
Introduction
Hypertrophic cardiomyopathy, which is usually genetically determined, is a disease of the myocardium characterized by marked hypertrophy of the left ventricle (LV) and occasionally the right ventricle (RV), possible obstruction of the LV outflow tract (LVOT), life-threatening arrhythmia and sudden cardiac death [1]. The European Society of Cardiology (ESC) Guidelines for the diagnosis and management of hypertrophic cardiomyopathy [2] suggest surgical septal myectomy (SM) as the preferred treatment in patients with hypertrophic obstructive cardiomyopathy (HOCM). The success of SM depends on the following factors: clinic and operator experience [3], precise cardiac imaging, an accurate surgical plan and intraoperative monitoring of the results, and is defined by comparison with the target outcome. Identifying these optimal factors is a challenge for centres that perform low numbers of procedures (i.e., low-volume centres) and for surgeons inexperienced in SM. The extent of SM affects the surgical outcomes [4], but its planning is still mainly based on echocardiographic findings. According to the 2014 ESC Guidelines [2], transthoracic echocardiography (TTE) is recommended as initial evaluation for all patients with hypertrophic cardiomyopathy. Cardio-vascular magnetic resonance (CMR) or computed tomography angiography (CTA) is indicated only in those with an inadequate echocardiography window. There are few studies and limited case reports that describe the use of 3-dimensional (3D) cardiac imaging and 3D-printed models of the LV and interventricular septum (IVS) to treat patients with HOCM [5]. 3D models are useful for cardiac imaging [5] and for improving the surgeon’s manual skills in performing SM [6]. We offer a new method of extended SM, namely an optimal 3D-modelled septal myectomy (OSM) [7] to achieve an ‘ideal’ thickness of 10–11 mm at all points of the IVS. We suggest that the OSM should not only reduce the elevated LVOT gradient and systolic anterior motion (SAM) of the mitral valve, but also lead to long-term LV remodelling with an increase in its volumetric dimensional parameters and decreased diastolic dysfunction. It should also accelerate the surgeon’s learning curve.
Aim
To improve results in centres treating few patients with hypertrophic obstructive cardiomyopathy, we propose a new method of optimal septal myectomy using 3-dimensional models to achieve an ‘ideal’ interventricular septum thickness of 10–11 mm at all points.
Material and methods
Thirty consecutive patients admitted to our centre between January 2017 and July 2018 were included in this prospective non-randomized cohort study. Their dominant symptom was shortness of breath. The inclusion criterion was a peak pressure gradient in the area of LV obstruction (basal, mid-ventricular or both) ≥ 40 mm Hg at rest and being refractory to ongoing drug therapy. Exclusion criteria were contraindications to surgery. The patients’ characteristics before surgery are summarized in Table I. Table II presents the preoperative TTE data.
Table I
Baseline clinical characteristics before surgery
Table II
Transthoracic echocardiography data before operation and at the latest follow-up
[i] LV – left ventricle, LVEDD – left ventricle end diastolic diameter, LVEDV – left ventricle end diastolic volume, LVEF – left ventricle ejection fraction, LVESD – left ventricle end systolic diameter, LVESV – left ventricle end systolic volume, LVOT – left ventricle outflow tract, SAM – systolic anterior motion.
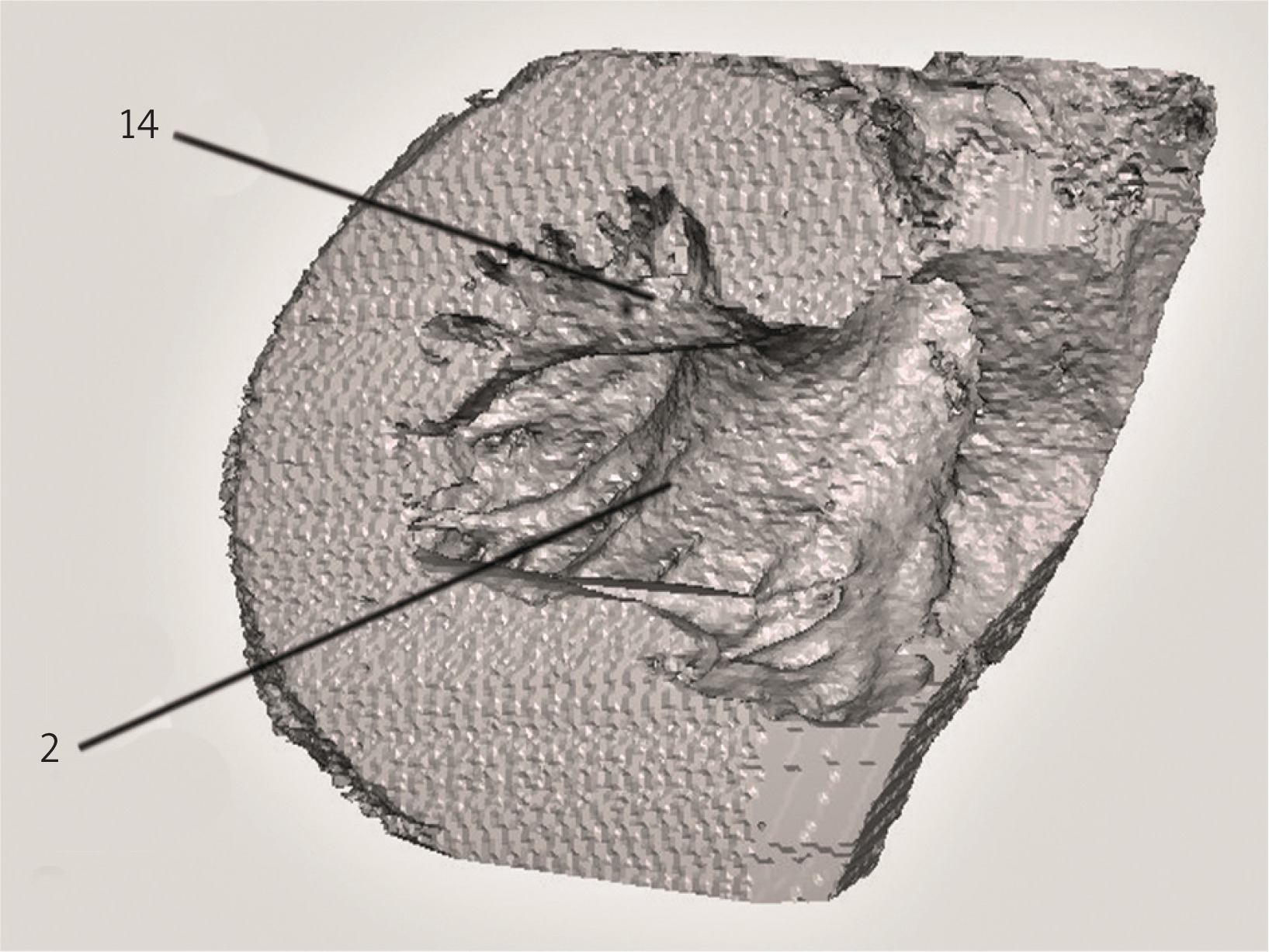
Preoperative patient examinations included TTE, CTA or CMR and coronary angiography. Intraoperatively, transoesophageal echocardiography (TEE) was performed before and after cardio-pulmonary bypass to monitor the results of SM. Using the CTA results (cardiac diastole phase), we created a virtual 3D model of the IVS (scale 1 : 1) using the OsiriX open source DICOM viewer (Fig. 1). We supplemented the anatomical divisions of the IVS by adding three additional surgical zones [7, Suppplementary material] for extended SM to facilitate navigation during mapping and surgery. We distinguished three varieties of abnormal bundles: anterior, from basal segments to anterolateral papillary muscle; posterior, from basal segments to posteromedial papillary muscle, and combinations of these such as ‘swallowtail’ (Fig. 1). Twenty-five (83%) patients had abnormal bundles in their LV. In three of these patients, the bundles were not visualized using TTE and TEE.
Fig. 1
Virtual 3D model of interventricular septum. Anterior bundle (1, indicated with line), posterior bundle (2, indicated with line), swallowtail bundle (1 + 2 lines)
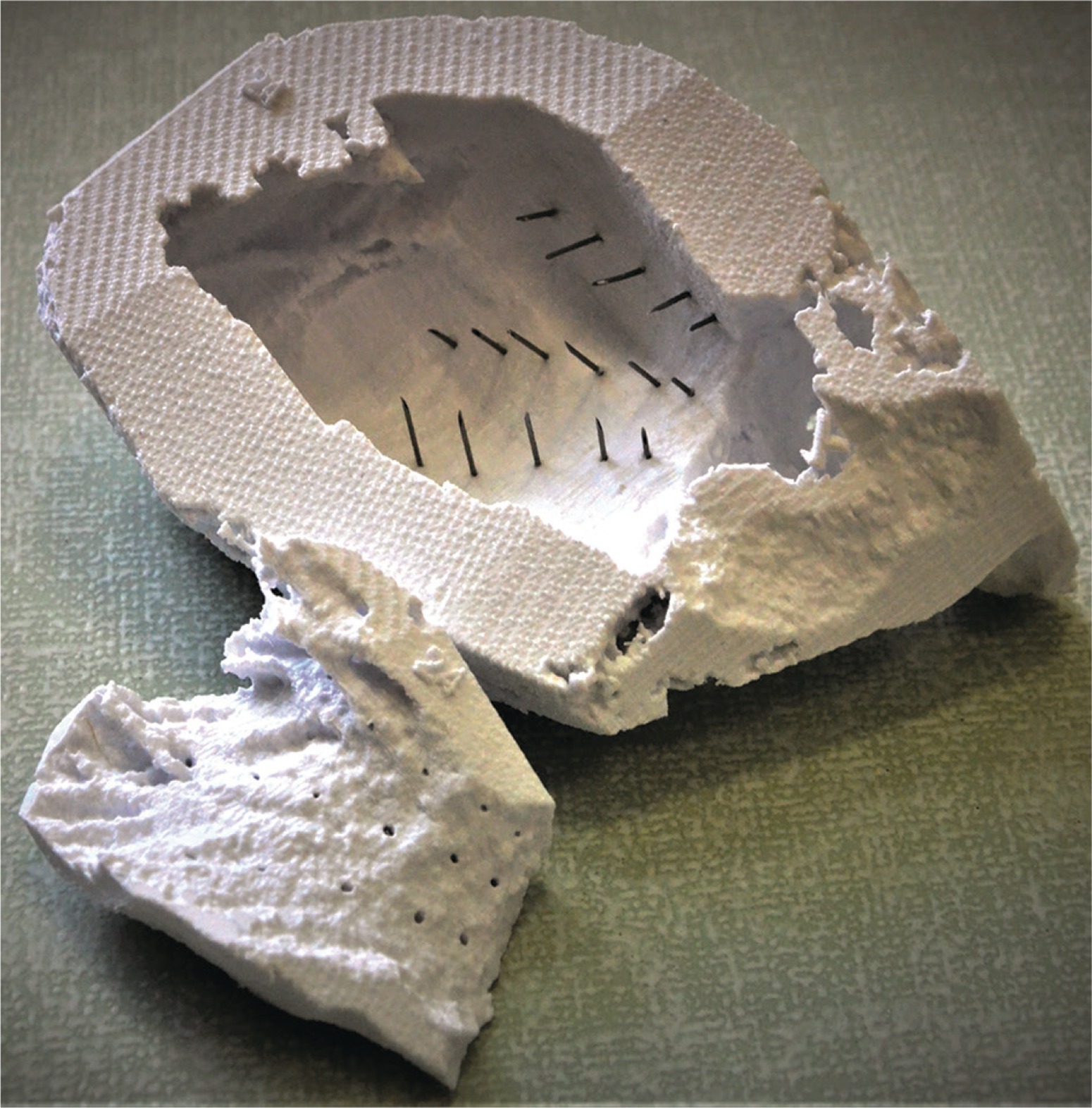
Subsequently, computer-aided mapping of the IVS was performed by cross-sectioning the 3D model in different planes and measuring the IVS thickness at different points. This was followed by performance of a virtual SM to produce an accurate plan of intervention and create an ‘ideal’ IVS. Virtual SM can be performed in several ways, one of which is by flattening an IVS model and then removing the flattened segment from the main model to obtain a fragment representing the tissue to be removed. The next step was 3D printing of a model of the ‘ideal’ IVS and its fragment in polylactide using a low-cost 3D printer (FlashForge Guider 3D printer; FlashForge Corporation, Zhejiang, China) at an average cost of $10 per model (Fig. 2). In the first 2 cases, the fragment was excised mechanically after 3D printing. In 15 more recent cases, we implanted needles into the ‘ideal’ IVS to the height of the fragment to mark accurately the depth of the myocardial excision in each surgical zone (Fig. 2).
Fig. 2
Model of an ‘ideal’ interventricular septum with needles implanted to mark the depth of septal myectomy and the fragment to be resected
The study was approved by the ethics committee of our centre and all participants signed written informed consent.
We took a sterile 3D model to the operating room. SM was performed through an ascending aorta approach from anatomical surgical segment IA to segment IIIA [7, Suppplementary material] and from basal to apical segments. We prefer a ‘layer-by-layer’ excision technique. Extended SM was completed using the in-house designed scalpel and forceps (Fig. 3). In the first 15 cases, the depth of the resection in each surgical zone was determined based on the model mapping data, considering the width of a number 13 blade (6.2 mm) and by successively filling the surgical zones of the trough in the sterilized 3D-printed IVS model with the excised myocardium until the thickness of the excised model fragment was achieved [7]. In 15 recent cases, the excised tissue was sequentially laid out on the bottom of the 3D model until it reached the tips of the needles and then it was weighed (Fig. 4).
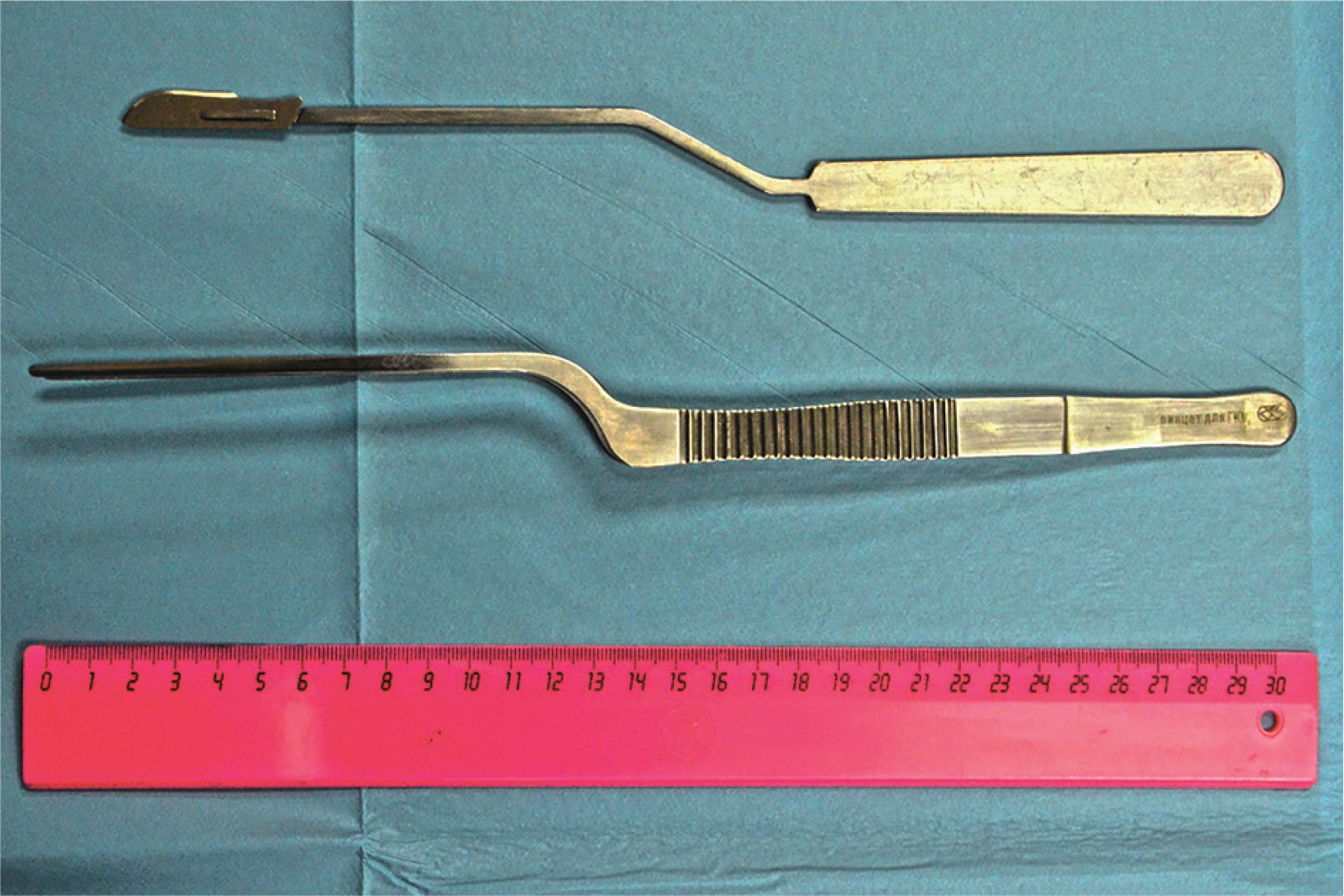
Fig. 4
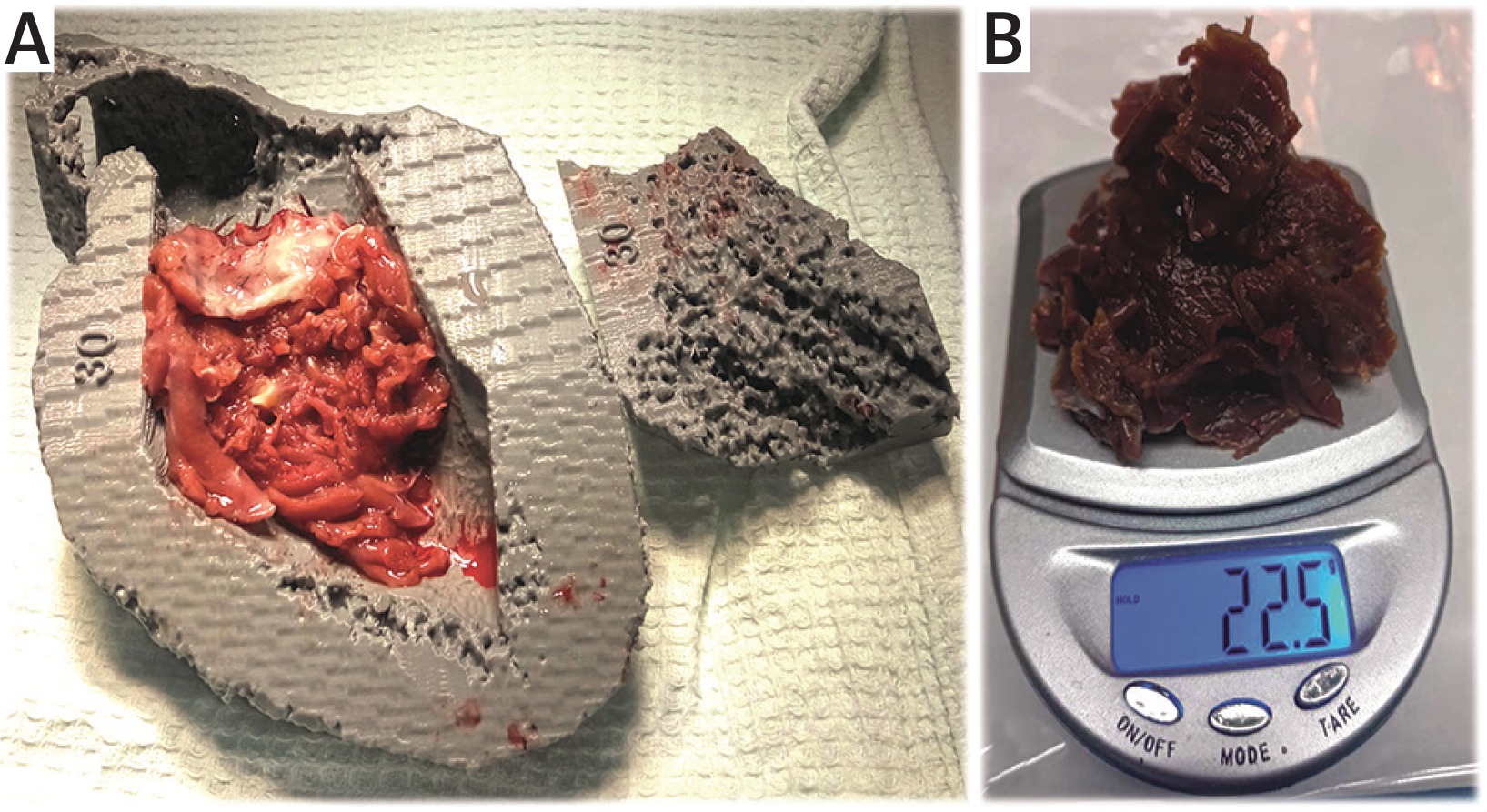
A – Resected fragments of myocardium are sequentially laid out on the bottom of the 3D model until they reach the tips of the needles. B – Weighing the excised myocardium (weight in grams)
Abnormal muscular bundles as well as fibrous–muscular attachments between papillary muscle and IVS or LV free wall, and anomalous chordal attachments between mitral valve leaflets and IVS or LV free wall, were excised. If necessary, longitudinal incision of hypertrophic papillary muscles was also performed.
Mortality and major hospital complications within 30 days after surgery were assessed. Follow-up examinations included symptom assessment, electrocardiography and TTE. These tests were done at discharge and at 3 and 12 months after intervention.
Statistical analysis
Continuous variables with normal distribution as indicated by the Kolmogorov-Smirnov test are reported as mean and standard deviation (mean ± SD). These values were compared using Student’s t-test or a repeated measures t-test. Categorical variables are presented as number and percentage. The Wilcoxon signed-rank test was used to compare repeated measurements. A statistical hypothesis of equal distributions was rejected at p ≤ 0.05. We used SPSS software (v. 19.0; IBM Statistics, Armonk NY, USA) for all statistical analyses.
Results
The main perioperative characteristics of the participants are shown in Table III.
Table III
Main perioperative characteristics (n = 30)
Initial isolated extended SM (n = 29, 97%) was effective in 23 of 29 cases (79%). We encountered no complications when re-clamping was required (6 patients) for mitral valve interventions.
Four non-fatal complications were observed: exacerbation of chronic obstructive pulmonary disease in 1 patient and pacemaker implantation for complete atrioventricular block in 3 patients, two of whom had complete right bundle branch block before surgery. No haemodynamically significant SAM was detected. No patient required mitral valve replacement or had an iatrogenic ventricular septal defect. Six patients required a restart of cardio-pulmonary bypass when TEE monitoring revealed severe mitral regurgitation because of organic valve disease or annulus dilatation. Mitral valve repair was completed in these patients with good outcomes. In one patient, mitral valve annuloplasty was pre-planned and performed simultaneously with OSM because of severe mitral valve annulus dilatation detected on TTE. Blood regurgitation volume (calculated from TTE) in cases of residual moderate (according to the depth of the regurgitant jet into the left atrium) mitral insufficiency (n = 16, 53%) did not exceed a value of 21.0 ml.
The obstruction was completely relieved in all cases, as evidenced by very low (7.5 ±4.4 mm Hg) residual LVOT gradients.
In 2 patients who had extreme HOCM phenotypes with systolic sub-obliteration of the LV cavity, we resected 22.3 and 22.5 g of the myocardium, respectively (Fig. 4 B).
All patients underwent follow-up. The mean follow-up time was 8.8 ±5.5 months (min. 9 days, max. 19 months). Complications were observed in one patient (sternal osteomyelitis). Major TTE data at follow-up are shown in Table II. Haemodynamically significant SAM was abolished in all patients. The mean resting peak LVOT gradient at the latest follow-up was 7.1 ±4.2 mm Hg (min. 3, max. 15). The maximum resting peak LVOT gradient of 15 mm Hg recorded in 1 patient was relieved by concomitant aortic valve replacement with a 21-mm bioprosthesis because of organic aortic valve stenosis. Asymptomatic moderate (2/4) aortic regurgitation was noted in 2 patients.
Both volumetric and dimensional TTE parameters of the LV increased compared with preoperative values (Table II).
All patients are alive and show significant improvement in their quality of life. Their New York Heart Association functional class (FC NYHA) improved significantly compared with preoperative values: 70% of patients (n = 21) were in FC NYHA I and 30% (n = 9) in FC NYHA II, p < 0.001.
Discussion
We are convinced that the completeness of SM is of great importance and the key to surgery. Based on our experience and literature reports [8], inadequate initial SM is associated with poor outcomes. The main reasons for repeated SM in patients initially operated on for HOCM are an insufficient length of the resection towards the LV apex, inadequate depth of SM, and mid-ventricular obstruction [9].
In our clinic over the period of nine years (2007–2016) before we commenced performing OSM, only 35 (34%) of 104 interventions were isolated SM; mitral valve replacement (MVR) and repair made up 41.4% and 23.1%, respectively (a large percentage of MVR in the surgical treatment of HOCM is generally typical of less-experienced clinics [10]). In these patients, the mean weight of the excised myocardium was only 4.7 ±2.9 g, the incidence rate of iatrogenic ventricular septal defect was 7.7% and the early mortality rate was 1.9%. Recurrence of symptoms and LVOT obstruction were observed in 3 patients. The difference between these results and those of the leading clinics offering HOCM surgery [3, 11] was catastrophic.
Such a non-radical approach was mainly because the extent of SM is currently predominantly empirical [12]. Surgeons rely on their own judgement to determine the extent of excision of the myocardium, without clear criteria for the depth, width and length of the resection. We envisage that advances in surgical procedures for HOCM will be associated with the development of new objective cardio-visualisation techniques for planning the shape and volume of the IVS fragment excised during SM and for intraoperative monitoring of SM quality. We believe that 2D TTE should be considered a screening method, rather than the gold standard for examining patients with HOCM. In our experience, the rejection of a preoperative 3D examination (CTA or CMR) of the heart can be a reason for inadequate SM: 2D TTE underestimates IVS thickness by approximately 6.5 mm (23.6 ±4.2 vs. 30.1 ±5.8 mm, p < 0.001; Table I). Cardio-visualisation based on CTA or CMR plays a major role in the accurate planning of radical SM [13]. The need for accurate cardiac imaging, coupled with the aim of performing truly radical SM to achieve the ‘ideal’ IVS thickness (10–11 mm) at all points, led us to develop the virtual SM as a tool to allow optimal planning, not for the purpose of improving our manual skills.
A combination of factors and mechanisms contributes to developing SAM in HOCM [14]. The key to resolving SAM is to perform truly radical SM instead of abolishing the obstruction using numerous plastic mitral valve interventions as suggested by some authors [14, 15–17]. The large variety of types of mitral valve repair in HOCM only demonstrates that there is still no effective universal intervention. Only SM significantly increases the distance between the anterior mitral valve leaflet and the hypertrophied IVS [14]. Therefore, we are convinced that a truly radical SM has an advantage over partial SM combined with resection of fibrotic secondary chordae [15]. The latter can relieve LVOT obstruction at the basal segments and abolish SAM and SAM-related mitral regurgitation. However, such an approach is ineffective in cases of obstruction in the mid and apical segments, and in diffuse and extreme forms of HOCM. Trans-atrial (including minimally invasive) approaches to relieving LVOT obstruction [16–18] also do not appear promising. Their achievement of radicality is doubtful and control of the remaining IVS thickness is complicated. Relief of obstruction by suturing a large auto-pericardial patch at the base of the anterior mitral leaflet [16–19] has a highly questionable long-term prognosis for mitral valve functioning in young and middle-aged patients.
The OSM we propose involves a trans-aortic treatment of obstruction in areas up to apical segments (Fig. 5), which is enabled by the specially shaped scalpel and forceps of our own design and the resection technique we use, i.e., ‘layer-by-layer’ instead of ‘en bloc’ [20]. This technique allows a gradual improvement in visualizing IVS resection zones from basal to apical segments.
Fig. 5
A – Trans-apical section of the 3D interventricular septum model before surgery. B – Trans-apical section of the 3D interventricular septum model of the same patient 3 weeks after ‘optimal’ septal myectomy
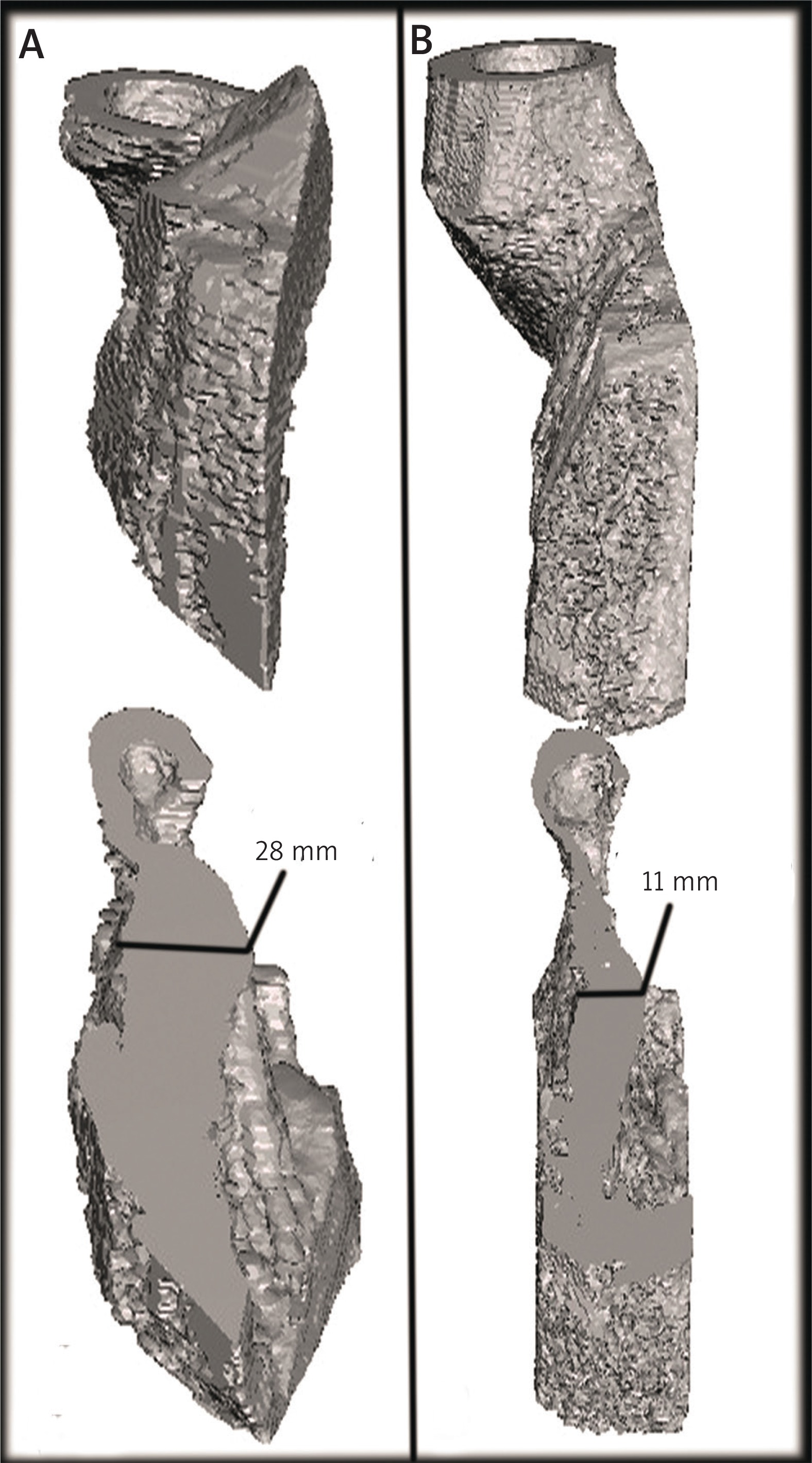
The resection topography remains clear when the fragments are laid out on the 3D-printed model. To our knowledge, the 22.3 and 22.5 g of myocardium that we excised in two of our patients (Fig. 4 B) are the largest excisions described in the literature. The previous largest fragment of 19.9 g was reported by Liu et al. in 2016 [21]. 3D reconstruction of the IVS was done in the first patient before and after the procedure and it proved the IVS thinning from 24–28 mm to 11–12 mm (Fig. 5) [7]. Further postoperative 3D reconstruction of the IVS was not performed because of optimal residual gradients and reliable TTE data on the reduced thickness of the IVS.
The radicality of OSM did not cause an increase in major in-hospital complications. Moreover, as demonstrated by our study findings, OSM resulted in positive remodelling, significantly increased volumetric and dimensional parameters, and a milder degree of diastolic dysfunction as a component of HOCM pathogenesis.
A lack of studies in the field of surgical anatomy in HOCM patients led us to develop our own anatomical–surgical classification for IVS zone resection [7], plus an anatomical–surgical classification of abnormal bundles, both of which facilitate navigation during mapping and surgery.
3D printing of an ‘ideal’ IVS with its excised fragment is also important in the OSM technique. One of the main problems with SM is to determine the resection depth at each point of the IVS and the thickness of the remaining IVS. This is usually done empirically based on the existing surgical plan, bimanual IVS examination [22] and different methods using ultrasonic probes [23]. We consider that none of these methods are both convenient and objective. Using sterile 3D-printed models of an ‘ideal’ IVS with needles implanted up to the excision height and of the IVS fragment to be removed in the operating room is an objective method of monitoring the shape, depth and volume of SM. Intraoperative weighing of the excised fragments of the hypertrophied IVS is an additional monitor of the radicality of SM and should be performed routinely. OSM does not exclude the possibility of preoperative and postoperative manual palpation of the IVS, if desired by the surgeon.
It is obvious that even the most radical SM does not allow relief of mitral regurgitation in cases of organic lesions of the mitral valve. In our practice, we had to restart cardio-pulmonary bypass after OSM and TEE monitoring in six patients to allow mitral valve repair. We are now confident in the paradigm: ‘Do not stitch (initially) and do not patch the mitral valve. Just do it – truly radical septal myectomy!’ This method always abolishes SAM-related mitral regurgitation. In cases where mitral regurgitation remains significant owing to an organic lesion of the mitral valve, the valve can be remodelled after restarting cardio-pulmonary bypass. In our experience, moderate residual mitral regurgitation (according to the depth of the regurgitant jet into the left atrium) after initial isolated SM is asymptomatic in patients with HOCM and has no greater impact on exercise tolerance and quality of life in the long-term postoperative period than mild residual mitral regurgitation (1/4).
The pacemaker implantation rate for complete atrio-ventricular block after OSM does not exceed that presented in the world’s largest SM registries [24, 25], but the risk of pacemaker implantation is obviously higher in patients with initial complete right bundle branch block.
Our study has some limitations, the most important of which is the small number of patients. Further patient enrolment is required to compare the results of OSM with those of other surgical treatment options for HOCM.
Conclusions
Computed tomography angiography (CMR) with 3D reconstruction is an optimal method for cardio-visualisation of the IVS. Virtual SM is an excellent planning method for a radical 3D-modelled SM. The proposed optimal 3D-modelled SM allows intraoperative monitoring of the shape and volume of the myocardium resection to achieve the ‘ideal’ IVS and true radicality. It eliminates obstruction in the LV and SAM, resulting in LV remodelling with an increase in LV end-diastolic volume and diameter at early follow-up. In addition, this method speeds up the learning curve for surgeons inexperienced in SM.









