U test was utilized in the comparison of groups and the c2 test for the comparison of categorical variables. In terms of survival EuroSCORE, NT-proBNP and copeptin threshold values were evaluated by ROC analysis. Factors affecting survival were evaluated via Cox regression analysis. A p-value < 0.05 was accepted as statistically significant.
Results
Pre-operative age, hypertension, EuroSCORE, NT-proBNP and copeptin parameters all showed statistical significance in terms of mortality analysis. The median copeptin levels were 60 pmol/l in alive individuals and 287 pmol/l in mortality cases (p < 0.0001). These values for NT-proBNP were 1011 pg/ml and 1325 pg/ml respectively (p = 0.005). Statistical significance was also found for EuroSCORE, HT and age (p < 0.005) (Table I).
Post-operative parameters such as arrythmia, inotropic drug usage, IABP, extubation period after operation, and duration of bypass surgery all affected mortality. The duration of bypass surgery for alive patients was 90 minutes versus 113 minutes for mortal cases.
The extubation period was 10 hours versus 24 hours respectively. When applied to IABP it was found that there were 11 subjects versus 3 subjects, 87 subjects versus 8 subjects for inotrope medication and 9 subjects versus 2 subjects for arrythmia respectively (Table II).
Table II
Post-operative outcomes
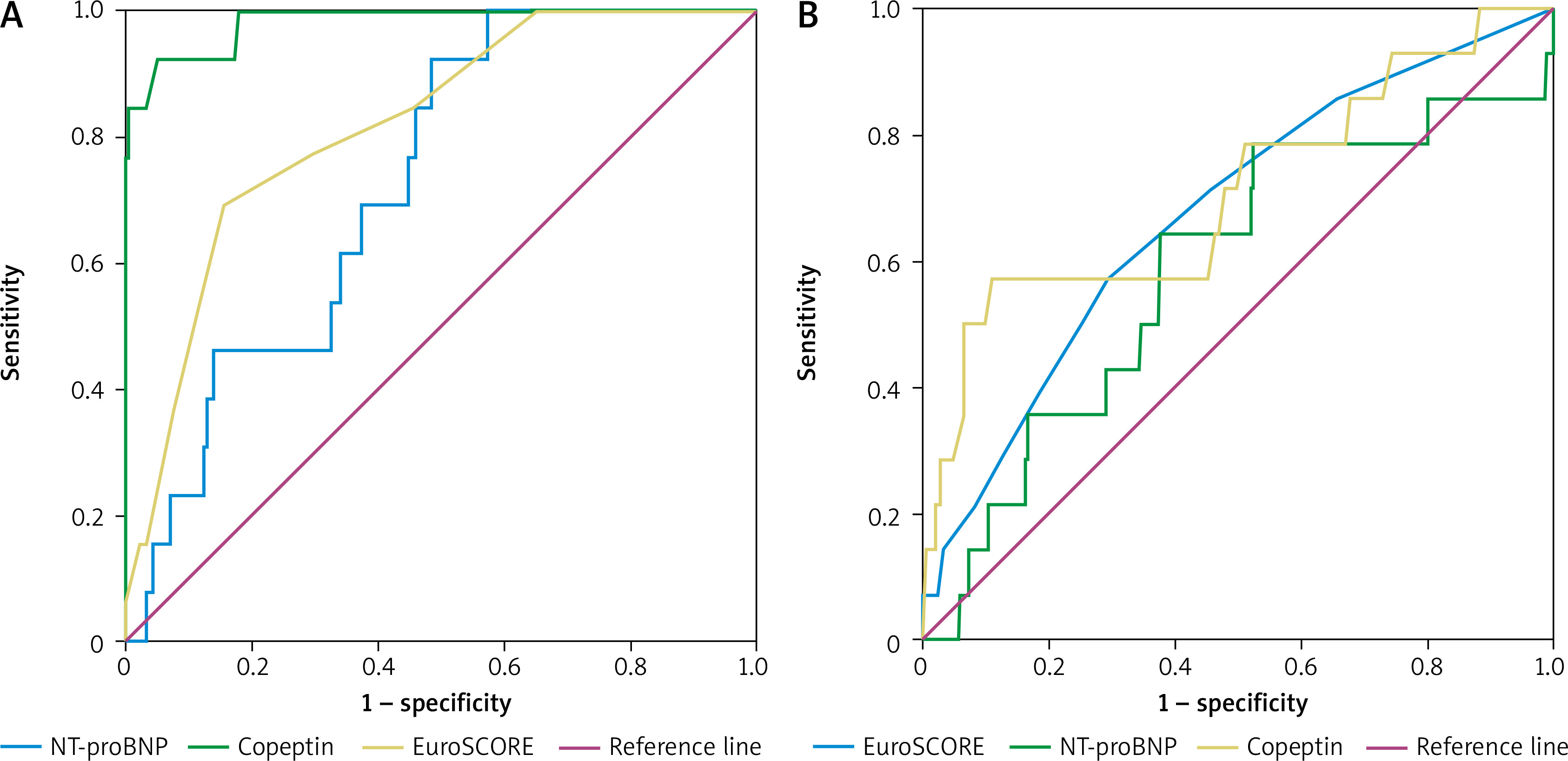
The effects of EuroSCORE, NT-proBNP and copeptin on mortality are shown in Table III via ROC analysis. The threshold value for EuroSCORE was 2, for NT-proBNP was 1296 pg/ml and for copeptin was 116 pmol/l. When the same analysis was conducted in patients using IABP, the threshold value for EuroSCORE was 2, for NT-proBNP was 1241 pg/ml and for copeptin was 110 pmol/l (Table IV).
Table III
Results of ROC analysis in terms of survival with respect to IABP utilization, EuroSCORE, NT-proBNP and copeptin levels
Table IV
Results of ROC analysis with respect to IABP utilization, EuroSCORE, NT-proBNP and copeptin levels
The Cox regression analysis revealed that death risk increased 1.13-fold with 1 year older age, 5.46-fold with inotrope medication, 10.01-fold with the use of IABP (the survival graph for mortality (a) and IABP (b) is shown in Figure 1), 1.04-fold with extubation period and 1.02-fold according to the duration of bypass surgery (Table V).
Table V
Risk factors affecting patient survival
Mortality increased 9.04-fold in cases with EuroSCORE ≥ 2, 5.04-fold when NT-proBNP level was > 1296 pg/ml. A dramatic outcome was observed in copeptin levels as mortality increased 138.17-fold when copeptin was > 116 pmol/l.
Discussion
In this research, the mean NT-proBNP and copeptin levels in mortal cases showed statistical significance. In this study the mean NT-proBNP level was 1325 pg/ml in mortal cases, thus showing statistical significance. The critical threshold level of mortality for NT-proBNP was 1296 pg/ml and for copeptin was 116 pmol/l in patients whose EuroSCORE II ≥ 2. Mortality increased 9.04-fold in cases with EuroSCORE ≥ 2, 5.04-fold when NT-proBNP level was > 1296 pg/ml. We also observed a strong correlation of copeptin and NT-proBNP with mortality and utilization of intra-aortic balloon pump.
Mortality is the major parameter not only for the patients but also for the surgeon and the whole medical team. Due to this, an objective risk stratification system needs to be developed as it will increase the detection of high risk patients and will provide better outcomes. This attribute is highly crucial as insufficient operation results may lower the performance of surgeons in future procedures. Certain tools such as EuroSCORE, STS score and Parsonnet have provided satisfactory results for pre-operative cases and on the other hand some biomarkers (ST2, galectin-3, NT-proBNP, cystatin C, IL-6 and IL-10, NGAL, TIMP2, IGFBP7) have been utilized to monitor the post-operative period [8, 9].
BNP is primarily produced by cardiac myocytes and its main duty is peripheral vasodilatation. BNP provides this physiological effect by inhibiting renin angiotensin production. The precursor peptide proBNP is split into the active hormone BNP and the NT-proBNP. Both BNP and NTproBNP are established markers for cardiac failure. Apart from cardiac failure increased levels of BNP are also observed in myocarditis, atrial fibrillation, acute coronary pathologies and chronic obstructive pulmonary disease. In contrast, BNP has been shown to decrease in obese individuals and increase in older age and females. Elevated BNP levels are prognostic markers of mortality in patients with myocardial infarction, cardiogenic shock, and pulmonary embolism [9].
The changes of plasma osmolarity in the direction of reduced cardiac output or decreased blood volume cause a rapid response in the hypothalamus and vasopressin (AVP) is secreted into the circulation. Due to its vasoconstrictive effect AVP levels are increased in several endocrinological and circulatory disorders such as trauma and oxidative stress. Regarding these physiological properties one can assume that AVP should be used as a predictive biomarker in the peri-operative stage. However, AVP measurements could not be routinely processed due to its low short half life and instability to temperature. Instead of AVP, copeptin, the C-terminal part of pre-proAVP is a more stable peptide both in plasma and during storage, and thus easier to measure. As copeptin is secreted in equimolar amounts as AVP it can accordingly be used as a surrogate for AVP release [10].
Holm et al. found strong correlation between copeptin levels and all-cause mortality in chronic heart failure patients. Increased copeptin has been an indicator of poor prognosis. This was applicable for all stages of subjects in the NYHA classification. They stated that elevated levels of copeptin were best predicted by natriuretic peptides and kidney function. Holm et al. evaluated the reliability of copeptin with NYHA functional class I to IV, BNP levels from 3 to 8.536 pg/ml, and concluded that it is as reliable as BNP [10]. Apart from Holm et al., in our research we focused on isolated coronary bypass patients but both studies emphasized the value of copeptin as a predictive biomarker. According to Holm et al. copeptin was independently related to mortality in each symptomatic stage of heart failure; it was most compelling in NYHA functional classes II and III. This is an important finding because NYHA functional classes II and III, the intermediate classes, are more difficult to judge in the ambulatory setting than the more obvious NYHA functional classes I and IV [10].
Previously the threshold value for preoperative NT-proBNP was identified as 1028 ng/l as a predictor of both postoperative severe circulatory failure and in-hospital mortality. Both pre- and post-operative NT-proBNP ≥ 1028 ng/l could be interpreted as a sign of circulatory problems even more predictive than echocardiographic assessment of left ventricular function [11, 12]. In an observational longitudinal study of 365 patients with acute coronary syndrome (ACS) undergoing isolated coronary artery bypass graft (CABG) EuroSCORE II provided satisfactory outcomes but combining EuroSCORE II and pre-operative NT-proBNP appears to improve risk prediction [13]. They also conducted a long term follow-up analysis over several years and were able to identify the cause of death in 37 of 39 subjects. The Kaplan-Meier graph was significantly worse for those with NT-proBNP ≥ 1028 ng/l (p = 0.002) [13].
In this study the mean NT-proBNP level was 1325 pg/ml in mortal cases, thus reaching statistical significance. We also observed a strong correlation of copeptin and NT-proBNP with mortality and utilization of an intra-aortic balloon pump. This situation was elaborated in Cox regression analysis graphs.
The first meta-analysis to compare the predictivity of copeptin and NT-proBNP was conducted by Zhong et al. in 2017 [14]. They analyzed 10 prospective cohort studies including 4473 patients and found that elevated copeptin level was associated with increased risk of mortality in heart failure. Two other meta-analyses have investigated the predictive role of copeptin alone. Yan et al. summarized 8 cohort studies in which elevated plasma copeptin level in HF patients was associated with mortality and the HR was 1.76 (95% CI: 1.33–2.33) [15]. Similar associations have been identified between liver enzyme markers and the risk of coronary heart disease [16]. The MASHAD study on the risks of heart disease in Iran showed that not only are fasting serum glucose and lipid profile associated with cardiovascular event outcome, but also high fasting glucose levels are strongly associated with cardiovascular events in this population [17]. Another study conducted by Zhang et al. showed that circulating copeptin was a biomarker for prediction of all-cause mortality in patients with heart failure, HR = 3.26 (95% CI: 0.95–11.25) [18]. In our study we found that the copeptin level was 287 pmol/l in mortal cases and similarly the predictive value of copeptin for mortality was 116 pmol/l in EuroSCORE 2.
Regarding the data of 484 patients in the current study one can say that copeptin and NT-proBNP can be utilized as predictive biomarkers for the mortality and prognosis of coronary bypass patients. Our results were also correlated with EuroSCORE II evaluations. The EuroSCORE II contains information on age, gender, angina pectoris, pulmonary hypertension, diabetes, renal failure and previous medical history but no data associated with predictive biomarkers. According to the outcomes of this research, EuroSCORE II might be developed and additional features might be added. We believe that copeptin and NT-proBNP may be included in EuroSCORE as predictive biomarkers. This could also increase the surgery results by focusing the surgeon.
This study was conducted solely on coronary bypass patients. Other cardiac procedures such as valvular surgery and/or aortic surgery cases were not included in the analysis. Further prospective research with a larger sample size and all kinds of cardiac operations is needed to enlighten the clinicians.