
Introduction
Liver cancer is the sixth most common cause of cancer deaths in the world with an estimation of 841,000 cases (9.3 cases per 100,000 people per year) and 782,000 deaths (8.5 deaths per 100,000 people per year) in 2018 [1]. Hepatocellular carcinoma (HCC) is the primary tumor of the liver and accounts for approximately 75% of all liver cancers [2]. It is more common in men (1 in 45 men vs. 1 in 113 women) [3] and has an average five-year survival of less than 15% [4]. Viral infections including hepatitis B virus (HBV) and hepatitis C virus (HCV), alcoholic liver disease, and nonalcoholic fatty liver disease are the most important risk factors for HCC [5]. According to the World Health Organization, HCC is expected to grow so that by 2030 it will rank as the second most common cancer in humans [6]. In addition to environmental factors, genetic factors can affect the development and incidence of HCC [7]. HCC is always associated with persistent inflammation of the liver tissues; however, the roles of tumor enhancers and the predictive value of inflammatory cytokines within the tumor are unclear [8]. Apart from ambiguities, inflammation is highly dependent on the cytokine-mediated immune response, in which a strong immune response causes chronic hepatitis, and a weak response can be a carcinogen in HBV or HCV carriers because persistent infection in the hepatic microenvironment promotes HCC progression [9, 10]. It has been shown that cytokine genes and their receptors are highly polymorphic, and that cytokine polymorphisms can affect the expression of cytokines that control the immune response, opening the gate to understanding the complex mechanisms of disease at the molecular level [11]. Many reports have focused on the genetic polymorphism of cytokines as host genetic factors in hepatitis HCC because they may indicate the complexity of HCC occurrence due to HBV or HCV as etiologic factors [11]. In addition to the development of the disease, it has been reported that several mutations in cytokine genes can be significantly associated with response to HCV/HBV treatment and spontaneous clearance [12, 13]. A recent meta-analysis reported an elevated risk of IL-6 polymorphisms in HCC patients [14]. Interleukin 8 (IL-8) is one of the most common cytokines and belongs to the CXC family of chemokines that stimulate the uptake of neutrophils and lymphocytes and represent a large range of proinflammatory effects [15]. This cytokine plays a significant role in the pathogenesis of several malignancies, including tumor angiogenesis, growth, metastasis, and invasion [16-18]. A recent meta-analysis showed the increased risk for serum IL-8 level in HCC patients [19]. In addition, another meta-analysis in 2016 [20] reporting the association between several IL-8 polymorphisms (+781C/T, +396T/G, +678T/C, +2767A/T, and +1633C/T) and the risk of several cancers based on 22 case-control studies showed a protective role of IL-8 (+781C/T) polymorphism in HCC patients. The IL-8 gene is located on chromosome 4q13-q21 in humans and evidence suggests that polymorphisms in IL-8 are associated with IL-8 production or protein expression and ultimately impact the function of genes [21, 22]. IL-8 polymorphisms of -251T/A and +781C/T are located on the promoter and intron 1 regions, respectively [23]. The aim of this study was to evaluate IL-8 polymorphisms (-251T/A and +781C/T) in patients with HCC in a meta-analysis study.
Material and methods
One reviewer (M.S.) retrieved the studies of the meta-analysis by the search terms (“interleukin 8” or “IL-8”) and “liver cancer” or “hepatocellular carcinoma” or “HCC”) and (“allele” or “polymorphism” or “genotype” or “variant”) in Scopus, Web of Science, PubMed, and Cochrane Library databases up to 21 November 2020.
Study selection and selection criteria
The studies on the association between IL-8 polymorphisms and the risk of HCC were selected with no restrictions of age, gender, language, or time. The studies were included if they: 1) were case-control reporting the HCC patients and healthy controls as the control group; 2) included IL-8 polymorphisms of -251T/A and +781C/T; 3) reported HCC diagnosis pathologically; 4) reported healthy control subjects without systematic diseases; 5) reported HCC patients with/without hepatitis and/or liver cirrhosis. The studies were excluded if they did not have control groups and conference papers. One reviewer (O.E.A.) checked the relevant articles based on the eligibility criteria.
Data extraction
The studies included in the meta-analysis were checked by one reviewer (M.S.) for extracting the relevant data. Another author (O.E.A.) re-evaluated the data. Disagreements were resolved by the third reviewer (Fr.M.).
Quality assessment
Two reviewers (M.S. and Fa.M.) independently evaluated the quality of the retrieved studies by scoring them. We developed a quality evaluation tool specifically for this meta-analysis, which consisted of 9 criteria. The range of scores varies from 0 to 14, with higher scores indicating better study quality.
Statistical analyses
The Cochrane Q test and I2 statistic were used to evaluate the heterogeneity between the studies. The analyses were done by Review Manager 5.3 (RevMan 5.3, The Cochrane Collaboration, Oxford, United Kingdom) with a random-effects model using odds ratios (ORs) and 95% confidence intervals (CIs) which, given the lack of heterogeneity (I2 < 50% [Ph or Pheterogeneity > 0.1]), led to use of a fixed-effects model. The funnel plot analyses with both Begg’s and Egger’s tests (for evaluation of publication bias across the studies) and sensitivity analyses (for confirming the stability of the results) – one removed study and cumulative analysis – were performed by Comprehensive Meta-Analysis 2.0 (CMA 2.0) software. The p-value (2-sided) < 0.05 was considered statistically significant. The analysis was performed by one author (M.S.). Finally, all authors revised the final version of the manuscript.
Results
Study selection
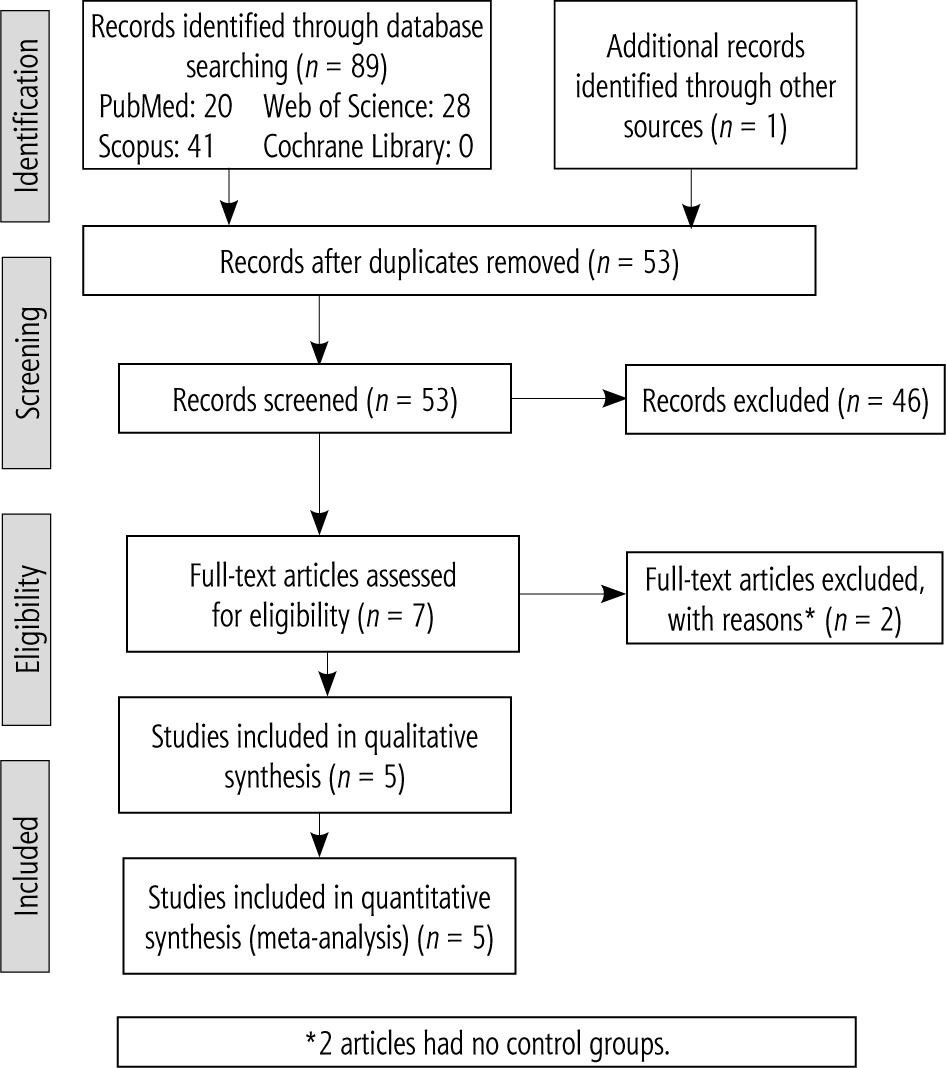
Searching databases/sources, 90 records were retrieved (Fig. 1). After removing duplicates and irrelevant records, seven full texts were screened. Out of all full-text articles, 2 articles were removed with reasons (two articles had no control groups). Then, five articles including ten studies were entered into the meta-analysis.
Quality evaluation
Ten criteria with a maximum score of 14 are shown in Table 1.
Table 1
Criteria for quality of study
Characteristics of the studies
Five studies [22, 24-27] included 1052 HCC cases and 1249 controls (Table 2). Three studies [22, 26, 27] reported from China, one [24] from Taiwan, and one [25] from Egypt. The quality score of all studies was ≥ 11. The source of controls and genotyping methods were the same in all studies.
Table 2
Characteristics of studies included in the meta-analysis
| First author, publication year | Country | Control source | Genotyping method | Number of patients | Number of controls | Quality score |
|---|---|---|---|---|---|---|
| Chien, 2011 [24] | Taiwan | Hospital-based | PCR-RFLP | 131 | 340 | 11 |
| Qin, 2012 [26] | China | Hospital-based | PCR-RFLP | 150 | 150 | 11 |
| Wang, 2014 [22] | China | Hospital-based | PCR-RFLP | 205 | 208 | 12 |
| Elsamanoudy, 2015 [25] | Egypt | Hospital-based | PCR-RFLP | 112 | 105 | 11 |
| Xiaohua, 2015 [27] | China | Hospital-based | PCR-RFLP | 454 | 446 | 12 |
The prevalence of genotypes and p-value of the Hardy-Weinberg equilibrium (HWE) for control groups for IL-8 polymorphisms (-251T/A and +781C/T) are shown in Table 3. The control group in one study [26] showed a deviation from HWE for IL-8 (+781C/T) polymorphism.
Table 3
Prevalence of genotypes of IL-8 polymorphisms (-251T/A and +781C/T) included in the meta-analysis
| First author, publication year | -251T/A | +781C/T | HWE* | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HCC patients | Controls | HCC patients | Controls | |||||||||||
| TT | TA | AA | TT | TA | AA | CC | CT | TT | CC | CT | TT | -251T/A | +781C/T | |
| Chien, 2011 [24] | 55 | 59 | 17 | 117 | 159 | 64 | 65 | 57 | 9 | 126 | 164 | 50 | 0.445 | 0.775 |
| Qin, 2012 [26] | 45 | 83 | 22 | 41 | 84 | 25 | 64 | 68 | 18 | 57 | 80 | 13 | 0.103 | 0.041 |
| Wang, 2014 [22] | 65 | 103 | 37 | 90 | 88 | 30 | 80 | 105 | 20 | 76 | 96 | 36 | 0.266 | 0.549 |
| Elsamanoudy, 2015 [25] | 29 | 56 | 27 | 33 | 49 | 23 | 68 | 36 | 8 | 36 | 45 | 24 | 0.551 | 0.177 |
| Xiaohua, 2015 [27] | 108 | 293 | 53 | 172 | 197 | 77 | 175 | 236 | 43 | 202 | 183 | 61 | 0.115 | 0.062 |
Meta-analysis
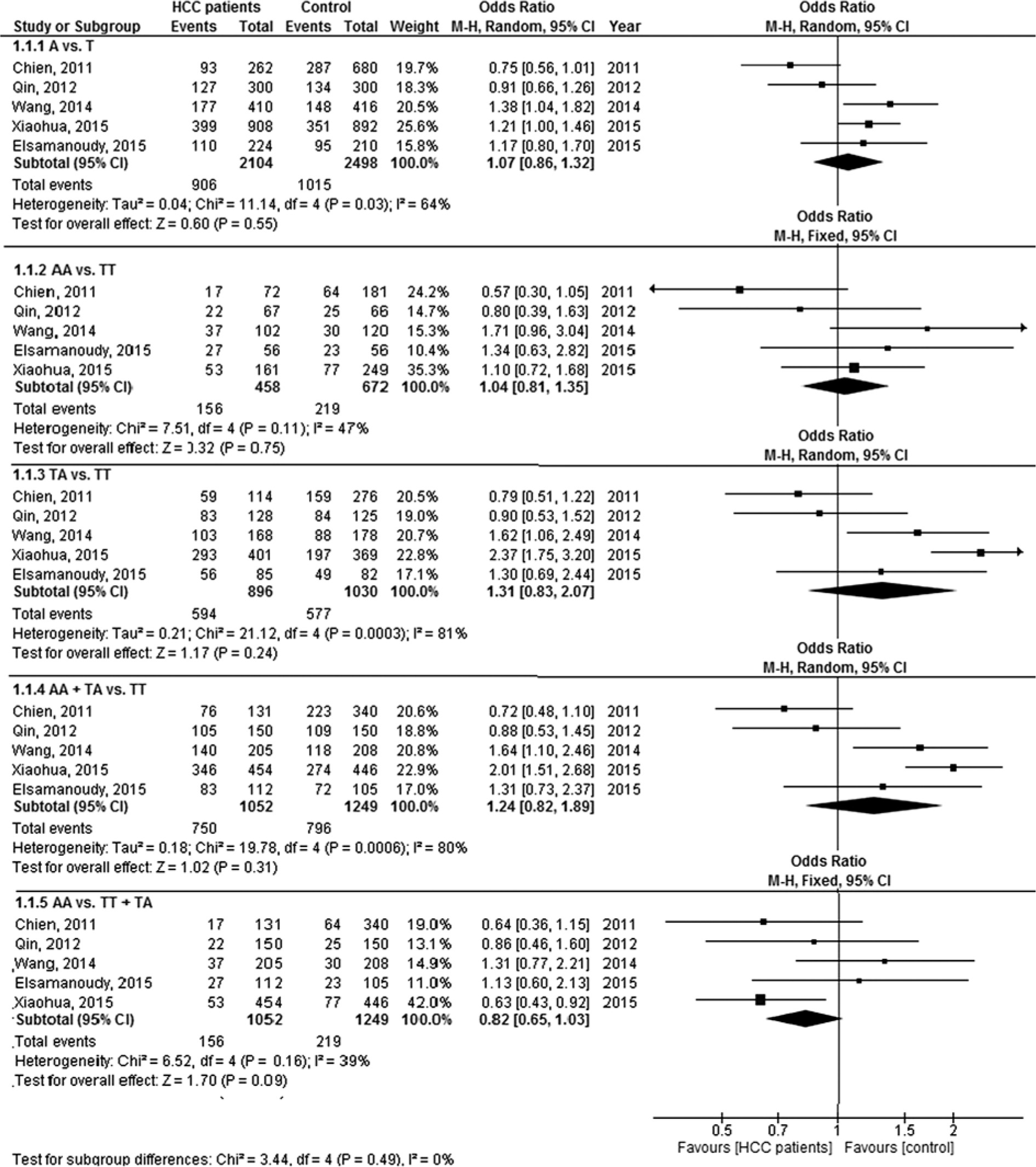
The forest plot analysis of IL-8 (-251T/A) polymorphism based on five genetic models in HCC patients compared to controls is shown in Figure 2. The pooled ORs were 1.07 (95% CI: 0.86, 1.32, p = 0.55, I2 = 64%), 1.04 (95% CI: 0.81, 1.35, p = 0.75, I2 = 47%), 1.31 (95% CI: 0.83, 2.07, p = 0.24, I2 = 81%), 1.24 (95% CI: 0.82, 1.89, p = 0.31, I2 = 80%), and 1.85 (95% CI: 0.63, 1.15, p = 0.29, I2 = 39%) for allele, homozygote, heterozygote, recessive and dominant models, respectively. The results did not confirm a significant association between IL-8 (-251T/A) polymorphism and the risk of HCC.
Fig. 2
Forest plot of interleukin-8 (-251T/A) polymorphism based on five genetic models in hepatocellular carcinoma patients versus controls
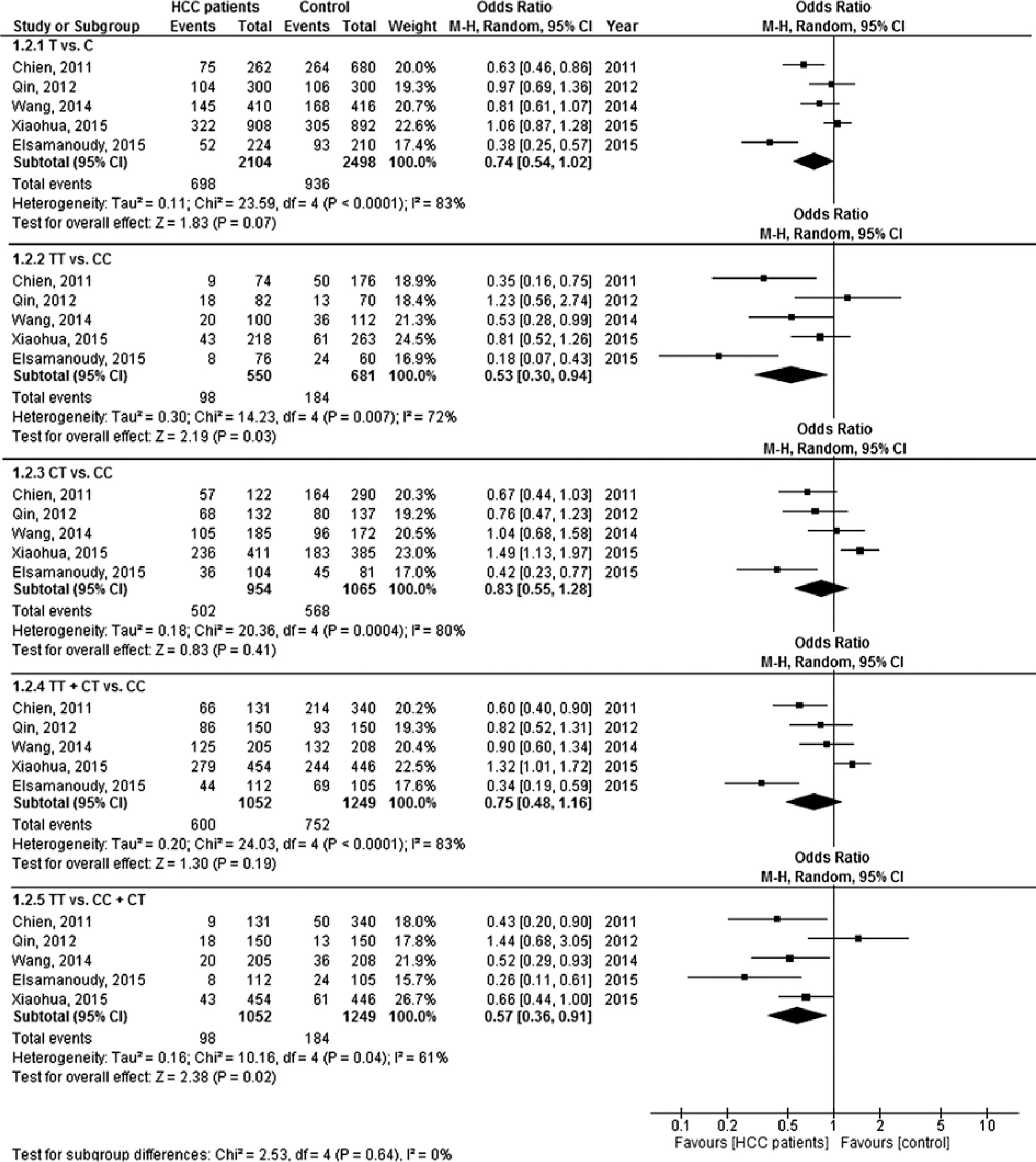
A forest plot analysis of IL-8 (+781C/T) polymorphism based on five genetic models in HCC patients compared to controls is shown in Figure 2. The pooled ORs were 0.74 (95% CI: 0.54, 1.02, p = 0.07, I2 = 83%), 0.53 (95% CI: 0.30, 0.94, p = 0.03, I2 = 72%), 0.83 (95% CI: 0.55, 1.28, p = 0.41, I2 = 80%), 0.75 (95% CI: 0.48, 1.16, p = 0.19, I2 = 83%), and 0.57 (95% CI: 0.36, 0.91, p = 0.02, I2 = 61%) for allele, homozygote, heterozygote, recessive, and dominant models, respectively. Therefore, the TT genotype of this polymorphism had a protective role in HCC patients compared to controls.
Sensitivity analysis
The “one removed study” and “cumulative analysis” showed stability of the results. In addition, removing one study [26] with a deviation from HWE in the control group for IL-8 (+781C/T) polymorphism, the new results confirmed previous results and even with more power for homozygote (OR = 0.44, 95% CI: 0.24, 0.81, p = 0.009, I2 = 72%) and dominant models with low heterogeneity (OR = 0.52, 95% CI: 0.39, 0.69, p < 0.00001, I2 = 27%).
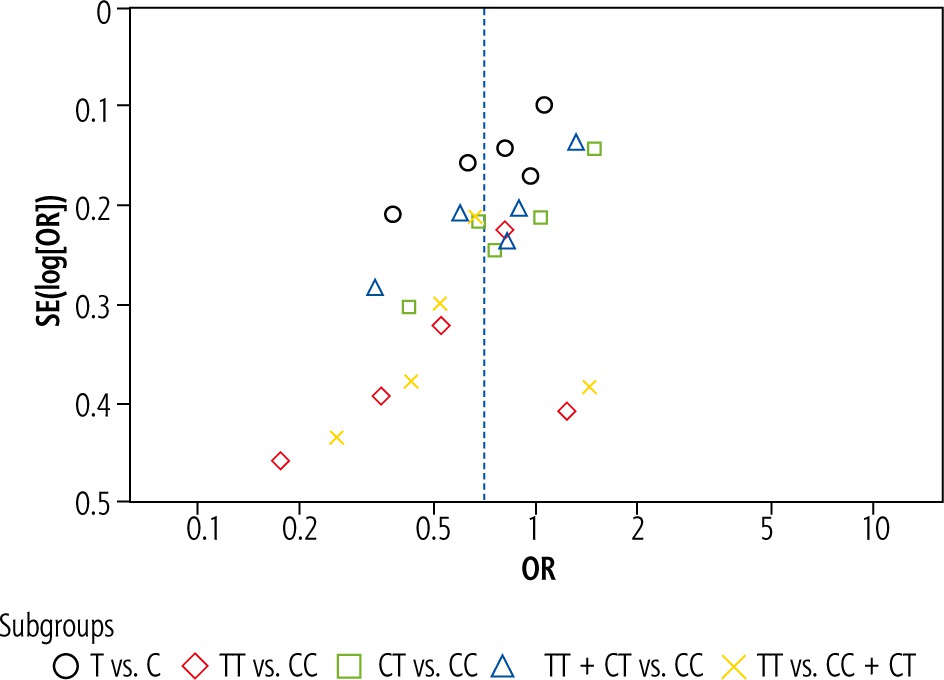
Publication bias
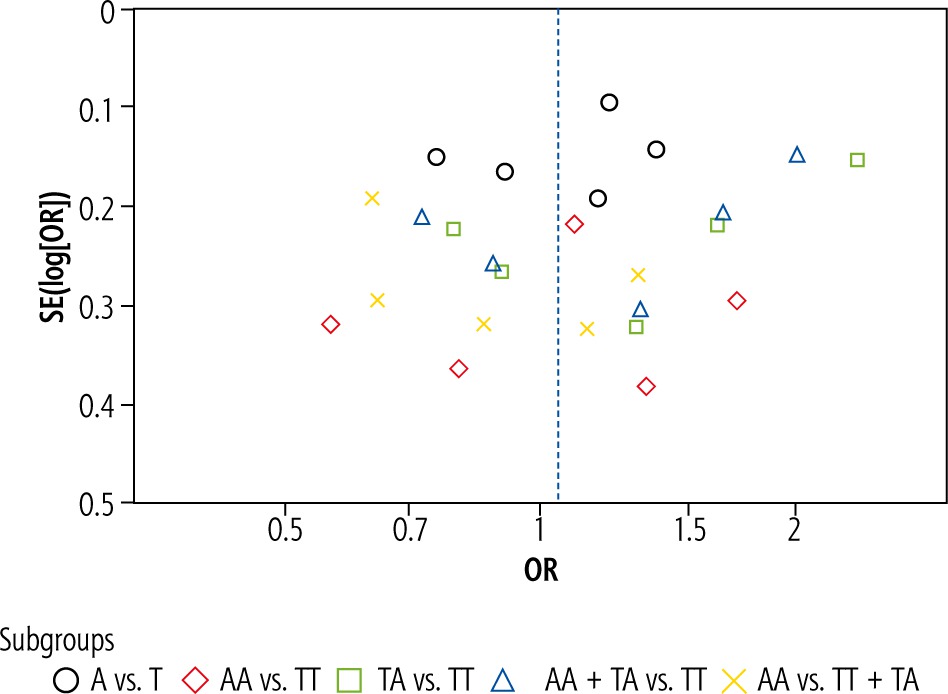
Neither Egger’s nor Begg’s test revealed publication bias between the studies including IL-8 polymorphisms (-251T/A and +781C/T) (Figs. 4 and 5) except for heterozygote and recessive models of IL-8 (+781C/T) polymorphism, for which Egger’s test showed publication bias (p = 0.01375 and p = 0.03072).
Fig. 3
Forest plot of interleukin-8 (+781C/T) polymorphism based on five genetic models in hepatocellular carcinoma patients versus controls
Discussion
A positive or negative effect can be seen by inflammatory cytokines on the development of HCC [28]. Molecular mechanisms leading to the development and growth of HCC are very complex and can result from significant genetic and epigenetic changes [29]. Of the fifteen IL-8 polymorphisms known until 2004, only -251A/T and +781C/T polymorphisms were associated with altered IL-8 mRNA levels [30, 31]. The findings of the present meta-analysis confirmed a lack of significant association between IL-8 (-251T/A) polymorphism and the risk of HCC, whereas IL-8 (+781C/T) polymorphism was associated with HCC risk.
IL-8 is a neutrophil stimulator with biological functions including inducing T lymphocyte migration, stimulating tumor growth and angiogenesis, and inhibiting collagen synthesis, which is produced by a wide range of different cell types in response to various inflammatory stimuli [22]. Two studies [22, 27] showed an association between IL-8 (-251T/A) polymorphism and susceptibility to HCC, whereas three studies [24-26] did not find any association between the polymorphism and HCC risk, in line with the present meta-analysis. In addition, four studies [22, 24, 25, 27] reported an association between IL-8 (+781C/T) polymorphism and susceptibility to HCC, in line with the present meta-analysis and another meta-analysis [20] reporting a protective role of this polymorphism in HCC patients, whereas one study [26] did not find any association between the polymorphism and HCC susceptibility. It is known that the cause of cancer is the interaction of genetic factors and environmental exposure, such as HBV or HCV infection, excessive alcohol consumption, and various risk factors for HCC [26]. Therefore, one should pay attention to interactions between genetic and environmental factors for understanding the association between polymorphisms and the risk of HCC in the future.
One study [26] revealed that the AA genotype of IL-8 (-251T/A) polymorphism had a protective role in liver cirrhosis, but this polymorphism was not associated with the risk of chronic HBV. Another study [24] showed that +781C/T and -251T/A polymorphisms had no significant association with any clinicopathological characteristics of HCC. However, HCC patients with at least one mutated A allele (TA + AA) of -251T/A polymorphism had around the three-fold elevated risk of HBV infection in comparison with HCC patients with TT genotype after adjusting for age, sex, smoking, and alcohol consumption. In addition, the serum IL-8 level of HCC patients carrying the A allele could be higher than in HCC patients carrying the T allele [24]. In the present meta-analysis, because of the small number of studies included, we could not analyze the association between the polymorphisms and clinicopathological features of HCC. However, more studies are needed to focus on this association so that a more comprehensive meta-analysis can be performed in the future to verify the results.
Our meta-analysis had three important limitations: 1) a lack of subgroup analysis due to the small number of studies reported, 2) existence of bias in two models of +781C/T polymorphism, 3) existence of high heterogeneity in most analyses. The strengths were: 1) high quality of all studies, 2) the same source of controls and genotyping methods.
Conclusions
The meta-analysis reported a lack of significant association between IL-8 (-251T/A) polymorphism and the risk of HCC, whereas the TT genotype of IL-8 (+781C/T) polymorphism had a protective role in HCC. The existence of this protective role can help clinicians in the treatment process of HCC patients in the future. Future studies including more cases and different areas should consider the interactions between genetic and environmental factors.





