
Introduction
Hepatic encephalopathy (HE) is a complex neuropsychiatric syndrome arising in patients with chronic liver disease, particularly those with advanced cirrhosis. It manifests as a wide range of cognitive, behavioural, emotional, and motor disturbances, ultimately impairing the patient’s quality of life and daily functioning [1]. HE is considered a poor prognostic marker in cirrhotic patients and is associated with increased morbidity, mortality, and healthcare burden. Clinically, HE is classified into overt HE (OHE) and minimal HE (MHE) based on the severity of symptoms. OHE presents with visible cognitive and neuromuscular impairments and is graded I to IV according to the West Haven Criteria [2]. In contrast, MHE is subclinical and requires specialised psychometric or neurophysiological testing for diagnosis [3]. Due to diagnostic overlap and the subtlety of presentation, MHE and grade I HE are often grouped under the term covert HE (CHF) for practical clinical evaluation [4].
The pathophysiology of HE is multifactorial. Although not fully understood, hyperammonaemia is a key contributing factor, along with impaired neurotransmission characterised by an excitatory-inhibitory imbalance, oxidative stress, neuroinflammation, and the presence of so-called “false neurotransmitters” that affect cerebral function [5]. Current standard treatments aim to reduce systemic ammonia levels, primarily using non-absorbable disaccharides such as lactulose and lactitol, which promote nitrogen excretion and acidify colonic contents [6]. Other therapeutic agents include rifaximin, a non-absorbable antibiotic that targets gut flora responsible for ammonia production [7], and branched-chain amino acids (BCAAs), which may support muscle-based ammonia detoxification [8]. However, despite these approaches, up to 20–30% of patients continue to experience persistent or recurrent HE episodes [9, 10]. One promising but underused therapeutic approach is zinc supplementation. Zinc plays a vital role in ammonia metabolism, particularly through its involvement in urea cycle enzymes such as ornithine transcarbamylase and glutamine synthetase [10, 11]. Zinc deficiency is frequently observed in cirrhotic patients due to factors such as reduced dietary intake, impaired intestinal absorption, and increased urinary excretion [11–13]. This deficiency may exacerbate ammonia accumulation and impair neurological function. Small-scale clinical studies suggest that zinc supplementation can improve cognitive function and reduce HE severity [14, 15].
Minimal HE is a frequent yet underrecognized complication of liver cirrhosis, characterised by subtle cognitive impairments that can significantly affect patients’ quality of life, daily functioning, and risk of progression to OHE [16]. Although lactulose remains the cornerstone of treatment, a considerable number of patients show suboptimal or delayed cognitive recovery, indicating a need for improved therapeutic strategies [17]. Zinc plays a critical role in ammonia metabolism through its involvement in urea cycle enzymes. It is commonly deficient in patients with cirrhosis due to impaired intake, absorption, and increased urinary loss [16, 17]. This deficiency may exacerbate hyperammonaemia and contribute to the pathogenesis of MHE. Prior studies have suggested that zinc supplementation can enhance ammonia detoxification and support neurocognitive recovery; however, robust clinical evidence, particularly in comparison with standard monotherapy, remains limited and inconclusive [18]. Our study aims to fill this gap by assessing whether adding oral zinc supplementation to lactulose results in a greater improvement in cognitive function and serum ammonia levels compared to lactulose alone. Using validated psychometric testing (PHES) and serum monitoring over 12 weeks, we seek evidence supporting zinc’s adjunctive role in managing MHE and refining treatment strategies.
Material and methods
This prospective cohort study was conducted after approval of the study synopsis by the Ethical Review Committee. Written informed consent was obtained from all participants and their attendants after a detailed explanation of the study’s purpose, potential benefits, and possible side effects. The sample size was calculated to detect a difference in the recurrence of HE between zinc-lactulose combination therapy and lactulose monotherapy (expected proportions: 15.7% vs. 36.3%), with 80% power and a 5% significance level, accounting for a 10% attrition rate. A total of 148 patients (74 per group) were required [18].
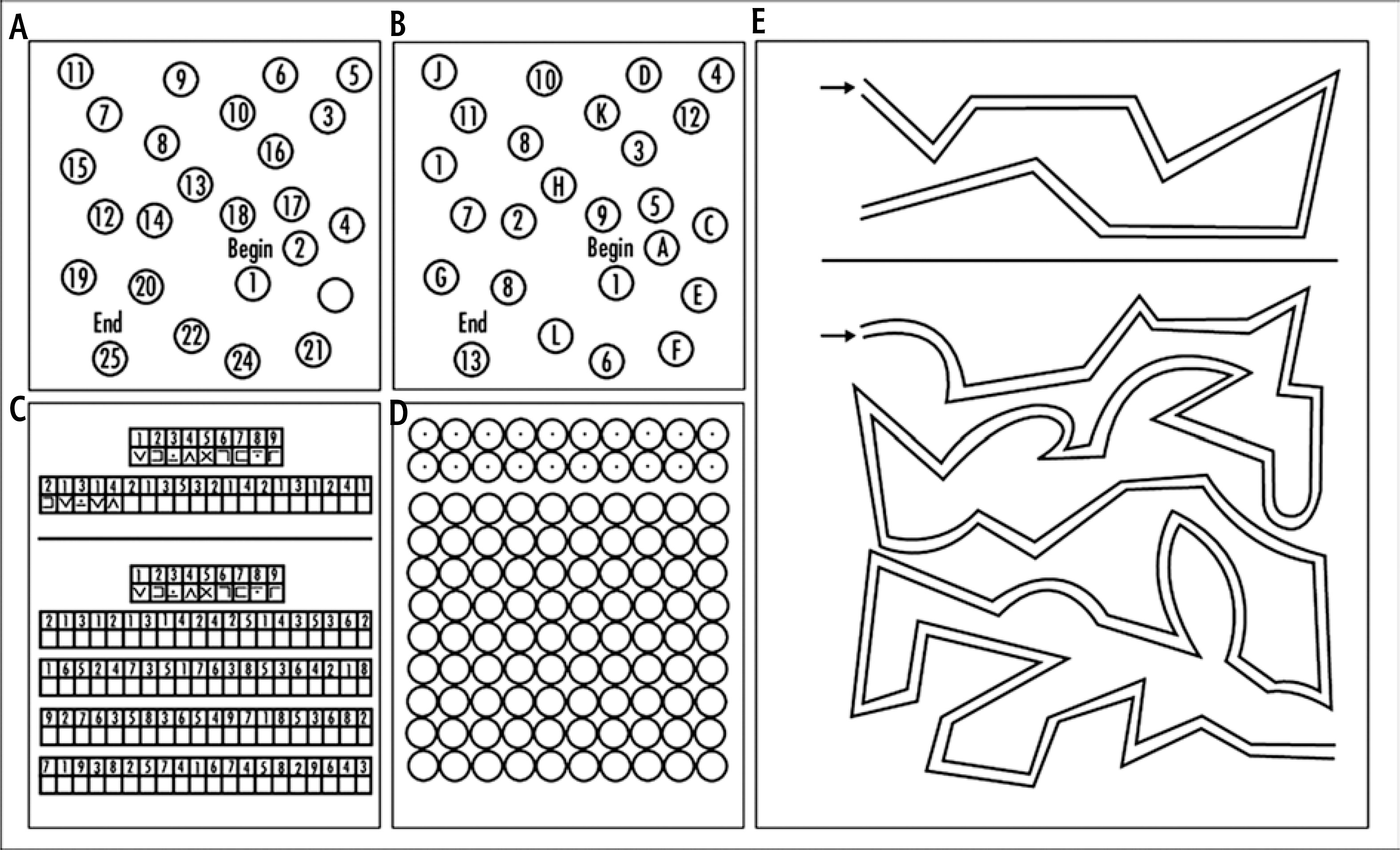
Patients aged 18-60 years with diagnosed liver cirrhosis were included based on predefined inclusion and exclusion criteria. Demographic and clinical information was collected, including age, gender, smoking status (> 5 pack-years), presence of diabetes, hypertension, hepatitis B or C status, and duration since cirrhosis diagnosis. Each patient underwent a thorough clinical examination. Blood samples were drawn and analysed for serum electrolytes, as well as renal and liver function tests, to ensure eligibility. Baseline serum albumin, serum ammonia and serum zinc levels were measured. To eliminate the presence of OHE, a screening test using the MMSE, a validated and structured instrument to evaluate cognitive function, was performed in all patients at baseline. The MMSE assesses the domains of orientation, attention, memory, language, and visuospatial functions, and ranges between 0 and 30. Patients scoring above 24 were considered cognitively intact and eligible to proceed with further study assessments. These patients were subsequently assessed with the Psychometric Hepatic Encephalopathy Score (PHES), including five standardised subtests – Number Connection Test-A (NCT-A), Number Connection Test-B (NCT-B), Serial Dotting Test (SDT), Line Tracing Test (LTT), and Digit Symbol Test (DST) – to detect MHE (Fig. 1). Testing was conducted in a distraction-free room, one-on-one, with timing (in seconds) and scoring (points or errors) recorded as per standard protocol. Final PHES scores ranged from –15 to +5, with scores < –4 indicating MHE. A shorter test completion time was associated with better performance [19].
Patients diagnosed with MHE were divided into two groups (n = 74 per group). Group A received oral zinc sulfate syrup (20 mg of elemental zinc per tablespoon, twice daily) along with lactulose (15-30 ml, twice daily, titrated to produce 2-3 soft stools per day). Group B received lactulose alone at the exact dosage. Follow-up visits were scheduled at week 2 to monitor side effects, such as nausea, vomiting, diarrhoea, or a metallic taste. They were conducted monthly thereafter to assess compliance and any intercurrent illnesses. Patients unable to attend in person were followed via video calls. Serum ammonia and albumin levels, as well as PHES scores, were reassessed at 12 weeks. The time to cognitive improvement was recorded based on noticeable changes in PHES scores.
The primary outcome was the improvement in cognitive function assessed by change in PHES score from baseline to 12 weeks. Secondary outcomes included changes in serum albumin levels, serum ammonia levels, and time to noticeable cognitive improvement. All data were recorded on a pre-designed proforma.
Statistical analysis
All data were entered and analysed using IBM SPSS Statistics for Windows, Version 26.0. Quantitative variables, including age, duration of cirrhosis, pre- and post-treatment serum albumin and serum ammonia levels, as well as individual psychometric test scores (NCT-A, NCT-B, SDT, LTT, and DST), were expressed as mean ± standard deviation (SD). Qualitative variables such as gender, smoking status, presence of diabetes, hypertension, and hepatitis B or C infection were summarised using frequencies and percentages. To assess within-group changes in MHE and PHES scores, serum albumin levels, and serum ammonia levels before and after treatment, a paired sample t-test was applied. An independent samples t-test was used to compare the mean difference in outcomes (PHES scores, serum albumin, and serum ammonia levels) between the two treatment groups. After stratification, outcomes were compared using the appropriate tests of significance, depending on the type of data. A p-value ≤ 0.05 was considered statistically significant.
Results
At baseline, both treatment groups were comparable in terms of demographic and clinical characteristics. The mean age of patients in the lactulose-alone group was 39.7 ±5.67 years, while in the zinc plus lactulose group was 41.2 ±6.43 years (Table 1). The majority of participants in each group were male, with 81.1% in the lactulose group and 78.4% in the zinc group. Smoking was more common in the zinc group (39.2%) than in the lactulose group (29.7%). The prevalence of diabetes was similar across groups (52.7% in the lactulose group vs. 56.8% in the zinc group), while hypertension was more frequent in the zinc group (66.2% vs. 47.3%), hepatitis B infection was higher in the zinc group (50% vs. 24.3%), and hepatitis C prevalence was nearly equal (52.7% vs. 51.4%) (Table 1).
Table 1
Baseline characteristics by treatment group (n = 148)
Following 12 weeks of treatment, both groups demonstrated statistically significant improvements across all components of the PHES. In the lactulose-alone group, there was a substantial reduction in task completion times for NCT-A (p = 0.000), NCT-B (p = 0.000), SDT (p = 0.000), and LTT (p = 0.000), indicating improved psychomotor speed and attention. Similarly, DST scores increased significantly (p = 0.000), reflecting enhanced cognitive processing and memory (Table 2). PHES scores improved from –5.08 ±0.81 to –0.03 ±2.44 (p = 0.000), showing reversal of MHE in many patients. In the zinc plus lactulose group, a comparable pattern was observed. Task completion times for NCT-A (p = 0.000), SDT (p = 0.000), and LTT (p = 0.000) showed significant reductions, while DST scores increased markedly (p = 0.000). The PHES score improved significantly from –5.12 ±0.84 to 0.43 ±2.52 (p = 0.000), with a more pronounced mean increase than in the lactulose-only group. Although both treatments were effective in improving cognitive performance in cirrhotic patients with MHE, the combination of zinc and lactulose demonstrated a slightly greater numerical improvement, particularly in PHES and DST scores, suggesting a potential added benefit of zinc supplementation (Table 2).
Table 2
Pre- and post-treatment neuropsychometric test results and PHES
After 12 weeks of treatment, both groups demonstrated overall clinical and cognitive improvement; however, most differences between the groups were statistically nonsignificant. Mean serum albumin levels were comparable between the lactulose-alone group (3.29 ±0.23 g/dl) and the zinc plus lactulose group (3.26 ±0.28 g/dl; p = 0.454) (Tables 2, 3). Serum ammonia levels decreased more in the combination therapy group (58.84 ±9.23 µmol/l) than in the lactulose group (61.41 ±9.86 µmol/l), though the difference did not reach statistical significance (p = 0.104) (Table 3). Psychometric performance improved in both groups. The mean PHES score improved to –0.03 ±2.44 in the lactulose-alone group and 0.43 ±2.52 in the zinc group, showing better overall cognitive function in the combination therapy group. However, the difference was not statistically significant (p = 0.262). Notably, the time to noticeable cognitive improvement was significantly shorter in the zinc plus lactulose group (6.05 ±0.81 weeks) compared to lactulose alone (6.61 ±1.45 weeks; p = 0.005), indicating that combination therapy may accelerate recovery from MHE (Table 3).
Table 3
Comparison of clinical and psychometric outcomes after 12 weeks of treatment
Discussion
This study assessed the comparative efficacy of zinc plus lactulose therapy versus lactulose monotherapy in improving cognitive function and lowering serum ammonia levels among cirrhotic patients with MHE. The findings affirm that both treatment approaches significantly improved neuropsychometric performance over 12 weeks; however, the addition of zinc resulted in a slightly greater improvement in PHES and a notably shorter time to cognitive recovery. The improvement in PHES components, particularly in attention, processing speed, and memory, reflects the reversibility of MHE with early and effective treatment. This aligns with previous literature suggesting that cognitive impairment in MHE is potentially reversible and responds well to targeted interventions [20, 21]. While lactulose remains a cornerstone therapy due to its ability to lower ammonia via cathartic and prebiotic effects, its combination with zinc may offer added benefits through complementary mechanisms [22].
Zinc’s role in ammonia detoxification is well established. It serves as a cofactor for key enzymes in the urea cycle and glutamine synthesis pathways, aiding in the clearance of ammonia from systemic circulation [23]. Zinc deficiency, common in cirrhotic patients due to poor intake, malabsorption, and increased urinary loss, has been implicated in worsening HE symptoms [24]. In our cohort, zinc supplementation may have addressed this deficiency, enhancing the metabolic capacity to process nitrogenous waste and contributing to the observed improvement in cognitive parameters. Interestingly, while serum ammonia levels decreased more in the zinc group, the between-group difference did not reach statistical significance. This is consistent with earlier meta-analyses, which demonstrated cognitive improvements with zinc supplementation but reported minimal effects on ammonia levels [25]. Jurado Garcia et al. observed that while zinc improved number connection test (NCT) scores, it did not significantly alter HE recurrence rates or serum ammonia concentrations [25]. These findings suggest that the clinical benefits of zinc may extend beyond direct ammonia reduction, possibly involving the mitigation of oxidative stress or the modulation of neurotransmitter function. Supporting this, Tuerk and Fazel described zinc’s neuroprotective role through attenuation of RNA oxidation and astrocytic swelling in hyperammonaemia states [26]. Furthermore, Chavez-Tapia et al. emphasised the importance of nutritional optimisation, including trace element supplementation, as a foundational component in managing HE [27]. Thus, zinc’s benefits may stem from its broader metabolic and neurobiological influence rather than a narrow ammonia-lowering effect alone.
In the present study, the most notable distinction between the two groups was the shorter time to cognitive improvement observed in patients receiving combination therapy. This outcome is clinically meaningful, as even mild cognitive dysfunction in MHE can impair driving ability, medication adherence, and quality of life [28]. Accelerated recovery not only improves patient well-being but may also reduce caregiver burden and healthcare utilisation. Our findings are supported by earlier controlled trials, such as that of Shaposhnikova et al., which demonstrated an improved clinical response to HE treatment in zinc-deficient cirrhotic patients after zinc supplementation [29]. Similarly, Chetri and Choudhuri emphasised the relevance of zinc in both the pathophysiology and management of HE, particularly in resource-limited settings where simple nutritional interventions may yield significant clinical benefits [30].
Limitation
Despite these promising results, some limitations merit consideration. The study was conducted in a single centre, which may limit generalizability. Additionally, while cognitive outcomes were well captured through PHES, neuroimaging or biomarkers of oxidative stress could have provided mechanistic insights. The study also did not stratify patients based on their baseline zinc levels, which could have influenced their response to supplementation. Future randomised controlled trials with longer follow-up and stratification based on nutritional status are warranted to validate and expand upon these findings.
Conclusions
This study supports the use of zinc as an adjunct to lactulose in the treatment of MHE, particularly in accelerating cognitive improvement. While both therapies were effective, the combination therapy offered a more rapid clinical response, underscoring the potential utility of zinc in comprehensive HE management. These findings advocate for routine assessment of micronutrient status in cirrhotic patients and suggest that zinc supplementation may serve as a cost-effective, low-risk strategy to enhance outcomes in early hepatic encephalopathy.





