
Introduction
Advances in early detection and improved treatment of breast cancer have resulted in increased chances of survival after diagnosis, resulting in a lot of women living with the consequences of cancer treatment [1]. The adverse side effects of chemotherapy treatment include, among others, pain, fatigue, cachexia (wasting syndrome), diminished strength and lung capacity, and reduced range of movement [2–5].
There is evidence that women successfully treated for breast cancer have ongoing morbidity with symptoms of dyspnoea, exercise intolerance (reduced exercise tolerance as measured by peak oxygen consumption), and reduced physical capacity [6–10]. Effort dyspnoea and exercise intolerance in breast cancer survivors are associated not only with increased ventilatory demand secondary to deconditioning, but also with reduced inspiratory capacity (IC) and inspiratory muscle weakness [11].
Currently, physiotherapy forms the main intervention technique applied in preventing these complications. Respiratory physiotherapy forms a core specialty within physiotherapy and plays a key role in treatment of patients with respiratory diseases [12, 13]. A variety of interventions, including pulmonary rehabilitation, early mobilisation, and airway clearance techniques have demonstrated beneficial effects on symptoms associated with respiratory diseases. These include enhanced pain management, sputum clearance and cough efficacy, reduced dyspnoea, and improved physical fitness [12]. The aim of this study involved the evaluation of the effects of physiotherapy in patients following oncological treatment, in particular including determination of whether rehabilitation in patients resulted in improvement of spirometric indicators and decreased occurrence of respiratory disorders. The assessment of the effect of the duration of the intervention program on ventilation activity of lungs was also performed.
Material and methods
The research involved patients after breast cancer treatment qualified for outpatient physiotherapy at the Rehabilitation Unit at the Cancer Centre and Institute of Oncology in Gliwice in 2012–2013. In total 91 patients underwent rehabilitation. The characteristics of this group are summarised in Table 1.
Table 1
Selected characteristics of qualified rehabilitated patients
It can be seen in Table 1 that following the classification of malignant tumours, the prevailing tumour types were T = 2 and N = 1. A vast majority of patients had an expression of oestrogen receptors (3) and reached menopause. All women were subjected to radiation therapy, and more than half underwent concurrent chemotherapy. Patients participated in rehabilitation were on average two and a half years after the completion of radiotherapy. On average, physiotherapy took approximately three weeks and it was performed following the physiotherapy treatment. The respiratory disorders in patients were assessed based on the spirometric tests including the following air flow indicators: forced expiratory volume in one second (FEV1), vital capacity (VC), forced vital capacity (FVC), peak expiratory flow (PEF), ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC), and forced expiratory flow (FEF). The resulting material was used for statistical analysis.
Statistical analysis
Student’s t-test for dependent observations for time intervals (preceding and following rehabilitation) was applied in the study. The assessment of the examined clinical factors on ventilation indicators relied on a linear model, which determines the relation between the dependent variable Y and the set of predicting factors X in the following form: Y = b0 + b1X1 + b2X2 + … + bkXk.
In this equation b0 is an intercept, and bi represents the regression coefficients (slopes) for explanatory variables (from 1 to k). In the statistical analysis, only univariate and bivariate regressions were considered.
Results
The study involved the use of Student’s t-test to compare the results before and after rehabilitation with regard to patients subjected to breast-conserving treatment and those after mastectomy.
Based on the results reported in Table 2, statistically significant differences in means of spirometric indicators before and after rehabilitation were estimated, especially in patients who underwent mastectomy. Linear univariate models of statistically significant effects of spirometric indicators and selected clinical factors on ventilation of lungs are reported in Table 3.
Table 2
Results of Student's t-test for subgroups of patients
Table 3
Linear model of changes in lung ventilation indicators in patients without combined chemotherapy
The data in Table 3 show that the time of physiotherapy significantly contributed to an increase in FEV1% – approximately 1.8 units per day of rehabilitation. In contrast, lymph node status radically reduced the level of PEF by as much as 64 units. The statistically significant linear models of a possible effect of chemotherapy on lung ventilation indicators are given in Table 4.
Table 4
Linear univariate models of spirometric indicators in patients with concurrent chemotherapy
The results in Table 4 demonstrate the positive influence of chemotherapy on the analysed spirometric indicators before and after rehabilitation. The effect of rehabilitation on FEV1 was also estimated in a linear bivariate regression approach (Table 5).
Table 5
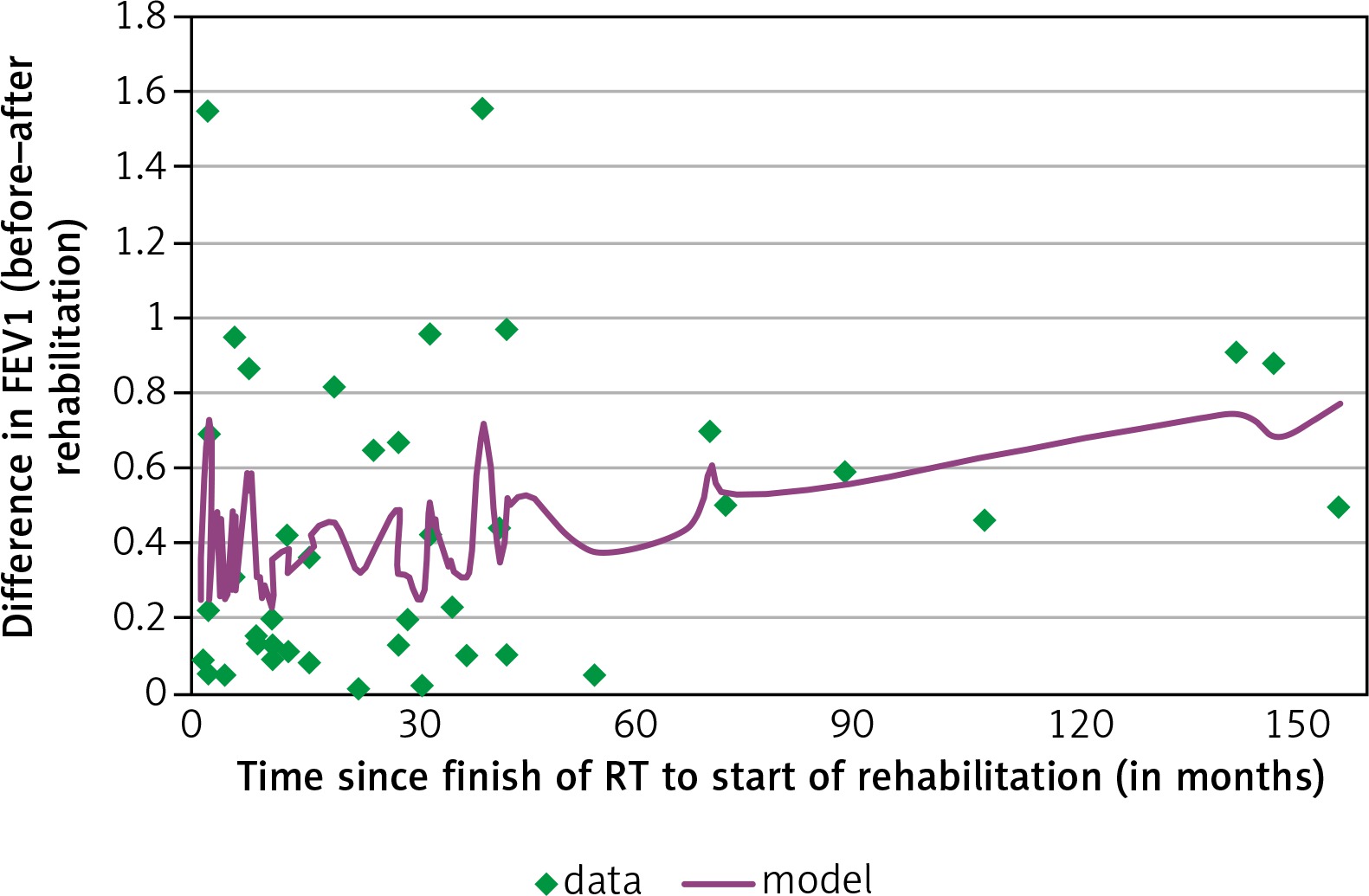
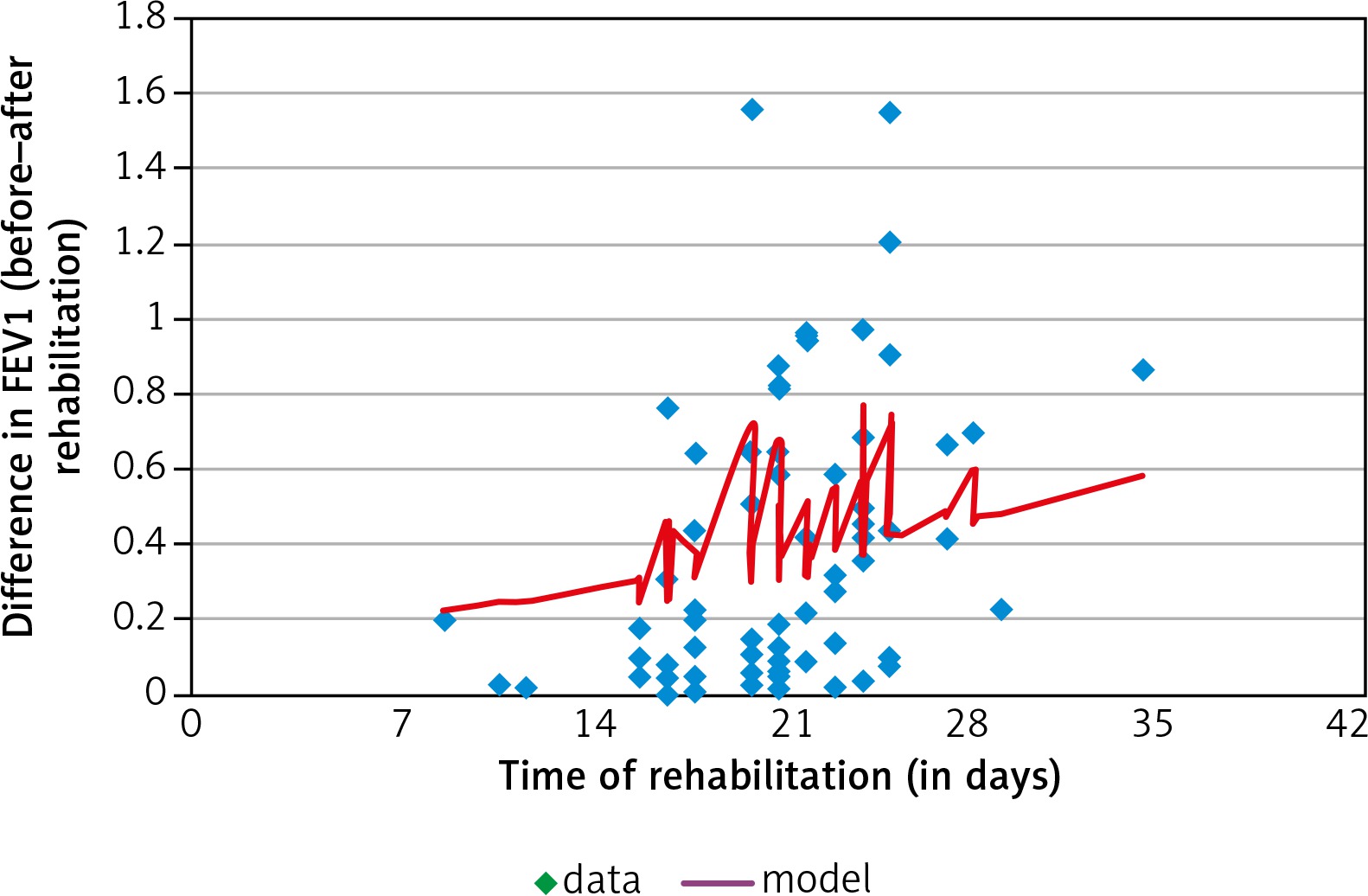
Linear bivariate regression of forced expiratory volume in one second (FEV1) on interval since oncological treatment and time of rehabilitation
The results reported in Table 5 provide evidence of a statistically significant increase in FEV1 in patients since the end of oncological treatment (approximately 0.04 l per year of the interval). What is more, a week of rehabilitation is equivalent to half a year of the non-intervention recovery of lungs in women. These results demonstrate a significant impact of the rehabilitation on FEV1. The described model is presented graphically in Figure 1 and 2.
Discussion
Based on the obtained results, a possible impact of the physiotherapeutic program on the progress in spirometric functions in breast cancer patients can be established. However, overall health development was considerably stronger in radically treated women than in women who underwent breast-conserving therapy. It seems that the better rehabilitation effect is observed in radical treatment leading to a more intensive regeneration of lungs.
The estimated correlations between differences in spirometric indicators before and after rehabilitation were mainly attributable to clinical factors, i.e. tumour size and lymph node status (Table 1). This could be explained by the intensity of the conducted radiotherapy, which in turn is related to radiation injury of lungs and their stronger recovery. Similar conclusions were reached in a study [14] on FVC, FEV1, carbon monoxide in patients suffering from irradiation after breast cancer therapy. In the cited study, the spirometric tests deteriorated relatively over the period of six months following radiotherapy and returned to a level similar to the one recorded before irradiation one year after the end of observation [14].
Contrasting observations to the present study of the effect of chemotherapy with concurrent radiotherapy on the spirometric measures were found in [15]; however, they are in accordance with [16]. The latter can be explained by stronger cell regeneration and reconstruction of lung functions in patients with the more intensive medical intervention [17].
Statistical correlations were also estimated as regards spirometric efficiency with an interval since the end of oncological treatment and time of rehabilitation. These findings can be interpreted by the natural regeneration of lungs since the end of oncological treatment. However, noteworthy is the fact that a week of rehabilitation is an equivalent to half a year of the non-intervention recovery of lungs in women. This result shows significant power of the rehabilitation on lung functions after breast cancer radiotherapy.
Based on the collected material, applied methodology, and obtained statistical results, positive physiotherapeutic effects on breast cancer patients can be established. The presented findings are not alone. Similar results were previously reported in the scientific literature worldwide [18–24]. They confirm the statement regarding the positive impact of rehabilitation on the condition of oncologically treated patients.
Conclusions
Physiotherapy leads to the improvement of lung function in patients with breast cancer following oncological treatment; progress is particularly evident in patients in more advanced cancer stages.
Clinical factors such as age of patients, body mass index, tumour size, nodal status, or menopause had no statistical effect on spirometry of lungs.
Time of physiotherapy played an important role in basic lung functions in breast cancer patients.






