







Introduction
Secondary hyperparathyroidism (SHPT) is one of the common complications in end-stage renal disease (ESRD) [1, 2]. It is characterized by persistently increased parathyroid hormone (PTH) and mineral metabolism disorder. Clinical features of SHPT include soft tissue calcification, vascular calcification, bone pain, and fracture, which can affect life quality and increase mortality [3, 4]. For refractory SHPT, parathyroidectomy (PTX) is recommended in the practical guidelines [2]. PTX can significantly reduce the PTH levels, relieve the symptoms, and decrease the complications and mortality [5, 6]. Open parathyroidectomy (OPTX) is the traditional surgical method, which has disadvantages such as large surgical trauma and significant surgical scars left on the neck.
In recent years, minimally invasive treatment of refractory SHPT has been developed. In our previous meta-analysis and other studies, we found that thermal ablation was an effective minimally invasive treatment for refractory SHPT, but thermal ablation increased the risk of SHPT persistence and recurrence compared to OPTX [7, 8]. With the development of endoscopic technology, endoscopic parathyroidectomy (EPTX) has been gradually introduced as a minimally invasive treatment for refractory SHPT [9, 10]. However, the efficacy and safety are uncertain when comparing EPTX and OPTX for refractory SHPT. To determine the efficacy and safety of the 2 treatment methods for refractory SHPT, it is necessary to collect published data and perform a meta-analysis.
Aim
This meta-analysis was conducted based on the published literature to evaluate the efficacy and safety between EPTX and OPTX in patients with refractory SHPT.
Material and methods
Search strategy
Our meta-analysis was reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). We searched PubMed, EMbase, the Cochrane Library, CNKI (China National Knowledge Infrastructure), and Wanfang database from inception until 10 April 2023. The combined text and MeSH terms included secondary hyperparathyroidism, endoscopic parathyroidectomy, and open parathyroidectomy. In addition, the relevant references and cited papers were searched manually to identify additional studies meeting the inclusion criteria. There were no language restrictions.
Inclusion and exclusion criteria
The inclusion criteria were (1) randomized controlled trials (RCTs), cohort or case-control studies, (2) refractory SHPT with PTH levels > 800 pg/ml, persistent hypercalcaemia and hyperphosphataemia and poor response to medical therapy, parathyroid gland hyperplasia diagnosed by ultrasound or radionuclide imaging, (3) comparison of outcomes between EPTX and OPTX, (4) outcomes including at least one of the following indicators: operating time, intraoperative blood loss, hospital stay, serum PTH level, serum calcium level, serum phosphorus level, and recurrence, complications.
Exclusion criteria were as follows: (1) case series, comments, reviews, (2) patients who have undergone surgical treatment of parathyroid gland, (3) severe coagulation disorder, (4) severe cardiopulmonary dysfunction, and (5) lack of relevant outcome data.
Data extraction and quality assessment
Data were extracted independently by 2 investigators using standard data extraction forms. In the case of disagreement, a third investigator was consulted. We extracted characteristics including first author, year of publication, location, study design, sample size, mean age, sex, follow-up period, the amount of parathyroid gland removed, whether to perform autotransplantation (AT), and treatment outcomes. The Cochrane assessment tool was used to assess the quality of RCTs [11], and the Newcastle-Ottawa scale (NOS) was used to assess non-randomized studies [12].
Statistical analysis
This meta-analysis was performed using Review Manager Version 5.3 (Cochrane Collaboration). We summarized treatment outcomes as odds ratios (OR) for categorical variables and weighted mean differences for continuous variables with 95% confidence intervals (CIs). P < 0.05 was considered statistically significant. We used the I2 statistic to assess heterogeneity among studies. We considered I2 > 0% and p < 0.10 to indicate significant heterogeneity. Meta-analyses with insignificant heterogeneity were performed using the fixed-effects model. For meta-analyses with significant heterogeneity, the random-effects model was used. Publication bias was assessed using sensitivity analysis.
Results
Study selection and characteristics
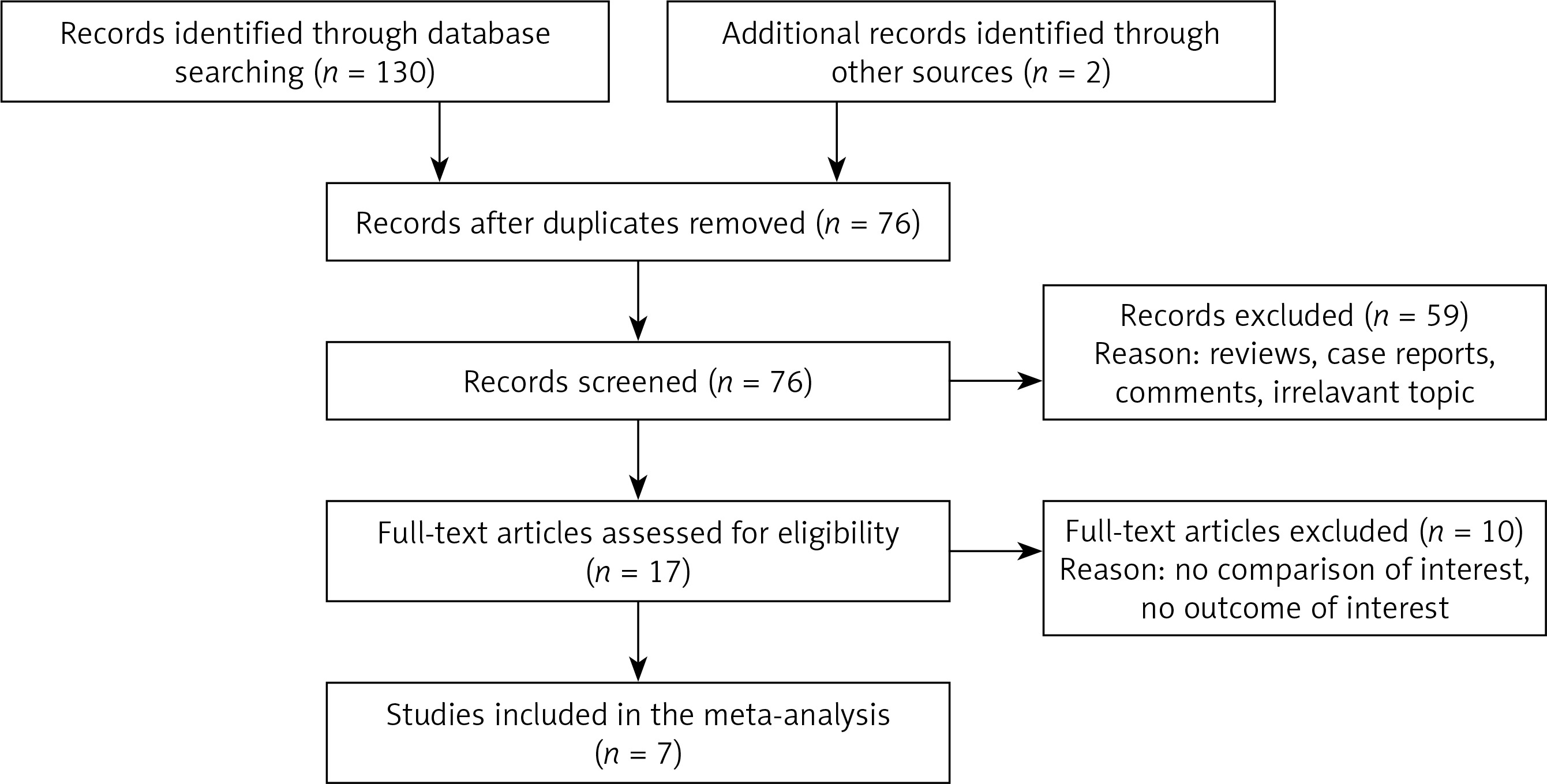
A flow diagram of the selection process is shown in Figure 1. Finally, a total of seven studies from China were included in this analysis [13–19]. Of the 7 studies, 5 were retrospective cohort studies, one was prospective cohort study, and one was an RCT. Overall, 249 patients were included in the OPTX group and 244 patients were included in the EPTX group. The risk of bias in the included RCTs was moderate. The cohort studies achieved scores of ≥ 6 points, which were considered to be of high quality. The baseline characteristics of these studies are listed in Table I. The Cochrane assessments are listed in Table II, and the NOS assessments are listed in Table III.
Table I
Characteristics of the included studies
| Study [year] | Country | Design | Follow-up period | Sample size | Mean age [years] | Male n (%) | PTH [pg/ml] | Calcium [mmol/l] | Phosphorus | The amount of parathyroid gland removed and whether to perform AT (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Zhang 2022 [13] | China | Retrospective cohort study | 3 months | OPTX: 24 EPTX: 25 | 53.0 ±9.5 53.5 ±10.1 | 10 (41.7) 12 (48.0) | 2450.13 ±266.74 2386.48 ±281.23 | 2.32 ±0.15 2.29 ±0.16 | 1.56 ±0.20 1.60 ±0.23 | TPTX (100) TPTX (100) |
| Qin 2020 [14] | China | RCT | – | OPTX: 41 EPTX: 41 | 43.3 ±3.6 43.7 ±3.4 | 18 (43.9) 19 (46.3) | 2017.34 ±416.87 2108.27 ± 422.74 | – | – | TPTX (100) TPTX (100) |
| Ma 2021 [15] | China | Retrospective cohort study | 6 months | OPTX: 46 EPTX: 49 | 43.8 ±5.6 44.4 ±5.4 | 25 (54.3) 27 (55.1) | 935.76 ±81.39 963.51 ±82.76 | 1.94 ±0.27 1.96 ±0.28 | 2.10 ±0.10 2.09 ±0.08 | TPTX + AT (100) TPTX + AT (100) |
| Jin 2018 [16] | China | Retrospective cohort study | 12 months | OPTX: 30 EPTX: 26 | 45.4 ±10.5 42.2 ±9.5 | 12 (40.0) 11 (42.3) | 2219.45 ±527.36 1985.12 ±427.36 | 2.46 ±0.13 2.48 ±0.16 | 2.07 ±0.26 2.18 ±0.32 | TPTX + AT (55.3) or TPTX (44.7) TPTX + AT (61.5) or TPTX (38.5) |
| Cui 2014 [17] | China | Retrospective cohort study | 6 months | OPTX: 25 EPTX: 22 | 46.5 45.2 | 15 (60.0) 13 (59.1) | – | – | – | TPTX + AT (100) TPTX + AT (100) |
| Xu 2022 [18] | China | Prospective cohort study | 12 months | OPTX: 50 EPTX: 47 | 56.8 ±10.0 56.2 ±10.8 | 14 (28.0) 12 (25.5) | 2137.77 ±528.14 2142.06 ±528.65 | 3.42 ±0.29 3.39 ±0.25 | – | TPTX + AT (100) TPTX + AT (100) |
| Sun 2009 [19] | China | Retrospective cohort study | 21.6 months | OPTX: 33 EPTX: 34 | – | 15 (45.5) 13 (38.2) | 1775.59 ±88.94 – | 2.61 ±0.36 – | 2.55 ±0.58 – | TPTX + AT (100) TPTX + AT (100) |
Table II
Quality assessment of randomized control trials
| Study | Random sequence generation | Allocation concealment | Blinding of participants and personnel | Incomplete outcome data | Selective reporting | Other bias |
|---|---|---|---|---|---|---|
| Jingyi Qin 2020 | + | ? | ? | + | + | ? |
Table III
Quality assessment of cohort studies
| Studies | Selection | Comparability | Outcome | Score |
|---|---|---|---|---|
| Changguo Jin 2018 | ★★★★ | ★ | ★★ | 7 |
| Fei Xu 2022 | ★★★ | ★ | ★★ | 6 |
| Hengfeng Cui 2014 | ★★★★ | ★ | ★ | 6 |
| Mengyao Zhang 2022 | ★★★★ | ★ | ★★ | 7 |
| Xiaofei Ma 2021 | ★★★★ | ★ | ★★ | 7 |
| Yueming Sun 2009 | ★★★ | ★ | ★★ | 6 |
[i] The Cohort studies were evaluated using the Newcastle-Ottawa scale, which comprises the study of selection (representativeness of the exposed group, representativeness of the non-exposed group, ascertainment of exposure, demonstration that outcome of interest was not present at start of study), group comparability (controls for the most important factor, controls for any additional factors), outcome measures (assessment of outcome, was follow-up long enough for outcomes to occur? Adequacy of follow-up of cohorts), a total of 9 points. ★, 1 point.
Meta-analysis results
Operation time
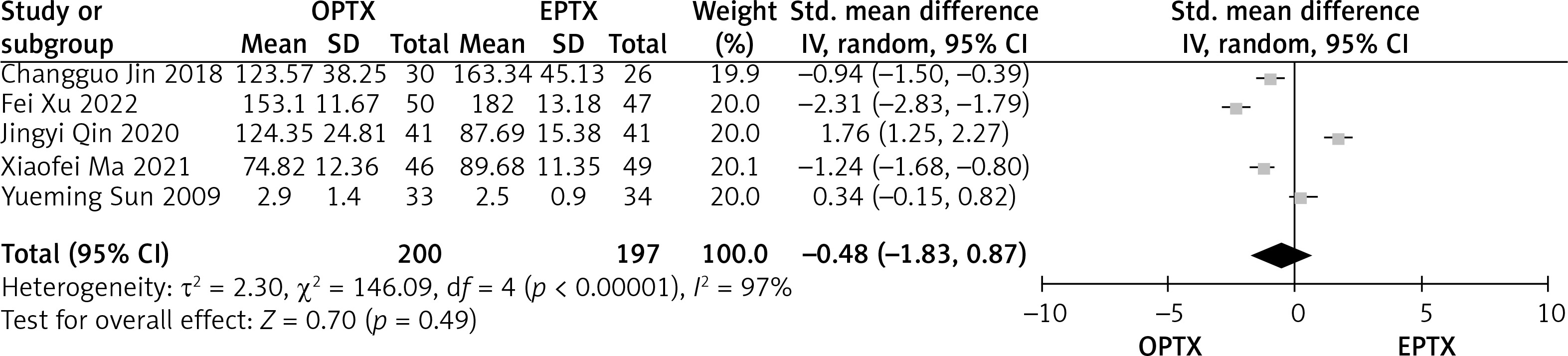
The data about the operation time were reported in 5 articles. The heterogeneity between the EPTX and OPTX group was substantial (p < 0.01, I2 = 97%). There was no significant difference between the EPTX and OPTX group concerning the operation time (MD = –0.48, 95% CI: -1.83–0.87, p = 0.49) (Figure 2).
Intraoperative blood loss
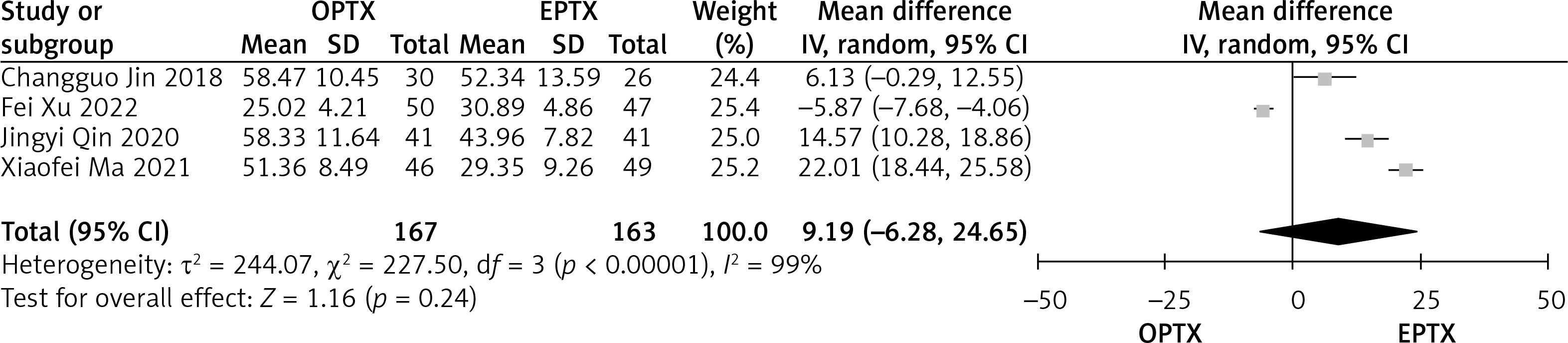
The data about the intraoperative blood loss were reported in 4 articles. The heterogeneity between the EPTX and OPTX group was substantial (p < 0.01, I2 = 99%). There was no significant difference between the EPTX and OPTX group concerning the intraoperative blood loss (MD = 9.19, 95% CI: -6.28–24.65, p = 0.24) (Figure 3).
Hospital stay
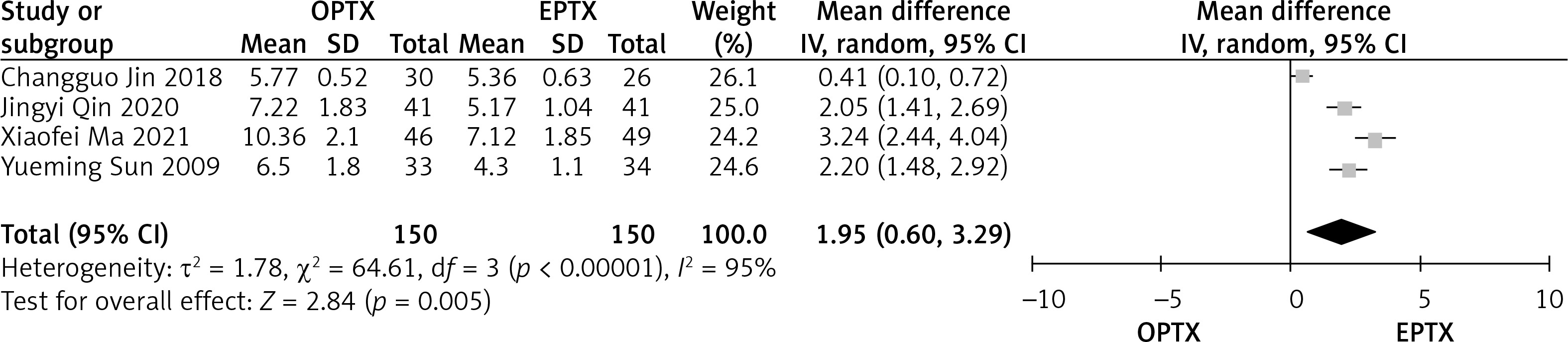
Data about the hospital stay were reported in 4 articles. The heterogeneity between the EPTX and OPTX group was substantial (p < 0.01, I2 = 95%). The hospital stays in the EPTX group were shorter than in the OPTX group, and the difference was statistically significant (OR = 1.95, 95% CI: 0.60–3.29, p < 0.01) (Figure 4).
Serum PTH level
Data about the serum PTH levels after operation were reported in 3 articles. The heterogeneity between the EPTX and OPTX group was substantial (p < 0.01, I2 = 98%). There was no significant difference between the EPTX and OPTX group concerning the serum PTH levels (MD = 21.66, 95% CI: -13.29–56.61, p = 0.22) (Figure 5).

Serum calcium level
Data about the serum calcium levels after operation were reported in 3 articles. The heterogeneity between the EPTX and OPTX group was substantial (p = 0.05, I2 = 69%). There was no significant difference between the EPTX and OPTX group concerning the serum calcium levels (MD = 0.00, 95% CI: -0.10–0.09, p = 0.93) (Figure 6).

Serum phosphorus level
Data about the serum phosphorus levels after operation were reported in 2 articles. The heterogeneity between the EPTX and OPTX group was substantial (p < 0.01, I2 = 97%). There was no significant difference between the EPTX and OPTX group concerning the serum phosphorus levels (MD = 0.10, 95% CI: -0.12–0.33, p = 0.37) (Figure 7).

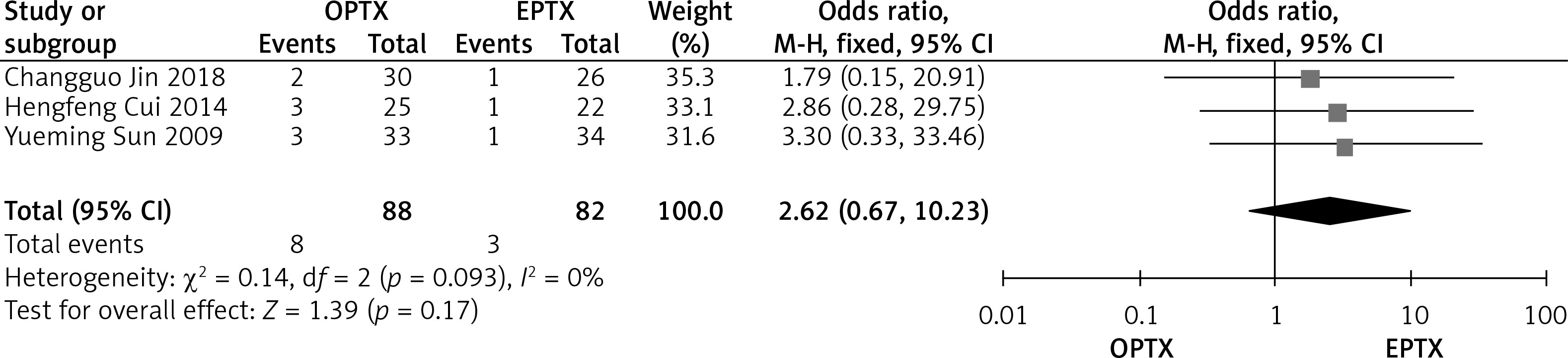
Recurrence
Data about the recurrence after operation were reported in 3 articles. The heterogeneity between the EPTX and OPTX group was not substantial (p = 0.93, I2 = 0%). There was no significant difference between the EPTX and OPTX group concerning the recurrence (OR = 2.62, 95% CI: 0.67–10.23, p = 0.17) (Figure 8).
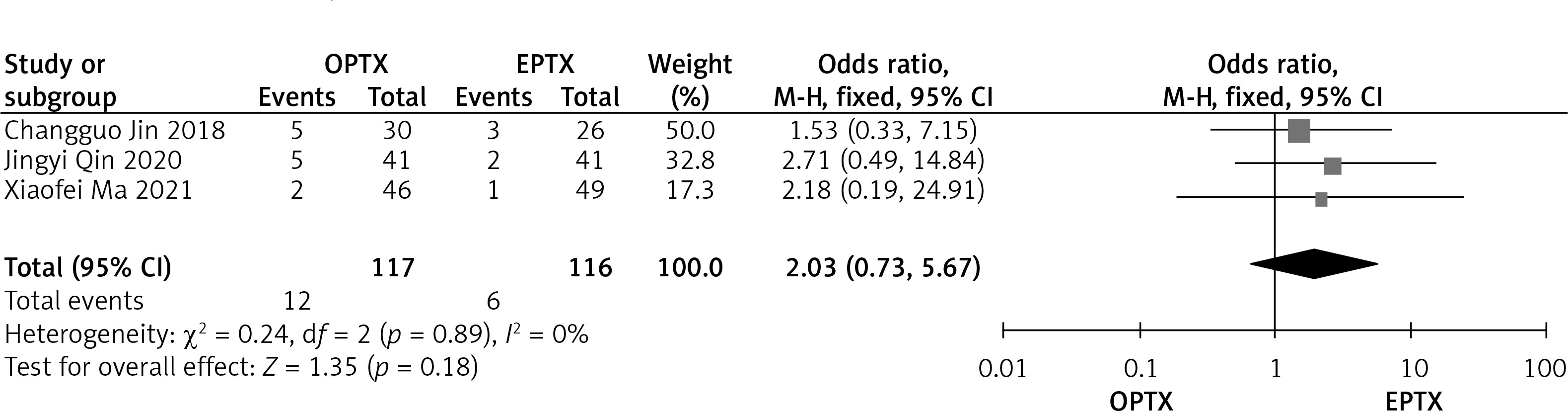
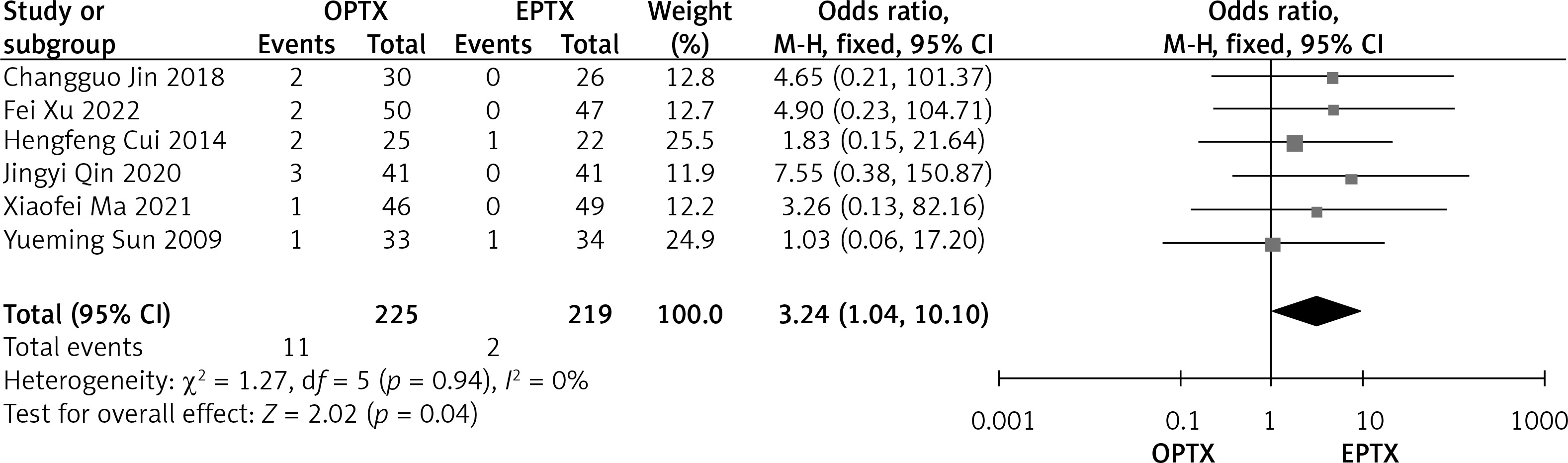
Complications
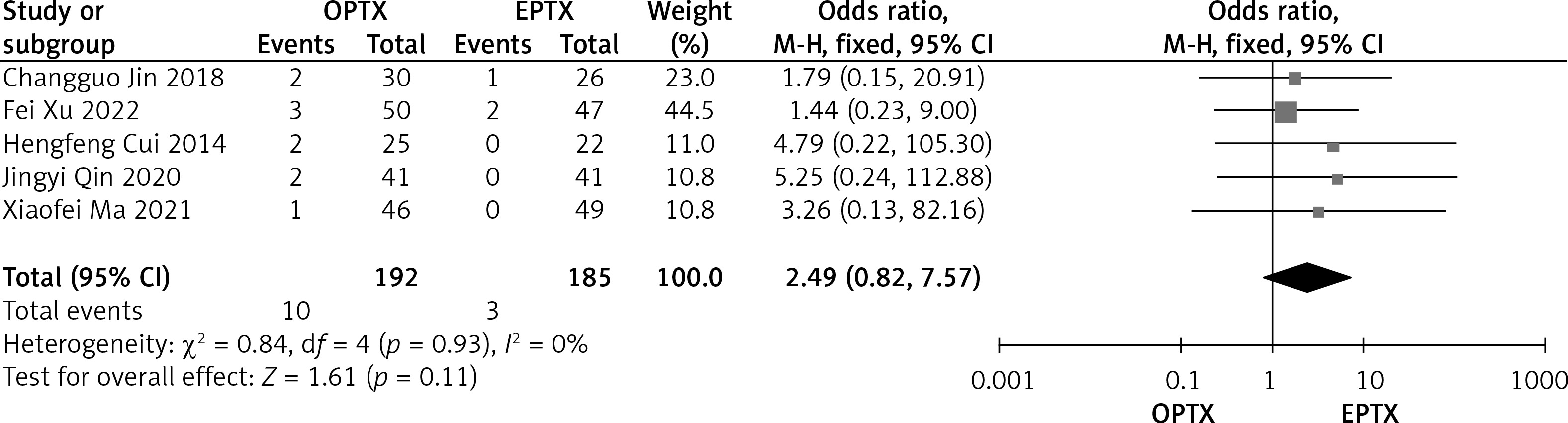
Data about the complications after operation were reported in 6 articles. Incidences of neck ecchymosis (6.0%, 7/117), subcutaneous haematoma (10.3%, 12/117), hoarseness or recurrent laryngeal nerve injury (4.9%, 11/225), and wound infection (5.2%, 10/192) occurred in the OPTX group. Incidences of neck ecchymosis (5.3%, 6/116), subcutaneous haematoma (5.3%, 6/116), hoarseness or recurrent laryngeal nerve injury (1.0%, 2/219), and wound infection (1.6%, 3/185) occurred in the EPTX group. There was no statistical significant difference between the EPTX and OPTX group concerning the incidence of the neck ecchymosis (OR = 1.10, 95% CI: 0.35–3.41, p = 0.87), subcutaneous haematoma (OR = 2.03, 95% CI: 0.7 3–5.67, p = 0.18), and wound infection (OR = 2.49, 95% CI: 0.82–7.57, p = 0.11). The incidences of hoarseness or recurrent laryngeal nerve injury in the EPTX group were lower than in the OPTX group, the difference was statistically significant (OR = 3.24, 95% CI: 1.04–10.10, p = 0.04). All forest plots of the complications after operation are listed in Figures 9–12.
Figure 9
Forest plots comparing the incidence of neck ecchymosis between EPTX and OPTX group in patients with refractory SHPT
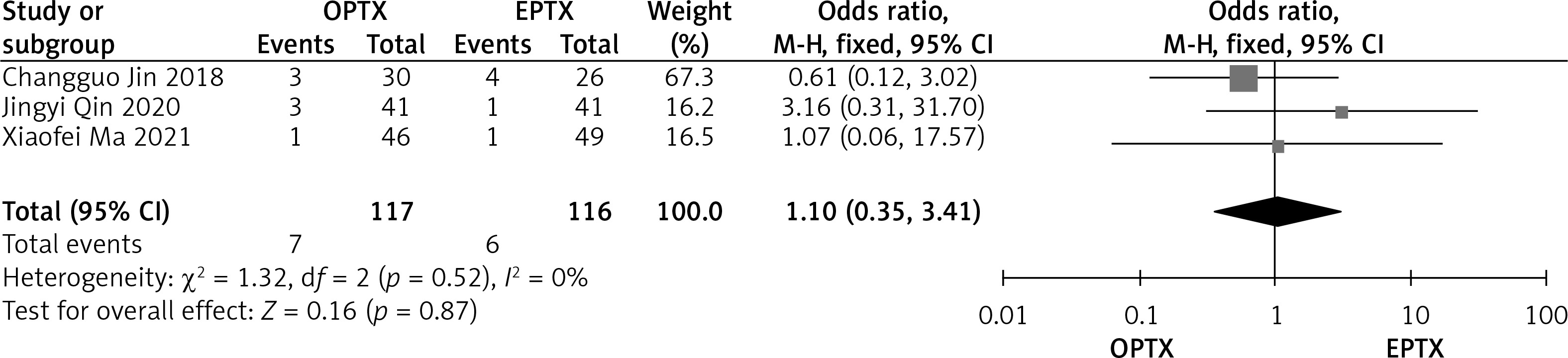
Figure 10
Forest plots comparing the incidence of subcutaneous hematoma between EPTX and OPTX group in patients with refractory SHPT
Sensitivity analyses
The sensitivity analyses for all outcomes were used to judge the dependability of the results. We deleted the study of Fei Xu because the result of the meta-analysis showed that the intraoperative blood loss in the EPTX group was lower statistically than in the OPTX group (p < 0.01). We deleted the study of Xiaofei Ma because the results of the meta-analysis showed that the serum phosphorus levels in the EPTX group were lower statistically than in the OPTX group (p < 0.01). We deleted one study at a time from the study of Changguo Jin, Fei Xu, Jingyi Qin, and Xiaofei Ma because the results of the meta-analysis showed that there was no significant difference between the EPTX and OPTX group concerning the incidences of hoarseness or recurrent laryngeal nerve injury (p > 0.05).
Discussion
OPTX is the classic treatment for refractory SHPT and has been used for more than half a century [7, 20]. However, OPTX has large trauma, and it may lead to the occurrence of ecchymoma, recurrent laryngeal nerve injury, and other complications, which is not conducive to the recovery of patients [21]. OPTX also brings obvious postoperative scarring, which may cause psychological trauma to female patients who have high requirements for aesthetics. EPTX is a minimally invasive treatment for refractory SHPT; simultaneously, it has aesthetic advantages compared with OPTX. However, there is no consensus on which is better between OPTX and EPTX concerning the efficacy and safety for the treatment of refractory SHPT.
We performed a meta-analysis comparing OPTX and EPTX in patients with refractory SHPT. EPTX and OPTX are both effective methods to reduce PTH levels. Under the magnification and illumination of the endoscope, EPTX is better in finding all the parathyroid glands to achieve complete resection of the parathyroid glands and ensure the success of the operation [16–18]. However, our meta-analysis did not show an obvious difference concerning the postoperative PTH, calcium, phosphorus levels, and the recurrence rate between the 2 surgical methods.
We also found that EPTX had lower incidences of neck ecchymosis, subcutaneous haematoma, wound infection and hoarseness, or recurrent laryngeal nerve injury compared with OPTX, but EPTX only had a statistically obvious advantage in reducing the incidence of hoarseness or recurrent laryngeal nerve injury. Most of the included articles reported that EPTX reduced intraoperative blood loss, but the results of the meta-analysis did not show that EPTX had an obvious advantage in reducing intraoperative blood loss. Theoretically, EPTX has the following advantages. Firstly, EPTX can better identify recurrent laryngeal nerve and small blood vessels under the magnification and illumination of the endoscope [16–18]. Secondly, using an ultrasonic knife, EPTX has remarkable effect of haemostasis [14, 16–18]. Thirdly, in EPTX, most recurrent laryngeal nerves need not be exposed, but OPTX often requires exposure of recurrent laryngeal nerves. There is a risk of damaging the recurrent laryngeal nerves in the process of exposing the recurrent laryngeal nerves [14, 16, 17]. Fourthly, EPTX is performed in a closed chamber with reduced contact with the outer boundary environment, which can reduce the risk of infection [14, 16]. In our meta-analysis, EPTX did not show any obvious advantage in reducing the incidence of bleeding and infection, which should be explored and verified in further studies. In addition, we found that patients with EPTX had shorter hospital stay compared with OPTX patients. Recovery was faster in the EPTX group because of the smaller incision and lower overall complication rate.
There were some limitations to our meta-analysis. Firstly, it was not uniform in the included study concerning the amount of parathyroid gland removed and whether to perform AT. Secondly, the definition of postoperative recurrence is not uniform in the included articles. Thirdly, the number of the included articles was small. Sensitivity analysis showed that the dependability of some outcomes were not enough.
Conclusions
Our meta-analysis revealed that EPTX and OPTX are both effective methods for patients with refractory SHPT. EPTX had the shorter hospital stay and lower incidence of hoarseness or recurrent laryngeal nerve injury compared with OPTX. However, there were no significant differences concerning operating time, intraoperative blood loss, serum PTH level, serum calcium level, serum phosphorus level, recurrence, and complications including the neck ecchymosis, subcutaneous haematoma, and wound infection. To confirm these conclusions, further large RCTs comparing EPTX and OPTX for the treatment of refractory SHPT are necessary.