





Pulmonary aspiration of gastric contents is mainly due to regurgitation or vomiting that may occur during laryngoscopy or tracheal extubation, or during ventilation via a laryngeal mask airway, or in sedated patients [1, 2]. Increased gastric content volume is one of the conditions required for aspiration to occur; it is also a determining factor of the severity of pulmonary injury related to aspiration [3]. Thus, results of previous animal studies have suggested that aspiration of acidic fluid volume ≥ 0.8 mL kg-1 may result in severe lung injury in humans [3].
The relationship between gastric fluid volume and pulmonary aspiration may be divided into two steps: a first step corresponding to the occurrence of regurgitation or of vomiting, and a second step corresponding to the relationship between regurgitated (or vomited) volume and aspirated volume of fluid. The first step is multifactorial as it depends on the decrease in the lower oesophageal sphincter pressure due to general anaesthesia and/or on the increase in intragastric pressure due to a full stomach or to anaesthetic factors such as insufficient depth of anaesthesia or insufflation of air into the stomach [4–6]. The second step is mostly dependent on anatomical and on head and body position factors [7–9]. In a recent study using a life-like manikin, we found that the minimal value of the volume of liquid regurgitated that may lead to pulmonary aspiration of fluid volume ≥ 0.8 mL kg-1 was around 1 mL kg-1 when the head was in the sniffing position, and around 1.8 mL kg-1when the head was in the extension position [10]. Nevertheless, the use of a manikin as a model of pulmonary aspiration raised some issues regarding the generalizability of the results due to important differences compared to humans with respect to the compliance of the tissues.
We therefore performed a study that aimed to compare the aspirated volume of regurgitated water in fresh human cadavers with the head set in the sniffing position and in the extension position. The second aim of this study was to determine the critical volume of liquid regurgitated or vomi-ted that led to pulmonary aspiration of fluid volume ≥ 0.8 mL kg-1 and ≥ 1.5 mL kg-1 for each head position.
METHODS
Study protocol
Human cadavers were provided by the Department of Anatomy of the Claude Bernard Lyon 1 University, Lyon, France. The cadavers used in research studies and for teaching purposes are donated to the Lyon 1 University Department of Anatomy according to a body donation procedure headed by Pr Patrick Mertens who has been empowered and commissioned to give approval for all studies using cadavers. Hence, separate ethical committee approval and formal consent were not required.
Adult human cadavers were included in this study. Seven fresh human cadavers were used, 48 h to 72 h after their death. They were stored at 6°C in the interim and were warmed to 22°C three hours before the start of the study protocol. Inclusion criteria were body mass between 45 and 90 kg, height 150 to 180 cm, body mass index < 30 kg m-2. Exclusion criteria were any previous history of gastrooesophageal surgery or of tracheal lesions or tumour, known disease of the pharynx, larynx, oesophagus, stomach, as well as previous history of radiation to the head, neck, chest, oesophagus, or stomach.
After a surgical thoracoabdominal incision was performed, a 2-way Foley urinary catheter was inserted into the lower extremity of the oesophagus, with the tip set immediately above the lower oesophageal sphincter. A surgical approach of the trachea was done at the anterior side of the neck, approximately 10 cm from the larynx. The cranial part of the trachea was connected to a bottle using surgical watertight catheterization to collect aspirated water.
The cadaver was placed in the supine position on a non-tilted table. The head was either extended and placed on a pillow 6 cm in height (sniffing position) or extended without a pillow (extension position).
For each head position, the following volumes of water were injected into the urinary catheter connected to the oesophagus: 40, 80, 100, 120, 150 and 200 mL. Syringes of 60 mL with a conical tip (Penta-ferte, Campli, Italy) were used by an investigator (NS) to manually inject water at a flow rate of 20 mL per second, on two occasions for each volume and for each head position. The order of volumes injected was randomized using a computer-generated list.
The volume of water that was collected in the bottle connected to the trachea was measured and recorded by a second investigator (EC), who was blinded to the volume injected.
After each injection, the residual volume of water was aspirated so that the stagnant water was completely evacuated from the oral cavity, pharynx and oesophagus.
Statistical analysis
Collected volumes were expressed as median and interquartile range, and were compared using the Mann-Whitney U test and Wilcoxon signed rank test, as appropriate. The correlations between injected volume and collected volume were analysed using linear regression, with calculation of the corresponding Pearson correlation coefficient, for each head position. The Benjamini-Hochberg step-up procedure was applied for multiple hypothesis testing correction [11]. The cut-off values of the volumes of water injected into the oesophagus leading to aspirated volume ≥ 1.5 mL kg-1 and ≥ 0.8 mL kg-1 were determined by plotting receiver operating characteristic (ROC) curves with calculation of the areas under the curve. All analyses were performed using MedCalc version 12.1.4.0 for Windows (MedCalc Software, Ostend, Belgium) using a 2-sided type 1 error of 0.05 as the threshold for statistical significance.
When assuming that the mean aspirated volume would be 75 ± 25 mL in the sniffing position [10], the inclusion of seven fresh human cadavers was required to show a difference of 50 mL between the positions, with a significance level of 0.05 and a power of 0.95.
RESULTS
Of the seven cadavers studied, five were women; the median (interquartile range) body mass was 59 (54–78) kg, height was 157 (154–172) cm, and body mass index was 24 (23–26) kg m-2.
The median aspirated volume was 106 (80–150) mL in the sniffing position and 89 (68–128) mL in the extension position (P = 0.038), corresponding to 99 (97–100)% and 86 (78–93)% of the injected volume that was aspirated into the trachea in the sniffing position and in the extension position (P < 0.0001), respectively. The median difference between injected and collected volume of water was 2 (0–5) mL in the sniffing position, and 15 (5–23) mL in the extension position (P < 0.0001). Collected volumes according to injected volumes in the sniffing and the extension positions are presented in Table 1. For each volume injected, the median aspirated volume of water was significantly increased in the sniffing position vs. the extension position.
TABLE 1
Aspirated volume of water for each injected volume, according to the head position of the cadaver
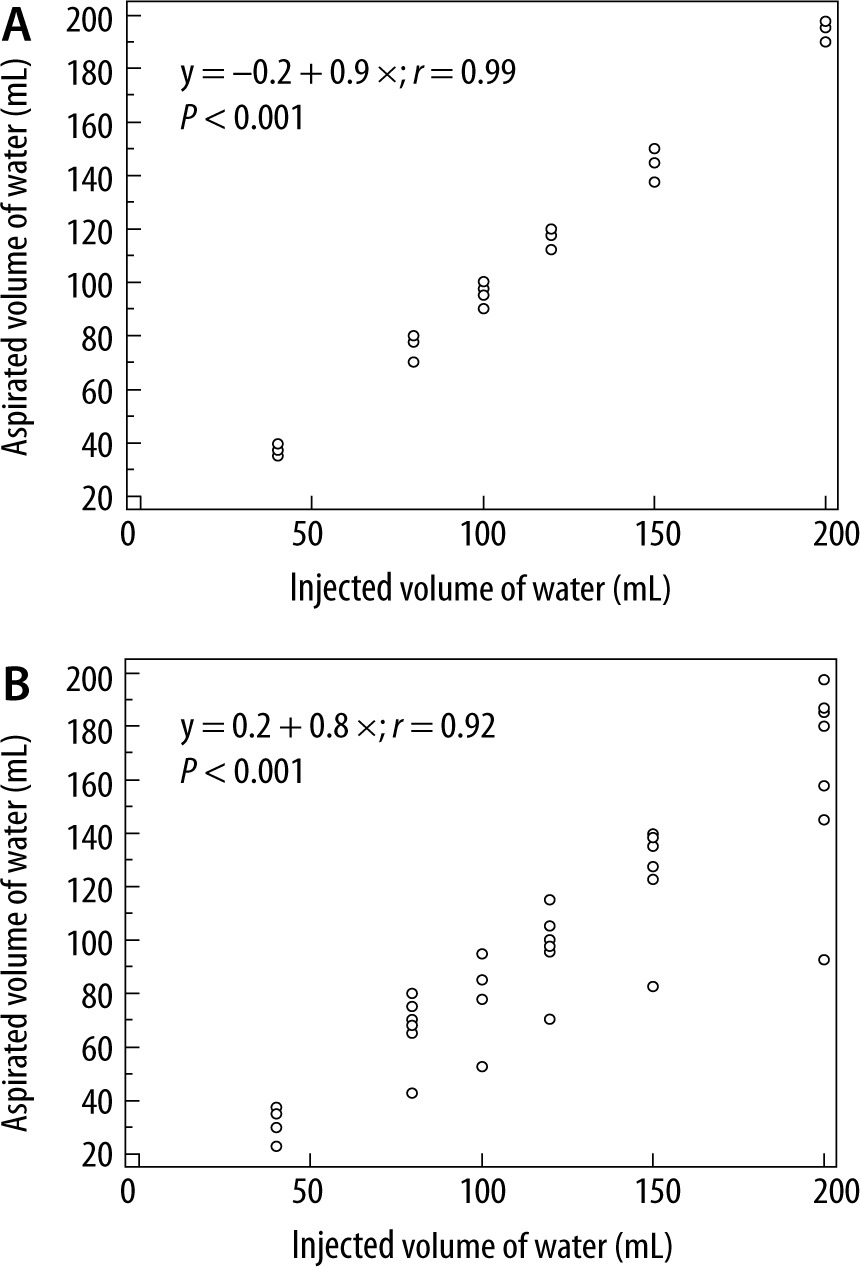
The correlation between injected and collected volume of water was high in both positions: r2 = 0.99 (P < 0.001) in the sniffing position and r2 = 0.84 (P < 0.001) in the extension position (Figure 1).
FIGURE 1
Correlation between the injected and the aspirated volume of water when the head is in the sniffing position (A) and in the extension position (B)
The cut-off volume of water injected into the oeso-phagus leading to aspirated volume ≥ 0.8 mL kg-1 was 0.8 mL kg-1 in the sniffing position and 1.2 mL kg-1 in the extension position. The area under the ROC curve was 0.99 (95% CI: 0.92–1) in the sniffing position and 0.98 (95% CI: 0.91–1) in the extension position. Aspirated volume was ≥ 0.8 mL kg-1 in the sniffing position when the injected volume was ≥ 0.8 mL kg-1 in 35/35 (100%) of cases, and it was < 0.8 mL kg-1 when the injected volume was < 0.8 mL kg-1 in 7/7 (100%) cases. In the extension position, aspirated volume was ≥ 0.8 mL kg-1 when the injected volume was ≥ 1.2 mL kg-1 in 32/32 (100%) cases, while it was < 0.8 mL kg-1 when the injected volume was < 1.2 mL kg-1 in 9/10 (90%) cases.
The cut-off volume of water injected into the oesophagus leading to aspirated volume ≥ 1.5 mL kg-1 was 1.5 mL kg-1 in the sniffing position and 1.8 mL kg-1 in the extension position. The area under the ROC curve was 0.99 (95% CI: 0.90–1) in the sniffing position and 0.98 (95% CI: 0.88–1) in the extension position. Aspirated volume was ≥ 1.5 mL kg-1 in the sniffing position when the injected volume was ≥ 1.5 mL kg-1 in 25/26 (96%) cases, while it was < 1.5 mL kg-1 when the injected volume was < 1.5 mL kg-1 in 16/16 (100%) cases. In the extension position, aspirated volume was ≥ 1.5 mL kg-1 when the injected volume was ≥ 1.8 mL kg-1 in 19/20 (95%) cases, while it was < 1.5 mL kg-1 when the injected volume was < 1.8 mL kg-1 in 22/22 (100%) cases.
DISCUSSION
The results of this study suggest that most of the regurgitated clear fluid may be aspirated into the trachea when no respiratory protection reflexes are effective in the human, as in the case of gene-ral anaesthesia or deep sedation. In particular, the sniffing position was associated with significantly greater volume of aspirated water than the extension position.
These results corroborate those of a previous study performed on a life-like manikin that reported a high correlation between injected and collected volume of water, with a larger collected volume when the head of the manikin was in the sniffing position vs the extension position [10]. However, the proportion of water passing into the trachea was somewhat increased in the cadaver model compared to the manikin model previously used, since more than 85% of injected water entered the trachea in the human cadavers, while the rate of collected water ranged from 0 to 90% of injected water in the manikin [10]. This discrepancy between the two models may be related to some differences in the elasticity of the tissues, even if anatomical features of life-like manikins are similar to those of humans. In particular, the human oesophagus is flat in the basal state, with collapsed walls and no lumen, while the manikin oesophagus was represented by a somewhat rigid open tube, which is likely to have affected the flow of injected water into the oeso-phagus and the reliability of the manikin model. Conversely, a fresh human cadaver has been considered in several previous studies as a particularly appropriate model for research and for training in airway management [12–14], since it reproduces similar conditions to those observed in paralyzed patients for airway management [12]. In addition, a fresh human cadaver model has been previously used to assess the seal of supraglottic airway devices during elevated oesophageal pressure [15]. The results of our study confirm that a fresh human cadaver model could be useful as an experimental model of pulmonary aspiration.
Little is known as regards the relationship between gastric fluid content volume and aspiration pneumonia. This question has become more relevant this last decade with the development of point-of-care gastric ultrasound for the preoperative assessment of the type and the volume of gastric fluid content [16, 17]. This tool allows the detection of thick fluid and solid contents corresponding to “high risk stomach” regardless of their volume [18]; it also allows the calculation of the volume of clear fluid content [19]. If the results of studies performed in animals have suggested that 0.8 mL kg–1 of acidic fluid should pass into the lungs to lead to severe pulmonary aspiration in humans [3, 20], the critical gastric contents volume leading to regurgitation or vomiting, and, ultimately, to pulmonary aspiration of a sufficient volume of fluids, remains unknown. Some authors have recommended the use of a 1.5 mL kg–1 cut-off value to define a full stomach when performing ultrasound assessment of gastric fluid volume [18, 21], arguing that the prevalence of pulmonary aspiration is low and that gastric volume ≥ 1.5 mL kg–1 is rarely measured in fasting volunteers and elective patients [22–27]. This assumption remains however speculative. In fact, the occurrence of pulmonary aspiration of gastric contents also depends on several other factors, including patient and head positioning as illustrated herein, as well as on the quality of anaesthetic management and on whether gastric contents was passively regurgitated or actively vomited [2, 28]. In the present study, we found only a small difference between injected and collected volume of water in both head positions, illustrating that, should regurgitation or vomiting occur, the volume that would pass through the lower oesophageal sphincter would almost fully pass the larynx and enter the trachea in an anaesthetized human without effective upper airway reflexes. Hence, our results suggest that a gastric fluid volume ≥ 0.8 mL kg-1 or ≥ 1.2 mL kg-1, according to the position of the head, may potentially lead to significant pulmonary aspiration in case of regurgitation or vomiting in an anaesthetised patient.
The sniffing and the extension positions both ensure good glottic visualization under direct laryngoscopy, though the sniffing position may provide better visualization in the obese and in head extension-limited patients [29, 30], and is considered as the best position for direct laryngoscopy according to the Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults [31]. In fact, the sniffing position ensures greater occipito-atlanto-axial extension compared to simple head extension [30], while, however, also increasing the mouth-arytenoid and the mouth-carina angles, hence favouring the flow back of regurgitated water towards the trachea [8]. The results herein suggest that the ultrasound calculation of gastric fluid volume ≥ 0.8 mL kg-1 could lead the anaesthetist to consider the risk of pulmonary aspiration and/or to decide to place the patient’s head in the extension position in first intention to reduce the risk of aspiration. For example, for a man weighing 80 kg with ultrasound calculated gastric fluid volume of 85 mL corresponding to a volume per weight of 1.05 mL kg-1, the risk of aspiration of fluid volume ≥ 0.8 mL kg-1 could probably be considered when positioning the head in the sniffing position. Conversely, for this patient, the risk of pulmonary aspiration of a volume ≥ 0.8 mL kg-1 probably remains low when positioning the head in the extension position.
The study has some limitations. First, the results apply only to clear fluids that passed through the lower oesophageal sphincter at a flow rate of 20 mL per second, which corresponds to a rather mild flow rate, of 1200 mL min-1. Any change in flow rate or in fluid viscosity might lead to a substantial change in the rate of water entering the trachea. Furthermore, regurgitation or vomiting of solid food particles may lead to immediate acute asphyxia, a complication that could not be assessed in the present study. Second, though non-embalmed human cadavers were used, there may have been some degree of rigidity affecting thoracic and pharyngeal compliance, which is likely to have affected the results of the study. However, the use of a fresh human cadaver remains of interest, as it provides anatomical and morphological conditions similar to those observed in an anaesthetized patient [12]. Besides, experimental studies assessing the regurgitation and the aspiration of gastric content volume are not feasible in the living human. Finally, the results of this study apply to cadavers placed on a non-tilted table, while it has been reported that head-down tilt was associated with decreased aspirated volume [8]. In particular, a 35° head-down tilt could fully prevent the occurrence of pulmonary aspiration when the head is set in the extension position [8], while, however, increasing the difficulty in visualizing the vocal cords and prolonging the time taken to intubate [9].
To conclude, the results of this study performed on fresh human cadavers confirm previous data showing that most of the regurgitated clear fluid volume enters the trachea in humans lying in the supine position on a non-tilted table, especially when the head is in the sniffing position. These results contribute to better understanding as regards the relationship between the volume of clear fluid regurgitated and the volume of clear fluid aspirated into the trachea in a paralyzed human. In particular, the determination of the cut-off value of the volume of liquid regurgitated leading to pulmonary aspiration of fluid volume ≥ 0.8 mL kg-1 could help clarify the interpretation of the ultrasound calculation of gastric fluid volume for the preoperative assessment of the risk of pulmonary aspiration.