Introduction
Surgical treatment of neoplastic lung metastases is a big therapeutic problem, both at the stage of qualifying for the procedure and the surgical technique itself, as well as the tactics of managing subsequent disease relapses. The most questionable aspect is determining which factors influence the prolongation of survivals. Knowing that only a few percent of patients with secondary neoplastic disease can undergo surgery, we usually lose sight of the remaining group of patients. We study survival only in selected patients and therefore we cannot objectively compare the results of surgical treatment to other methods. At the same time, it should be remembered that only some patients can undergo non-surgical oncological treatment due to the histological type of the tumor, the stage of the disease and, finally, the presence or absence comorbidities. These factors often exclude the possibility of any causal treatment. Another problem that reduces the value of research is the need to perform a retrospective evaluation. In the available literature, there are practically no publications taking into account the group of patients who, despite meeting the criteria, did not undergo surgical treatment. Some authors believe that the benefit of surgical treatment is neither immediate nor unquestionable [1–3]. On the other hand, it is easier to make a decision about surgical treatment than to look for arguments against its futility. Another issue that makes it difficult to obtain correct conclusions is the heterogeneity of the studied groups. It should be remembered that metastases are closely related to the properties of the primary tumor. Each of them has different spreading characteristics. It is known that the invasion can take place via the lymphatic or bloodstream route. This is related to the histological diversity of the primary tumor as well as its location, which further complicates obtaining objective results. In this case, for research purposes, it seems right to distinguish the group of neoplasms of epithelial origin without the necessity to define the starting point of the disease. Undoubtedly, sarcomas, germinal tumors and melanomas constitute a separate group. The creation of a homogeneous study group should allow for approximate determination of the predictive factors influencing the achieved therapeutic results. This, however, is usually not possible due to the insufficient database available in one treatment center. It seems that the published multicenter data are burdened with a greater error related to, for example, various criteria for qualifying for surgical treatment (despite generally accepted standards) They differ in terms of the surgical technique itself and postoperative management both at the early stage after surgery and the adopted criteria for qualifying for subsequent metastasectomy, which it is necessary in about 40–50% of patients. On the other hand, the conclusions published by Pastorino years ago based on a multicenter database are generally consistent with single-center publications. On the basis of our research to date, doubts arise mainly about the answer to the question of whether and why more operations result in longer survival. This does not seem to be logical. On the other hand, however, we can assume that patients who underwent only one or two operations lived shorter due to the greater progression of the disease, and thus were disqualified from subsequent surgical procedures. It should also be remembered that survival is influenced by other factors, such as the histological type of the tumor, the number and size of lesions in the lungs, and finally the presence or absence of metastases to the lymph nodes. Nor can we expect a permanent cure for a patient with secondary proliferative disease. The goal of surgical treatment is to extend the periods of remission by implementing standards of treatment that can only be defined on the basis of retrospective studies of large groups of patients.
Aim
The aim of the study is to find out what factors influence the effectiveness of surgical treatment. The dependencies affecting the radicality of the procedure, which is one of the main prognostic factors, will be analyzed. Moreover, an attempt was made to investigate the relationships related to the occurrence of relapse after resection. In the previous article, Surgical Treatment of Neoplastic Lung Metastases, there were some uncertainties that require further research. They concerned longer survival of patients who underwent multiple metastasectomy, as well as longer survival of patients with recurrence after resection, and the lack of a relationship between metastases to the chest lymph nodes and survival. Currently, an attempt has been made to clarify these doubts.
Material and methods
Due to the fact that some patients were operated initially outside the Institute of Tuberculosis and Lung Diseases in Warsaw, the data on treatment were not always complete. A group of 577 patients with secondary neoplastic disease involving the lungs was analyzed. At the same time, the available detailed data related to 1,009 operations. Only the group of patients for which the data were complete was analyzed. The factors influencing the lack of radicality during resection of metastatic lesions from the lungs and the relationships related to the occurrence of metastases to the chest lymph nodes were analyzed. In addition, the impact of the radical nature of the procedure on relapse after resection and the importance of unilateral and bilateral operations on disease relapse were examined. In order to objectify the obtained results in terms of the impact of disease relapse on survival, 2 homogeneous groups of patients were separated. The first group included patients operated on twice and having initially metastatic changes in both lungs. They were operated on at least 3 weeks apart from the first surgery. In justified cases, the surgery was postponed until it was fully functional after the first resection. The second group included patients who were also operated on twice. Initially, they had lesions in one lung. Another operation was performed due to a relapse in the lung that had been operated on or in the opposite one. Patients with metastatic changes in the lymph nodes were also thoroughly analyzed. In the previous work, in statistical studies of the entire data set, no statistically significant differences in survival were found for patients with or without lymph node involvement. At the same time, it has not been unequivocally demonstrated so far that their removal in a secondary neoplastic disease prolongs survival. At that time, when analyzing the group of patients with lymph node metastases, the survival from the first (or only) metastasectomy to the date of death was assessed. Survival from the day of surgery, during which lymph node metastases were found, has now been studied. Such an assumption objectifies the obtained results. It allows for a real study of the survival of a group of patients with or without metastases to the lymph nodes.
Statistical analysis
The data were presented in two ways. The analysis of the factors influencing the lack of radicalism and the occurrence of lymph node metastases was performed in conjunction with surgery as the unit for analysis. The experiences were examined in relation to the patient as the analyzed record. Factors influencing radicalism and the incidence of lymph node metastases were investigated using descriptive statistics and statistical significance assessed using χ2 test estimates. Patient survival was analyzed using Kaplan-Meier estimates and the log-rank test. The analysis was performed using the R statistical software version 4.0.2 (R Core Team 2020). R: Statistical computing language and environment. R. Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/).
Results
The database was created on the basis of retrospective studies. It contains data from 1009 operations performed on 577 patients. Information about the radical nature of the operation was available in 943 records. Information on metastasis was available in 936 records. The number of missing data is given in each table. The missing information was completely accidental and unrelated to the patient’s condition. The factors influencing the lack of radicality in resection of metastatic lesions to the lungs were investigated. The following findings were made:
The percentage of non-radical procedures increases statistically significantly with the number of metastases.
If there were lymph node metastases, the percentage of non-radical operations was significantly higher; the difference was statistically significant.
The percentage of non-radical operations was the highest in the age group under 50; it decreased significantly with the patient’s age.
Statistically significant relationships were observed between the primary starting point of the proliferative disease and the fact of performing a non-radical metastasectomy. Their highest percentage was found at the primary location of the disease in the liver, followed by the location (other) where the pancreas, larynx and thyroid were the dominant primary lesions. The next location was the osteoarticular system/muscles, another breast, and the reproductive organ. The kidney and the large intestine were in further places. It should be emphasized that the above-mentioned calculations were obtained on the basis of the total number of operations in all examined patients.
There was also a correlation between the histological type of the tumor and the radical nature of the metastasectomy. The most frequent lack of radicality was in sarcomas, then melanomas, squamous cell carcinoma, clear cell carcinoma, and adenocarcinoma.
In subsequent operations in the same patient, the percentage of non-radical operations increased statistically significantly (Table I).
Table I
Factors influencing the lack of radicalism of metastasectomy where the unit of calculation for statistical purposes is the operation (not the patient)
[i] 1The percentage of non-radical operations increases statistically significantly with the number of metastases. 2There were no statistically significant differences between the maximum tumor size and the percentage of non-radical operations. However, the largest number of non-radical operations were performed in situations where the largest lesion in the pulmonary parenchyma was over 3 cm in diameter. 3If there were lymph node metastases, the percentage of non-radical operations was significantly higher; the difference was statistically significant. 4Men underwent non-radical surgery slightly more often, but the difference was not statistically significant. 5The percentage of non-radical operations was the highest in the age group up to 50 years; it decreased statistically significantly with the patient’s age. 6There was no statistically significant relationship between the percentage of non-radical operations and one/two-sided operations. 7There were statistically significant differences between the location of the primary tumor and the fact of performing a non-radical operation. Their highest percentage was observed for liver operations, followed by the location (other) where the pancreas, larynx and thyroid were the dominant primary focus. The next location was the osteoarticular system/muscles, another breast, and the reproductive organ. The kidney and the large intestine were in further places. It should be emphasized that the above-mentioned calculations were obtained based on the total number of operations in all examined patients. 8There was also a relationship between the histological type of the tumor and the radicalism of the metastasectomy. Here it was found that the most frequent lack of radicalism was in sarcomas, followed by melanomas, squamous cell carcinomas, clear cell carcinomas, and adenocarcinomas. 9In subsequent operations on the same patient, the percentage of non-radical operations increases statistically significantly.
The relationships between the occurrence of relapse after resection and the radicality of the procedure were analyzed successively. When analyzing the operated cases, it was not completely determined whether the recurrence occurred in the non-radical operated site or in a different location of the pulmonary parenchyma. Such methodology resulted from objective difficulties in establishing this information in a large number of cases. Nine hundred and forty-three procedures performed in 562 patients were analyzed. No radicality was found during 106 operations performed in 53 patients. Accordingly, radicality was achieved during 837 operations performed in 509 patients. Percentage of relapse after resection or no relapse was compared between the study groups. There was no statistical significance of the recurrence of the disease depending on the radicality of the procedure (Table II). However, no conclusion should be drawn that the completeness of the procedure did not affect the survival. Patients undergoing such surgery live shorter lives, which was confirmed in our previous studies. The mean survival time was 47 months in the case of radical surgery versus 28 months in the absence of radical surgery. With a complete operation, the 3- and 5-year survival rates were 60% and 43%, respectively, compared to 44% and 26% with an incomplete operation. An attempt was also made to determine the effect of the presence of metastases in one or both lungs on relapse. There was a higher incidence of relapses in bilateral procedures of approximately 20%. In cases of unilateral operations, recurrences were found in 10% of cases. These results were statistically significant (Table III).
Table II
Relapse after resection depending on the radicalism of the operation
Table III
Recurrence after resection depending on the presence of unilateral or bilateral metastases
Factors influencing the occurrence of lymph node metastases in the thoracic region were also investigated. The number of metastases in the lung parenchyma, their size, the radical nature of the operation, recurrence after resection, sex, age, the number of operations performed, unilateral or bilateral surgery, the location of the primary tumor, and the histological type of the tumor were taken into account, and the next surgery was followed by the most frequent metastatic lesions in lymph nodes. The following results were found to be statistically significant:
Lymph node metastases are more common during non-radical surgery.
Lymph node metastases were most often found in the 50–60 age group.
Lymph node metastases were found more frequently during unilateral surgery. At the same time, it should be emphasized that some of these patients had metastases on the other side, but were not qualified for further surgical treatment.
A statistically significant association was observed between the location of the primary tumor focus and the occurrence of metastases to the lymph nodes. They were most often found in the case of testicular neoplasms, followed by breast and kidney tumors.
The histological type also statistically significantly differentiated the occurrence of lymph node metastases. They most often occurred in germinal tumors, then in epithelial carcinomas classified as other epithelial groups (65 cases including pancreatic, laryngeal, reproductive organ, breast, integumentary, thyroid, salivary gland, prostate and bladder cancer), then in renal cancer (Table IV).
Discussion
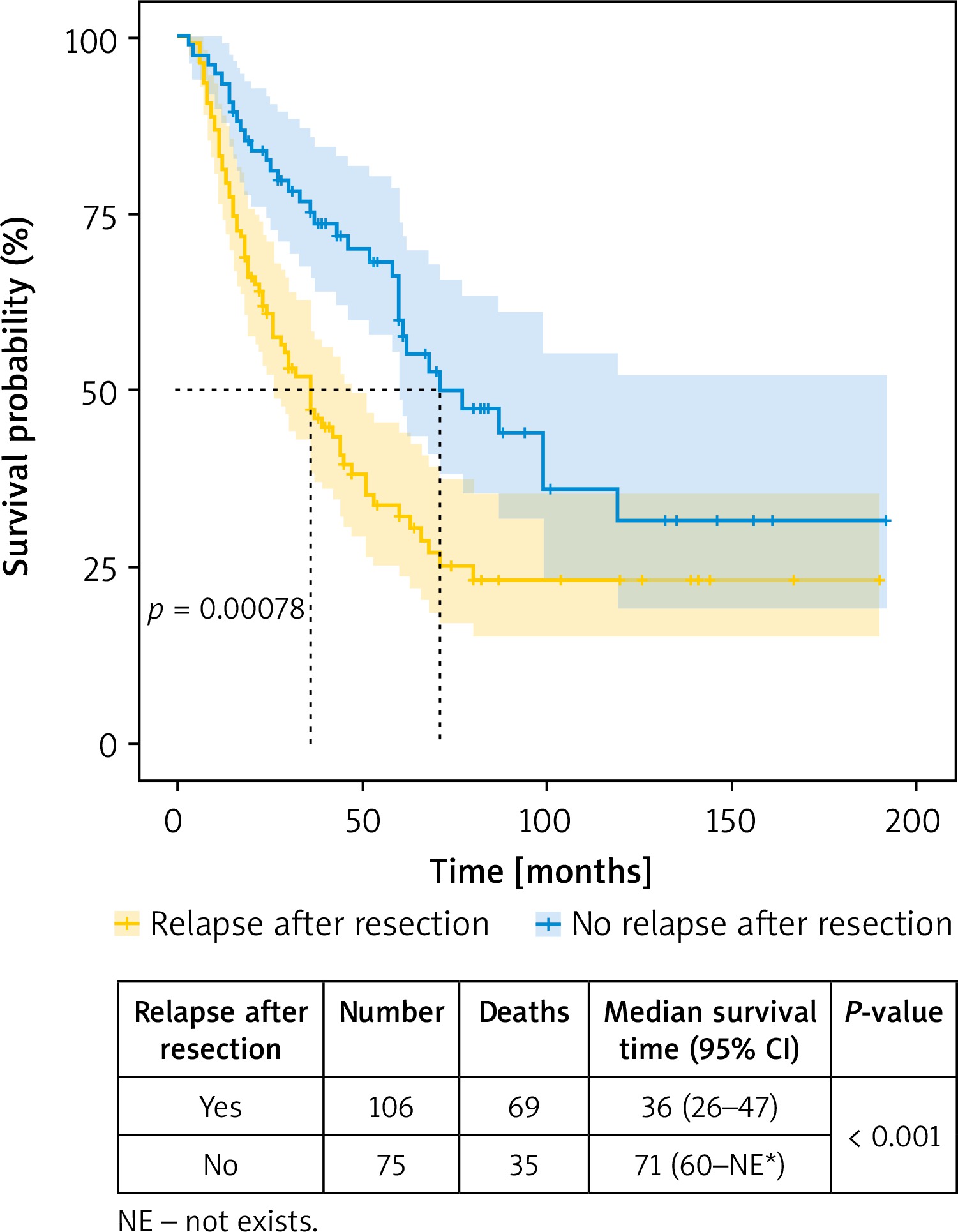
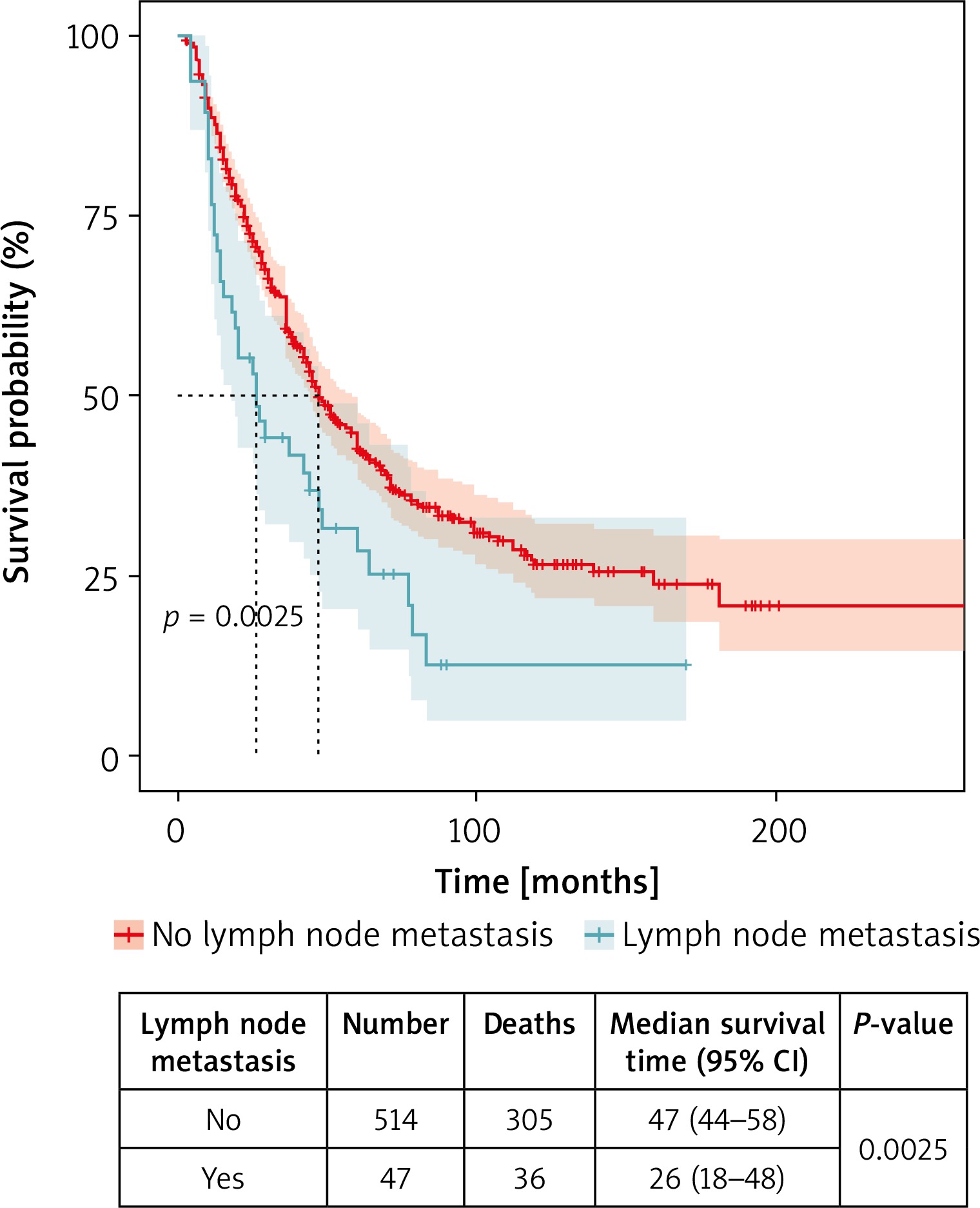
Subsequent metastasectomy obviously correlates with relapses after resection. According to various researchers, multiple lung resections enable longer survival. Welter et al. concluded that repeated resections of lung metastases (a study on metastasis of colorectal cancer) were safe and provided longer survival [4]. The authors reported 5-year survival in 53.8% of cases with repeated resection. The median survival was 47 months in patients after a single metastasectomy; with more operations it increased to 72 months. Kandioler et al. studied a group of 330 patients who had undergone at least two metastasectomies. These authors suggest that patients who are permanently disease-free at the original site, but who have recurrent resectable metastatic lung disease, are likely to benefit from surgery a second, third, or even fourth time [3]. According to the International Registry of Lung Metastases (IRLM), after the second resection, 44% of patients survive for 5 years, and 29% for 10 years. 34% and 25% of patients who have undergone only one resection survive for 5 and 10 years, respectively. In our studies to date, the results achieved also indicate longer survival of patients operated on several occasions. After the first resection for 5 years, 38% survive; after the second, 46%; and with more procedures (three or more), 48% (Table V). It is impossible to objectively assess whether multiple operations to remove lung metastases prolong survival, because it is difficult to find a comparative group [3, 4]. It is also obvious that patients qualified for subsequent treatments must meet oncological criteria that give a chance for radical surgery. In order to objectify the obtained results, in terms of the impact of the relapse of the proliferative process on survival, an attempt was made to create two groups of patients that could be compared with each other. The survival of patients who underwent only two metastasectomies was examined. Longer survival was observed in the group of patients without relapse – with initial metastases in both lungs (median survival 71 months vs. 36 months). These results were statistically significant (Figure 1). Another issue that requires more attention is the question of how important a predictor of secondary proliferative disease is the presence or lack of metastasis to regional lymph nodes. It is obvious that tumors spreading through the lymphatic route more often metastasize to nodes; the primary location of the tumor and its histological type are of similar importance. Therefore, the mere fact of the presence of metastases in the thoracic nodes does not necessarily indicate the same degree of progression of the proliferative disease for different types and primary tumor locations. For example, the frequency of nodal metastases is low in colorectal adenocarcinoma (9%) and sarcoma (6.6%), average in head and neck and urinary tract cancers (12–18%) and high in melanoma, uterine cancers, ovaries, breast cancer and germ cell tumors (33%, 38%, 54% and 100%, respectively) [5–7]. Lymphadenectomy performed in secondary proliferative disease does not prolong survival. However, it allows for a more accurate determination of the stage of the disease and thus gives a chance for systemic treatment. According to the majority of researchers, there is a statistically significant association of survival with metastases to the lymph nodes. The invasion of cancer cells into the lymphatic vessels results in a greater likelihood of the formation of further metastases, relapses of the disease and, therefore, shorter survival times. However, it has also been reported that the group of patients with the presence of nodal metastases has no worse prognosis than patients without their involvement [8–10]. In the previous work, in statistical studies of the entire data set, no statistically significant differences in survival were found for patients with or without lymph node involvement. However, it should be remembered that the analysis covered a selected group of patients who initially qualified for surgical treatment. When qualified for metastasectomy in imaging studies (CT and possibly PET-CT), they did not have significantly enlarged nodes and/or increased FDG uptake in them. It seems reasonable to determine at which surgery (multiple operations were performed in about 40% of cases) metastatic changes were found in the nodes. This may answer why we did not observe previously statistically significant differences in survival in patients with and without lymph node metastases. If node involvement occurs during the first operation, the prognosis is worse. However, the situation is different when, after a long treatment period and multiple operations, metastases appear, which prevent further therapy. Previously, when analyzing the group of patients with and without metastatic changes in nodes, the moment of their involvement in the disease process was not taken into account. Survival from the day of surgery where nodal metastases were found has now been investigated. It was found that the median survival is longer in patients without nodal metastases compared to those with nodal involvement (47 months vs. 26 months) (Figure 2). An additional element that was examined was the determination of the extent of resection at which metastases in the lymph nodes were most often detected. According to some authors, they were found more often in anatomical resections in relation to marginal or wedge resections (23% to 12%) [11–14]. Our studies have not confirmed this opinion. A total of 728 wedge resections were performed, revealing lymph node metastases in 38 cases. 195 anatomical resections were also performed, confirming nodal involvement in 12 patients. These values were 6.15% and 5.21%, respectively. Summarizing the obtained results, longer survival was found in patients without disease recurrence (median survival 71 months vs. 36 months). At the same time, the occurrence of disease recurrence was not statistically significantly dependent on the radicality of the procedure. The reason for such results of the current research is the fact that patients undergoing non-radical surgery live shorter lives, which was confirmed in previous studies. Therefore, we do not observe any relapse that could be treated surgically. Relapses were found to be more frequent in patients undergoing bilateral metastasectomy. It was also found that the median survival is longer in patients without nodal metastases compared to those with nodal involvement (47 months vs. 26 months). Moreover, it was established what factors influence the radicality of the operation in secondary proliferative disease with lung involvement. These are mainly the number of metastatic lesions, coexistence of metastases in the lymph nodes, the location of the primary tumor, the histological type of the tumor and the number of operations. In turn, the occurrence of metastases to the chest lymph nodes is influenced by non-radical metastasectomies, the age range (50–60 years), the location of the primary focus and the histological type. Moreover, more frequent occurrence of metastases in the thoracic lymph nodes was found in unilateral surgery. However, no conclusions should be drawn from this that could suggest that unilateral involvement of the lymph nodes affects the prognosis. Patients with metastatic changes in nodes at the first operation were disqualified from further metastasectomy and in statistical studies were included in the group of patients undergoing single/unilateral surgery. This in turn influenced the obtained results.
Table IV
Factors influencing the occurrence of lymph node metastases where the unit of calculation for statistical purposes is the operation (not the patient)
[i] 1There is no statistically significant correlation between the number of lung metastases and the occurrence of lymph node metastases. 2There is no statistically significant relationship between the size of the metastasis and the occurrence of lymph node metastases. 3Lymph node metastases are statistically significantly more common in non-radical surgery. 4There is no significant relationship between the fact of relapse after resection and the presence of lymph node metastases (calculation unit – patient). 5There is no significant relationship between the fact of recurrence after resection and the presence of lymph node metastases (calculation unit – operation). 6There is no statistically significant relationship between the patient’s sex and the occurrence of lymph node metastases. 7Statistically significant differences in the frequency of lymph node metastases depending on age were observed. The highest percentage was in the age group 50–60, the lowest in the group over 60 years old. 8The percentage of lymph node metastases was lower in the group of bilaterally operated patients. 9The incidence of lymph node metastases differs statistically significantly depending on the type of initial surgery – the highest in the case of testicular, breast and kidney surgery. 10The incidence of lymph node metastases differs statistically significantly depending on the histology – they often occur in the case of germinal tumors, epithelial carcinomas (other group), and kidney cancer. 11There is no statistically significant relationship between the occurrence of lymph node metastases and subsequent metastasectomies.
Table V
Survival by the number of operations