
Introduction
COVID-19 is a disease caused by acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) [1]. It changes the patients’ daily routines and social communications, and the care and support they receive. Older people are challenged by themselves and others due to the need for spending more time at home, lack of physical contact with other family members, friends, and colleagues, temporary loss of job and other activities, anxiety, and fear of illness and death [2]. It is recommended that the social distancing protocol be observed to control COVID-19; but despite its positive effects, it can increase inactivity by isolating people, which can be detrimental to health [3]. Mechanical depletion of muscles due to periods of inactivity may lead to the transient exacerbation of age-related muscle changes and a reduction in the progression of skeletal muscle mass and physical strength (sarcopenia) [3, 4]. Bed rest and limb immobility, after just 5–10 days, can significantly stimulate muscle atrophy in the elderly population. Step-reduction models indicate physical inactivity caused by isolation and show that reducing daily steps (to 1500 steps per day) reduces lean foot mass in the elderly by approximately 4% within 14 days. Increased inactivity also increases mortality and functional disability in elderly people [5].
Functional disability increases the elderly’s dependence and need for care and support [6]. Successful performance of the activities of daily living (ADL) is a significant health indicator that can predict mild cognitive impairment, dementia, and mortality in the elderly population (6). After retirement age, a quarter of elderly people are unable to perform regular daily activities and 10% of them are completely paralyzed and dependent [7].
For the elderly, avoiding daily activities due to the fear of falling (FOF) while doing ADLs can increase dependence on others and social isolation while reducing physical activity and quality of life [8, 9]. The impact of these psychological factors on physical activity is likely to have devastating consequences for the health status of the elderly [10]. Although the economic costs of falling are increasing, the loss of mobility in elderly people, which leads to the loss of independence and autonomy, is the greatest loss in their remaining years of life [11]. Aging is also associated with articular cartilage damage, stiffness, and pain, which commonly affect the knee joints. Avoiding pain-related activities weakens muscles and thus limits physical activities [12]. Disabilities and problems due to knee function typically have a significant impact on people’s lives, including mobility, independence, and daily activities, and lead to a reduction in the quality of life [13].
Considering the effects of COVID-19 on all aspects of the elderly’s lives and the need for successful performance of ADLs to have an independent life and compensate for the inactivity caused by isolation and prevent its complications, elderly people should at least have positive performance in the ADLs. In order to improve ADLs, first, factors affecting ADLs should be determined and then a comprehensive plan should be provided by understanding these factors. In this regard, the question that arises is as follows: What percentage of the total variance of ADLs in the elderly can be explained by the 2 factors of FOF and knee pain and the personal performance questionnaire Western Ontario and McMaster Universities Osteoarthritis (WOMAC) that normally affect ADLs during the COVID-19 pandemic? To answer this question, this study was conducted to determine the effects of the 2 structures on ADLs using structural equation modelling/path analysis. The findings of this study could help solve some of the problems of healthy aging during the COVID-19 pandemic.
Material and methods
Study design and population
In this descriptive-analytical study, the study population included all elderly people aged 60 years and above living in the city of Izeh in the northeast of Khuzestan Province, Iran.
Sampling
The multi-stage random method was used for sampling. First, according to the map, the city was divided into 5 areas: north, south, east, west, and central. Then, to start the sampling point, one of the 5 areas was randomly selected and several centres were randomly selected from the comprehensive health centres located in that area. This process was repeated in other areas. Among the selected health centres, several were randomly selected, and the elderly people referring to them were invited to complete the questionnaire if they met the inclusion criteria. The inclusion criteria were the willingness to continue participating in the study, ability to speak, and no memory impairment. The elderly completed the questionnaires under the supervision of the researcher; for the illiterate or low-literate samples, the questionnaires were completed by the researcher.
Sample size
The sample size was determined to be at least 456 people by using the data of da Costa et al. [14], and sampling was performed in 2020. Study and estimating the correlation between the variables of FOF and movement limitation (r = 0.242) with the probability of the first-type error (α = 0.05) and 80% test power. However, considering the possibility of sample drop, 487 elderly men and women over 60 years of age were selected in Izeh city to participate in the study
n = (Z1 – α/2 + Z1-β) 2/(1/2 ln 1 + r/1-r) 2 + 3.
Measuring tools
Demographic information questionnaire: This was used to collect personal information.
Activities of daily living index: In the present study, the 6-item version of the ADLI was used. These items include personal hygiene, eating, dressing, moving, bathing, and urinary and faecal control. Each item had 3 options of dependent (score = 0), needing help (score = 1), and independent (score = 2). The overall ADL score ranged 0–12, and each participant was classified into one of the subclasses of dependent (score = 0–4), needing help (score = 5–8), or independent (score = 9–12), depending on the score he or she obtained. The validity and reliability of this questionnaire has already been confirmed [3].
Knee pain and personal performance questionnaire: This questionnaire consisted of 24 items that measured health and function in various aspects, including the severity of joint stiffness (2 questions), degree of pain (5 questions), and physical function (17 questions). Each question had 5 subscales, in which “never” or “nothing” indicated the best status and “severe” or “always” indicated the worst status. Lower scores indicated better status and less pain. The validity and reliability of this questionnaire have already been confirmed [15].
Fear of falling scale: Scoring in this questionnaire was classified into 4 levels. A higher score indicated greater fear of falling [16] The validity and reliability of this questionnaire have already been confirmed [17].
Ethical considerations
This study was approved by the Ethics Committee of Behbahan University of Medical Sciences (ID number: IR.BHN.REC.1399.059) and was conducted in accordance with the principles of the Declaration of Helsinki. Before implementing this research, the objectives of the study were explained to the participants, and they were assured about the confidentiality of their personal information. The participants were also informed that participation in this study was voluntary and they could withdraw from the study at any time.
Data analysis
In the present study, data analysis was performed in SPSS software (version 22) using descriptive and inferential statistics. The goodness of fit and predictive variance of ADL was assessed by path analysis in AMOS software. In this analysis, the relevant indicators, including the ratio of χ2 to the degree of freedom (χ2/df), goodness of fit index (GFI), comparative fit index (CFI), and root mean square error of approximation (RMSEA) were calculated. A significance level of less than 0.05 was considered in this study.
Results
The demographic characteristics of the participants are presented in Table 1. The mean (standard deviation) age of the participants was 72.04 (7.75) years. 66.3% of the participants were illiterate.
Table 1
Descriptive statistics of qualitative variables
The frequency of ADLs is shown in Table 2. According to the results, 224 people (48.8% of the participants) were independent in performing ADLs and they did not require assistance. However, 112 people (24.4% of the participants) were dependent on those around them for daily activities. Meanwhile, there were 123 people (26.8%) who needed the assistance of those around them to perform some of their daily activities.
Table 2
Frequency of activities of daily living
| Variable | Level | Frequency | Percentage |
|---|---|---|---|
| ADL (n = 459) | Dependent | 112 | 24.4 |
| Needing help | 123 | 26.8 | |
| Independent | 224 | 48.8 |
Descriptive statistics including the lowest and highest values along with the mean and standard deviation for the variables of FOF, knee pain and personal performance (WOMAC), and the ADL are reported in Table 3. The total score of the ADL index ranged 0–12, and its mean and variance were 8.05 and 3.53, respectively. According to the results of the present study, the ADL score was significantly different between men and women (p < 0.05). The mean ADL score was higher in males than in females, and their average difference was reported to be 2.1 units. But the mean of FOF for females was significantly higher than for males, by 4.8 units (p < 0.001). Also, the total score of knee pain and personal performance (WOMAC) was significantly higher for women than for men (p < 0.05). In addition, the Pearson correlation coefficient of the age variable with the ADL, FOF, and WOMAC variables was so low that its significance was rejected at the level of 0.05.
Table 3
Descriptive statistics of the studied variables
The results of path analysis of the model’s indicators showed the optimal goodness of fit for the model:
(χ2/df = 1.98, GFI = 0.97, CFI = 0.92, RMSEA = 0.063, p < 0.001).
The results of path analysis also showed that the fitted model was able to explain 64% of the total variance of the ADL (Fig. 1, Table 4).
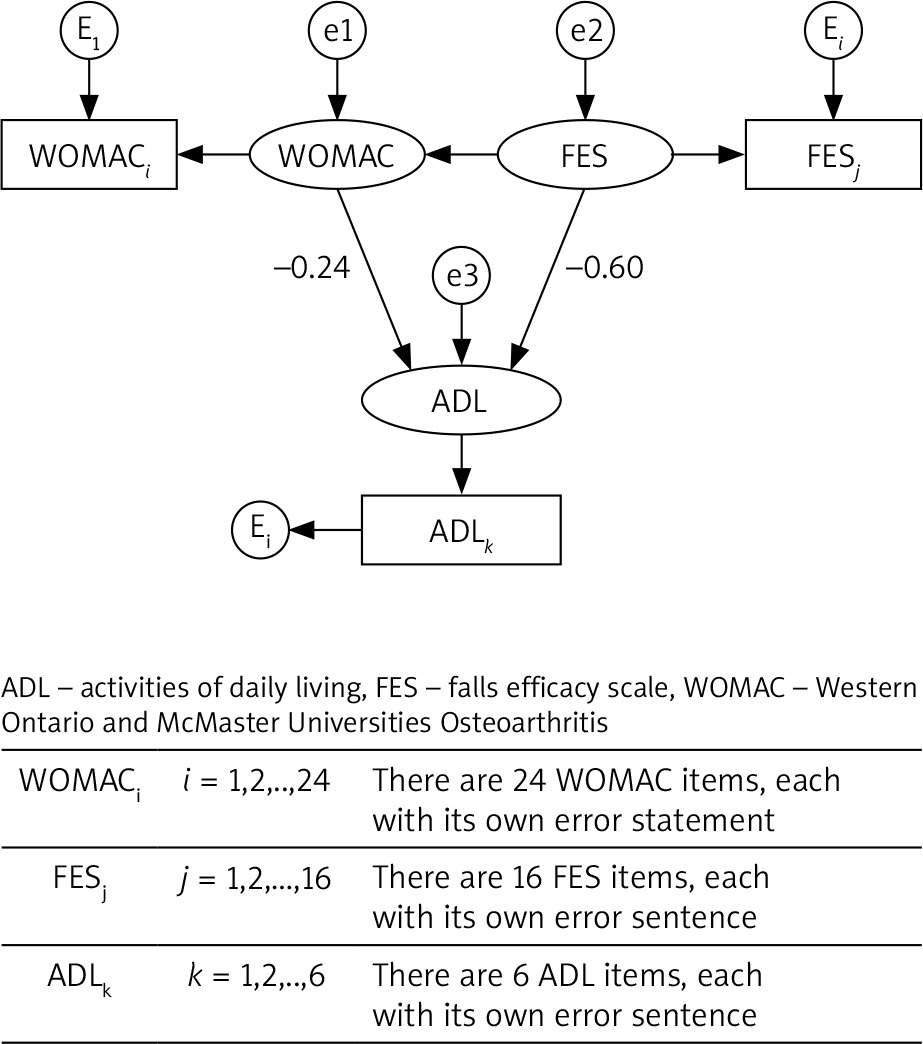
Table 4
Indicators of path analysis goodness of fit
| Indicator | The obtained value |
|---|---|
| χ2/df | 0.98 |
| GFI | 0.97 |
| CFI | 0.92 |
| NFI | 0.99 |
| IFI | 0.93 |
| RMSEA | 0.063 |
| PNFI | 0.65 |
| AIC | 733.2 |
| Percentage of variance coverage | 64 |
The results of path analysis showed that:
The structure of FOF had a direct, negative, and significant effect on ADLs. This means that the higher the FOF, the more an elderly person needs the help of others to perform ADLs, so that for one unit increase in the FOF, 0.65 units of independence in performing ADLs was reduced.
The FOF structure also had an indirect effect on ADLs by affecting the WOMAC structure, so that for every unit increase in the fear of falls efficacy scale (FES-1), 81% was added to WOMAC. This means that increased FOF would increase WOMAC and decrease independence or increase dependence in the ADL.
Discussion
Along with aging, maintaining independence in daily activities and continuing to live an active life are the most important factors in improving the health of elderly people, which leads to satisfaction, higher self-esteem, and lower physical dependence [18]. Considering the effects of COVID-19 on the daily life of elderly people, assessing the ADL status is one of the best ways to evaluate the functional independence of elderly people [19]. Sudden decline in activity levels, as is likely to be caused by social isolation, is a particular concern in older people, who are typically more sedentary than their younger counterparts and prone to weakness, sarcopaenia, and chronic diseases [13]. Independence in activities and lack of reliance on others are essential during the COVID-19 pandemic. To improve the daily activities of elderly people, we need to identify factors affecting ADLs, and design and implement effective interventions to improve it. This study aimed to determine factors affecting ADLs among elderly people during the COVID-19 pandemic. To achieve this goal, the structures of FOF, WOMAC index, and ADLs were investigated using structural equation modelling/path analysis.
In the present study, 24.4% of the participants were dependent. The mean score of the ADLs in the elderly samples was 8.05. Increasing the dependence percentage among elderly people during the COVID-19 pandemic and decreasing the mean score of ADLs compared to normal conditions [7] led to more reliance of elderly people on care and support. Meanwhile, COVID-19 has changed the care and support programs that older people receive. Elderly people have also been challenged due to observing social distancing, spending more time at home, and not having physical contact with other family members, friends, and colleagues. Undoubtedly, infection prevention is important, but supporting older adults in activities that provide them with a sense of purpose in life can contribute to their overall health, including mental health [2]. Thus, an increase in the percentage of dependent elders, on the one hand, and the changes that the COVID-19 pandemic has made to the lives of the elderly, on the other hand, have created a complex situation for educational policymakers and planners in designing special and appropriate interventions, particularly in this rapidly evolving situation. It seems that during the COVID-19 pandemic, the best way to promote ADLs in the elderly is to pay attention to the effective personal factors. The empowering self-management model can be used as a suitable model to improve the quality of life of the elderly because it is a native model and its main purpose is to empower individuals. In fact, in this model, the process of self-participation is necessary, which can compensate for the loss of physical strength by increasing the mental and spiritual strength of the elderly [20]. The empowering self-management model emphasizes the role of individuals in gaining power through maintaining independence and lack of reliance, awareness of the changes in using one’s own abilities effectively, active problem-solving attitudes through adaptation, life satisfaction and playing a useful role in life, and finally, the ability to control the problems caused by aging [21]. Therefore, the empowering self-management model can be a suitable framework for educational interventions to increase the functional independence of the elderly during the COVID-19 pandemic. Considering the psychological factors such as factors that inhibit and facilitate the ADLs of the elderly during the COVID-19 pandemic is potentially important because it will lead to more effective and appropriate training strategies. For example, inhibitory factors such as lack of motivation to carry out ADLs can be managed by facilitating factors such as sending incentive text messages and mail. Qualitative studies on the factors that inhibit and facilitate elderly people’s ADLs are recommended to explore hidden aspects of this issue.
In the present study, the 2 constructs of FOF and WOMAC predicted 64% of the variance of elderly people’s ADLs. The findings of the present study also showed that each of the structures was significantly correlated to elderly people’s ADLs. In this regard, the structure of FOF had a direct, negative, and significant effect on the ADLs. FOF also had an indirect effect on ADLs by affecting the WOMAC structure. The findings of the present study are consistent with the results of many investigations, including Hornyak et al. [22], Suzuki et al. [23], Fucahori et al. [24], and Choi et al. [25]. In the study by Brustio et al., FOF had a direct and indirect effect on ADLs [26]. Another study concluded that restriction in ADLs by about 46–56% of elderly people was affected by FOF [24].
The fear of falling scale measures the elderly’s self-confidence in performing a series of daily tasks without falling by assessing the falling self-efficacy [27]. Bandura’s theory of self-efficacy predicts that the ability to perform tasks depends on physical ability and mental self-efficacy [28]. Therefore, a relationship exists between the falling self-efficacy and deteriorating the ADL performance [27]. Self-efficacy affects the level of effort made by a person to do a task and the levels of his/her performance [29]. Therefore, the educational interventions are suggested that are based on strategies that enhance self-efficacy such as considering step-by-step objectives, behavioural contract (a formal contract with specific objectives and rewards), control and support (feedback through self-control and memo writing), control of negative emotional responses, and providing verbal incentives and support to enhance the self-efficacy related to falls in the elderly. Physical intervention programs may reduce FOF that can contribute to psychological conditions such as depression and affect the quality of life of older people. Thus, providing integrated health care activities is critical for the elderly to engage in both psychological and physical well-being [23].
To improve knee function and reduce the effects of pain, morning dryness, joint stiffness, and difficulty in performing daily activities, it is recommended that this population during the current pandemic are provided with appropriate exercise programs through television, online films, and distance health programs. Recent evidence suggests that a multi-component exercise regimen focusing on flexibility, strength, balance, and endurance can effectively improve balance, mobility, and physical function, as well as reduce the incidence of falls and fall-related injuries in the elderly. The Otago Exercise Program (OEP) covers all the above aspects and is designed for the elderly over 65 years of age. Most studies have reported OEP as an effective fall prevention strategy that helps balance function and reduces the FOF [30]. It is hoped that the Iranian form of this program will be considered by planners and policy makers for the elderly Iranian population.
Factors that may be involved in knee function include high body mass index and obesity, continuous cross-legged sitting, low consumption of dairy products and milk, and vitamin D deficiency [31]. These factors can be adjusted through lifestyle-changing educational interventions. To manage knee pain, using complementary and herbal medicine methods is recommended under the supervision of relevant experts; elderly people have a higher tendency to use complementary and traditional medicine treatments because they are cheaper and more accessible, and have fewer complications [32].
As with other studies, the present study also had several limitations. Using self-reporting method in assessing the ADL of the elderly was one of these limitations. However, although it was done with the full supervision of the researcher and colleagues, it showed the need to know and use more objective methods in future studies.
Conclusions
The results of the present study show that the number of independent elderly people is low. The results also demonstrate that 64% of the total variance of the ADL in the studied elderly can be explained by 2 structures of FOF and WOMAC during the COVID-19 pandemic. Thus, these 2 structures can be used in designing educational interventions that aim to improve the ADLs of elderly people during the current pandemic. These findings confirm that FOF is a health problem that deserves more attention. Therefore, a multi-component program containing exercise and psychological strategies through television, online videos, and distance health programs is recommended for this population during the COVID pandemic. We hope designing and implementing educational interventions based on these determinants will reduce the problems caused by inadequate daily activities and correct them in the elderly population during the COVID-19 pandemic.








