








Introduction
The lifetime occurrence of groin hernia is 27–43% in men and 3–6% in women [1]. The condition can be repaired only by surgical procedures involving open inguinal hernia repair (OIHR) and laparoscopic inguinal hernia repair (LIHR). OIHR is one of the chronic postoperative inguinal pain (CPIP) risk factors. Overall, the incidence of clinically significant chronic pain ranges from 10% to 12% [2]. The chronic pain rate for laparoscopic techniques is estimated at approximately 6% (range: 1–16%), which is significantly lower than the rate for tension-free open hernia repair technique of approximately 18% (range 1–75%) [2]. Minimally invasive techniques have allowed LIHR to offer the advantages of rapid recovery and less pain. An indirect inguinal hernia (IIH) is the most common inguinal hernia (IH) characterized by tissue protrusion through the internal inguinal ring (IIR). Transabdominal preperitoneal (TAPP) repair can treat IIH. For large IIH, it is of interest whether autologous tissue reconstruction can be used to cover the IIR in laparoscopic repair, whether there is no significant increase in CPIP after laparoscopic suture, whether it is feasible, and may have some impact on vascular injury. A retrospective analysis was conducted by the medical team of the Department of Hernia Surgery at the Shanghai Public Health Clinical Centre on patients who had undergone TAPP. The IIR was covered with the lateral umbilical fold (LUF) and repaired with a self-gripping mesh. The LUF contains the inferior epigastric vessels (deep epigastric vessels – DEV). We comprehensively studied its feasibility, safety, postoperative pain, scrotal serum swelling, and recurrence. The study was approved by the Shanghai Ethical Committee.
Aim
The aim of the study is to evaluate the efficacy and safety of covering IIR with the LUF combined with patch repair in laparoscopic IIH repair.
Material and methods
General data
A total of 195 IH patients treated by TAPP at the Department of General Surgery, Shanghai Public Health Clinical Centre between September 2019 and March 2021 were retrospectively analyzed. Among them, 76 patients were classified according to the European Hernia Society (EHS) groin hernia classification as having type M2 and M3 DIH [3]. The remaining 119 patients were assigned to primary type L2 and L3 IIH according to the EHS groin hernia classification. The data collected consist of patient demographics such as age, sex, body mass index (BMI) and comorbidities, and perioperative data such as the type of hernia as per the European Hernia Society (EHS) classification [4]. All patients who underwent LIHR, aged between 18 and 85 years old, presenting with primary IH, with an IH inclusive of L2 or L3 IIH (measured intra-operatively according to the EHS groin hernia classification system) were included. All patients received anti-coagulant prophylaxis after the TAPP operation. The patient signed an informed consent form. Patients aged 25 to 84 years in whom the LUF was used to cover the IIR were included in the study. The patients and their families were informed before the surgery. In total, 112 males and 7 females were enrolled and graded as type I–II based on the American Association of Anesthesiologists (ASA). There were 16 patients with hypertension, 10 with diabetes, and 18 with chronic obstructive pulmonary disease (COPD) before the surgery. Nine patients had the acquired immune deficiency syndrome (AIDS), and 21 patients had a scrotal hernia. Patients classified as having L2 and L3 IIH according to the EHS groin hernia classification were enrolled in the study. Exclusion criteria were: 1) patients with severe abnormal functions of heart, lungs, liver, or kidneys, 2) patients with severe intraperitoneal infection, 3) patients with psychiatric disorders who could not cooperate during the perioperative period, 4) patients who were classified as having M2 and M3 DIH according to the EHS groin hernia classification. No significant differences between the two groups in terms of age, gender, BMI, complications, and other clinical data (p > 0.05) were observed, as shown in Table I.
Table I
Comparison of general clinical data between the two groups before the surgery
Methods
Group I: The preperitoneal separated plane was used at the routine method. The IIR was covered with the LUF (suturing with a needle holder in laparoscopy with the right hand). The starting point suture of the left IIH is slightly different from that of the right one. It is first better to suture the LUF on the left side, and the transversalis fascia (TA) on the right side first:
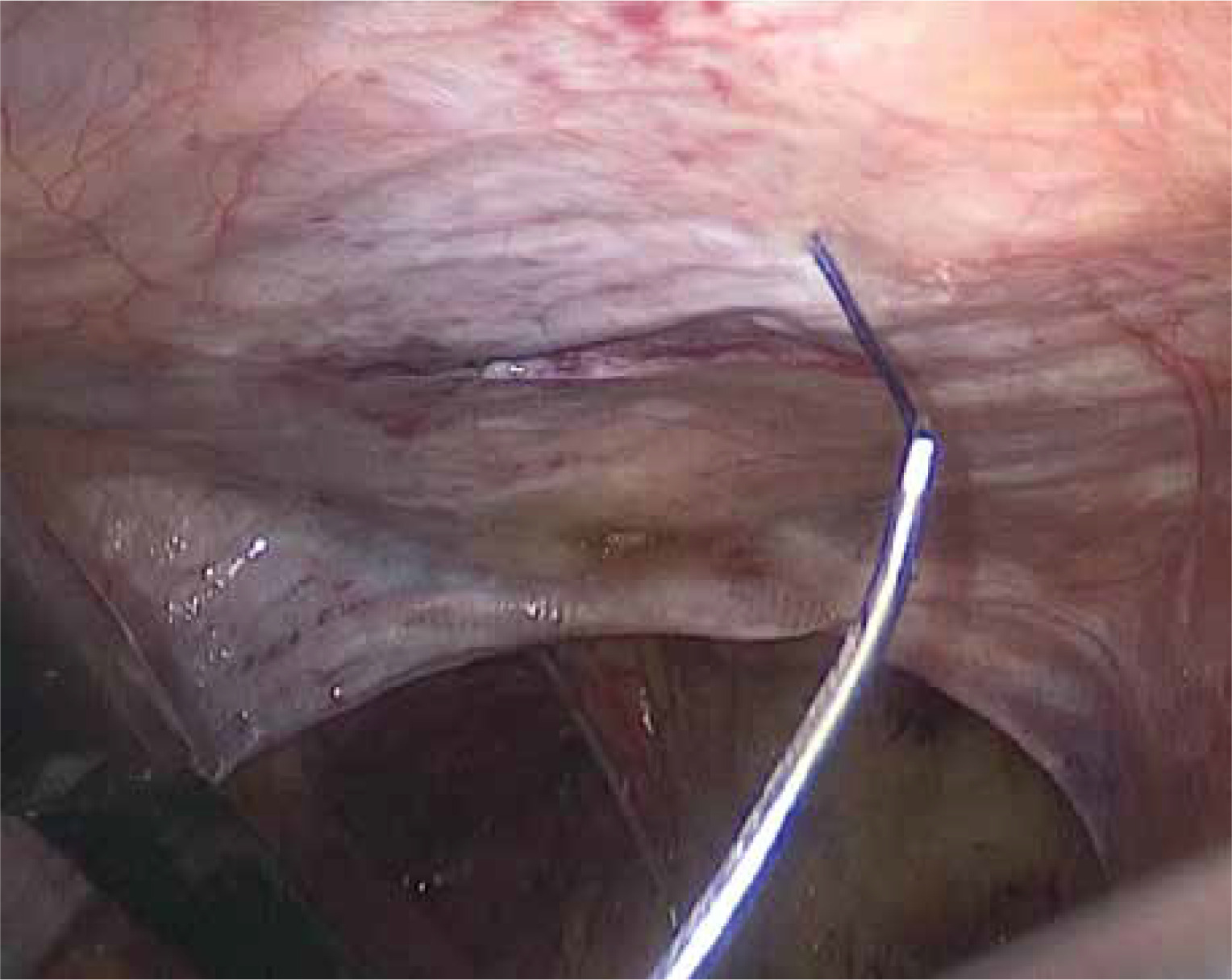
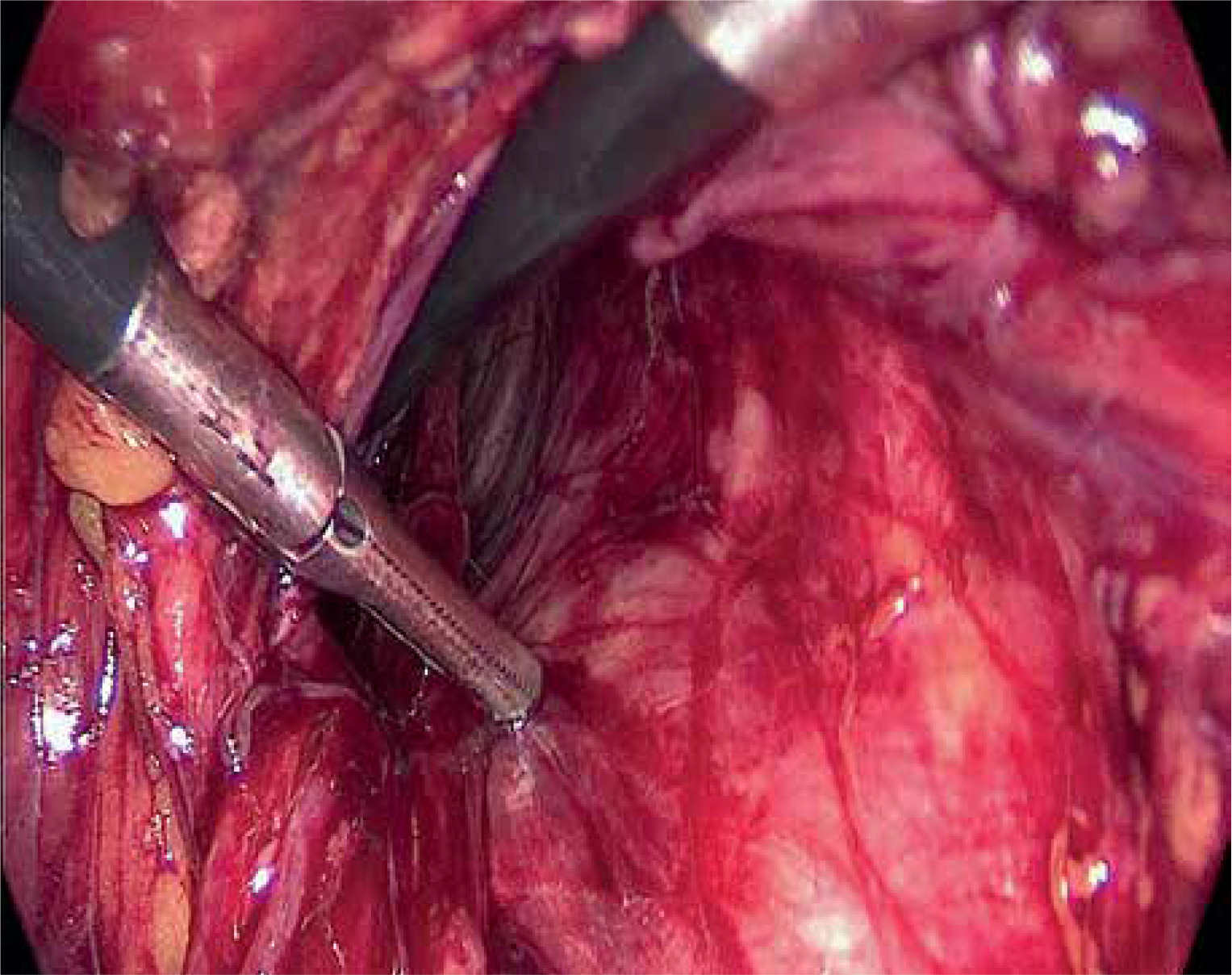
The left IIH: a 1/0 vicryl absorbable suture needle was used to adjust the needle’s curvature before entering the abdomen to reduce the curvature of the needle as much as possible. The absorbable suture needle pricking point was selected by pressing the abdominal wall. The needle was inserted from the inferior abdominal cavity, and the needle penetrated the abdominal cavity, as shown in Photo 1 below.
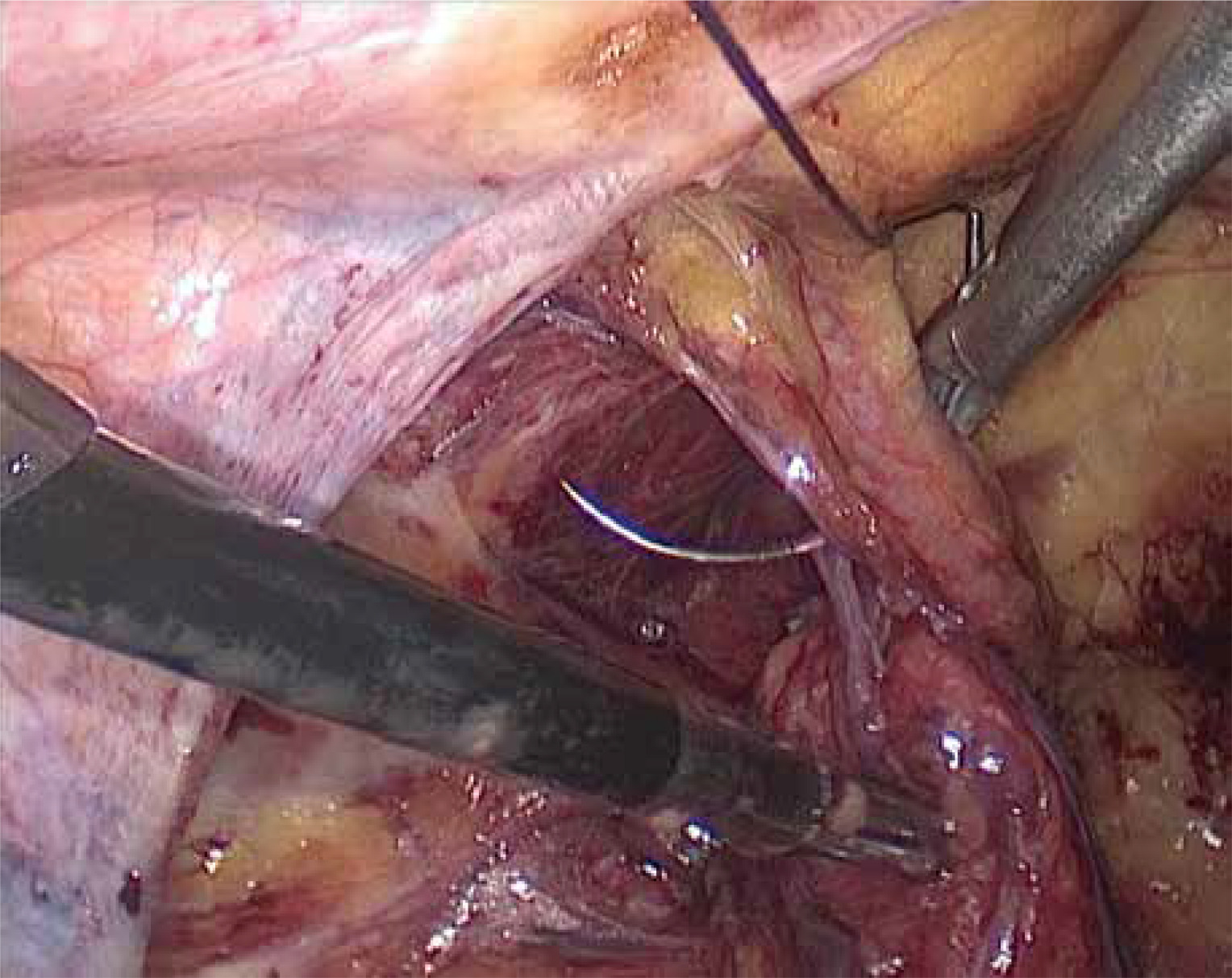
Suture of the first knot: the anterior superior part of the LUF was sutured, avoiding suturing the DEV, as shown in Photo 2.
Photo 2
The anterior superior part of the subabdominal vessels (over the flat IIR opening) was sutured
The needle holder was used to rotate the suture downward. The suture contained with the TA above the IIR. The needle was drawn from the anterior superior part of the DEV (about 0.5 cm from the early needle).
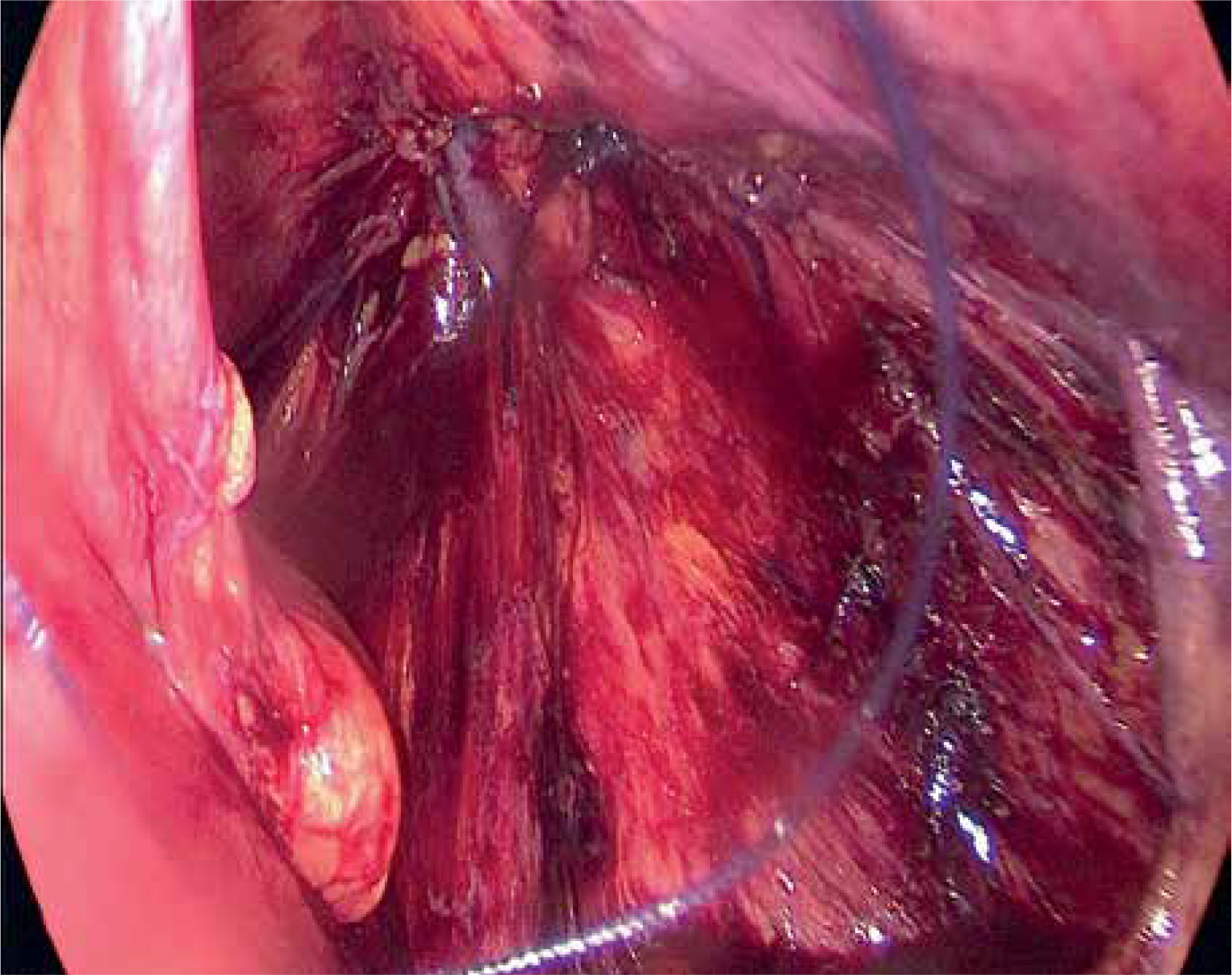
The suture was tied with a surgical knot, which can easily slip out of place. An exact and reliable knot is needed. The image after the first suture is shown in Photo 3. Suture of the second knot: The fascia of the LUF was sutured behind the DEV.
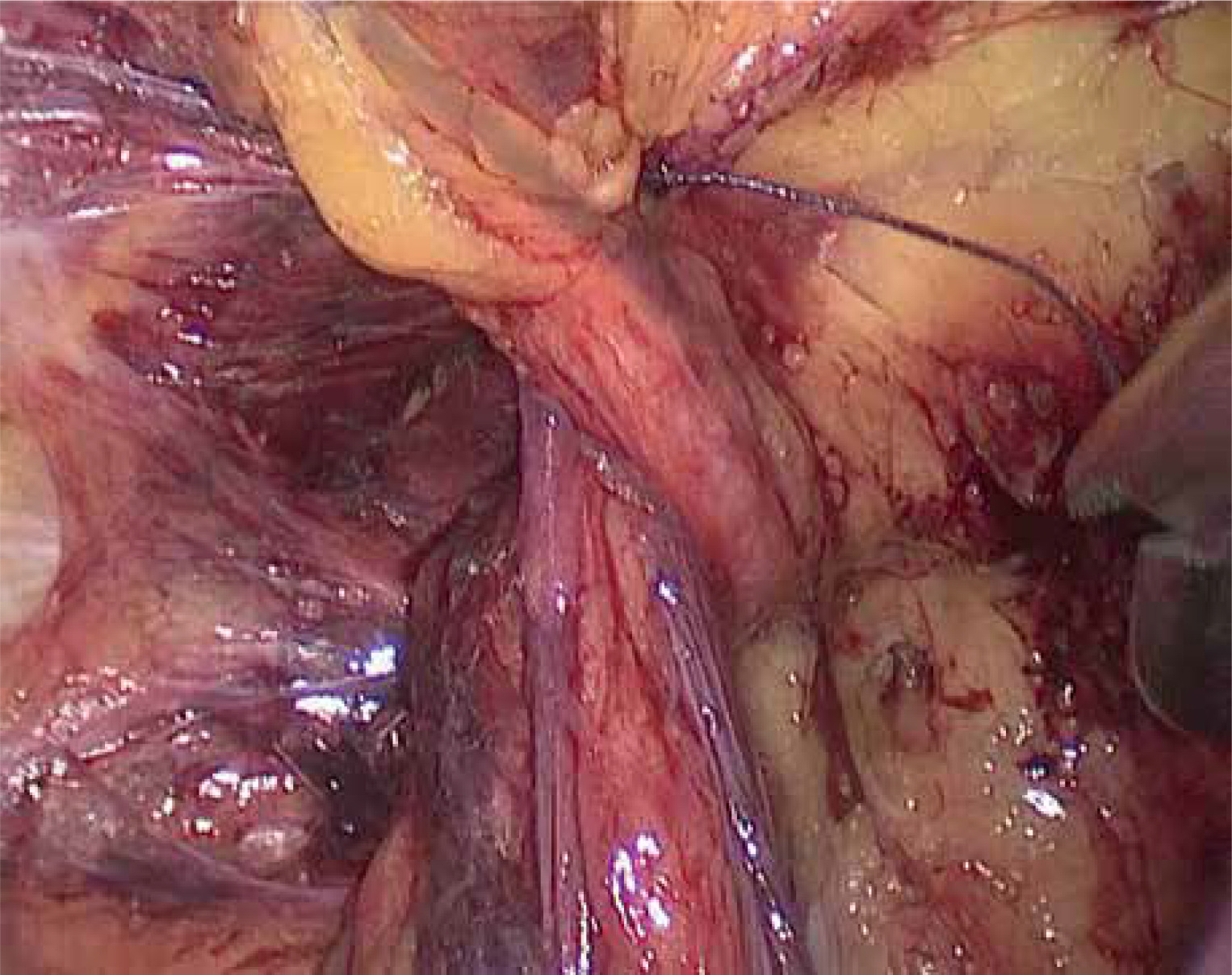
The TA below the outer part of the IIR was sutured. During suturing, the left-handed forceps lifted the TA tissue properly to ensure that the needle was sutured with a needle in the right hand. This needle was as close to the lateral abdominal TA tissue as possible and away from the triangle of pain (TOP). The second knot was tied and fixed.
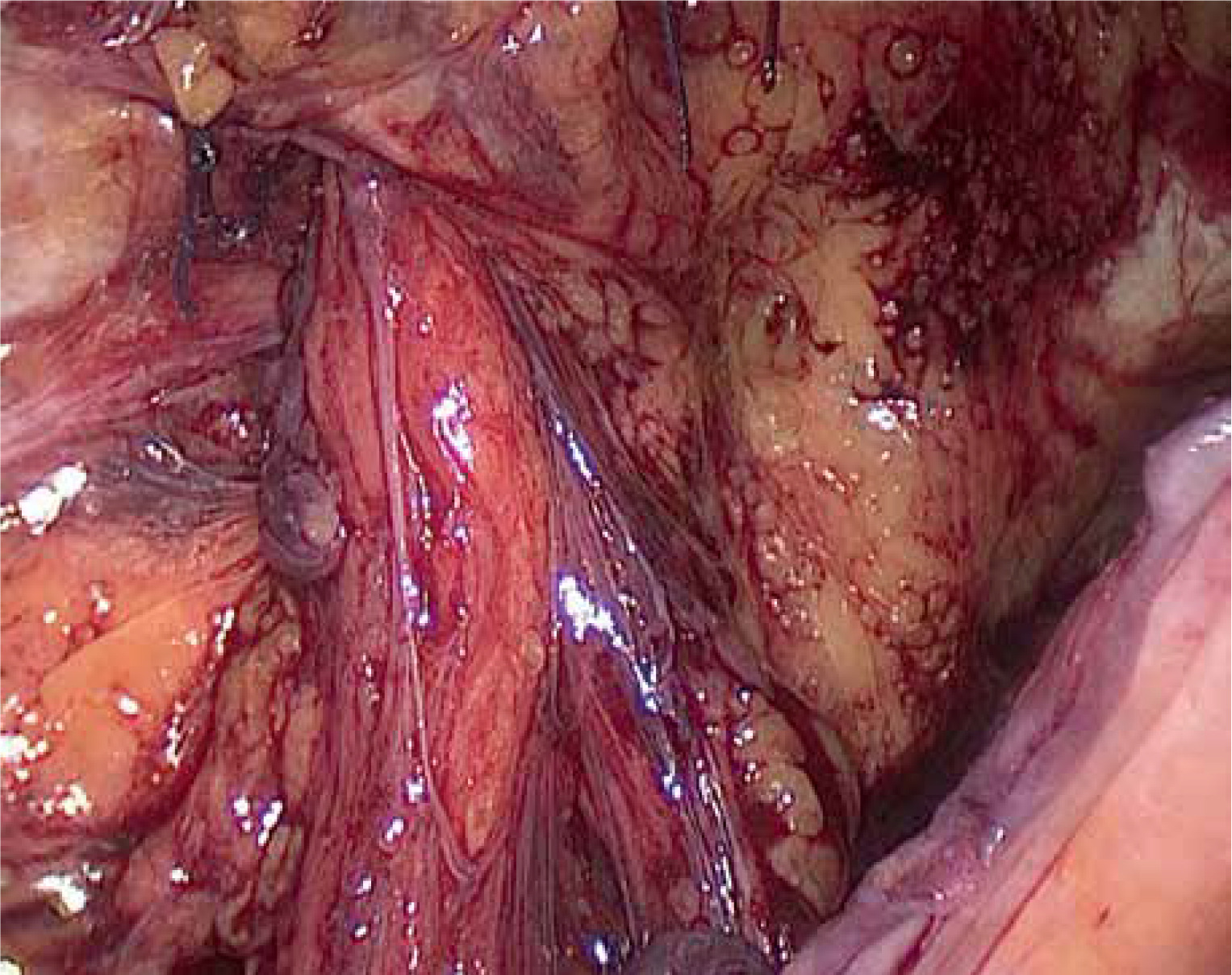
The image after two sutures is shown in Photo 4; the IIR was covered. The right IIH: The right IIH was stitched through the TA, and afterward, the LUF was sutured to cover the IIR. The image of the right LUF covering the IIR is shown in Photos 5 and 6.
After the LUF was covered, the four corners of the self-gripping mesh (ProGrip Self-Gripping Polyester Mesh, Covidien, Trevoux, PP1509, 15 × 9 cm, China) were cut appropriately and placed into the anterior peritoneal plane, with the patch covering at least 3 cm of the edge of the hernia ring, completely spread and fixed. The peritoneum was closed.
Group II, the IIR was not covered with the LUF but only with a self-gripping mesh.
Observation indicators
The patients were followed up for at least 3 months. The surgery time, postoperative hospital stay, postoperative cost, and complications such as trocar infection, surgical site infection (SSI), pulmonary infection, surgery area hematoma, urinary retention, trocar bleeding, seroma, DEV injury, and postoperative pain in the surgery area were recorded.
Statistical analysis
SPSS22.0 software was used for analyses of data. The data are expressed as mean ± standard deviation (x ± s). The t-test was conducted, and the repeated measurement data were analyzed by analysis of variance (ANOVA). The data were compared using the χ2 test. Fisher’s exact probability test was used for small probability events. P < 0.05 indicated a significant difference.
Results
All patients recovered quickly after the surgery and were discharged. The patients were followed up for more than 3 months. No significant difference in the postoperative hospital stay between the two groups (p > 0.05) was observed. However, a significant difference in surgery time and hospitalization cost (p < 0.05) was found. In terms of complications, no incision infection, SSI, pulmonary infection, surgical area hematoma, or trocar bleeding in the two groups was present, and there were no significant differences in urinary retention between the two groups (p > 0.05). In addition, no significant difference in postoperative pain was observed between the two groups (p > 0.05). One case of hernia recurrence occurred in group II, as shown in Table II.
Table II
Comparison of intraoperative and postoperative covering data between the two groups
Discussion
Partial treatment of IIH and whole treatment of the myopectineal orifice (MPO)
IH can only be cured by surgery [5]. The treatment of IH with open and minimally invasive procedures has reached a high standard over the past 30 years. However, there is still a need for further improvement in inguinal hernia repair, particularly in reducing postoperative seroma, chronic pain, and recurrence. The basic knowledge of IH anatomy, mesh biomechanics, and surgeon’s experience are essential in hernia repairs in reducing those problems. The anatomy of the inguinal area has necessitated a renewed understanding of inguinal anatomy. The IH anatomy reveals an anatomic defect in the inguinal region. Modern hernia surgery believes that the weakness of the MPO and the defect of the TA are the critical causes of all IH [6, 7]. The MPO is referred to potential sites for IH (indirect inguinal, direct inguinal, and femoral) as the development of laparoscopic techniques and preperitoneal approaches to surgical hernia repair. Mastering the important anatomical structure of the MPO is crucial to the success of the operation.
LIHR is among tensionless hernia repairs one of the most popular methods nowadays [8]. It is also one of the commonly used methods for IIH. It is reasonable. It has the advantages of fast recovery and a lower recurrence rate than the traditional operation. Its advantages are beyond doubt, and it has become one of the important ways of preperitoneal approaches of hernia repair. LIHR includes totally extraperitoneal repair (TEP) and TAPP techniques. TAPP can more easily detect the existence of occult hernia and repair it at the same time.
IH includes direct inguinal hernia (DIH), IIH and femoral hernia (FH). The IIH is the most common type of IH. The area, lateral to the DEV, which is called the lateral triangle of the groin [9], including the IIR, is protected solely by the internal oblique muscle and TF.
IH can be repaired by suture or mesh-based techniques, using open surgery or laparoscopy, and IIH can also be repaired by suture or mesh-based techniques by open surgery or laparoscopy. OIHR is still the most common surgical method at present. Suture-based open operations are performed through the classic anterior approach, and the open techniques are those of Lichtenstein, Bassini, and Shouldice because it is easy to suture and knot. LIHR is always done through a posterior approach and with a mesh. Prosthetic mesh reinforcement is now a routine step in the operative management of IH, having been shown to significantly reduce the risk of recurrence [10]. Suture repair is rarely seen in LIHR because it is difficult to suture and knot in laparoscopy.
Mesh size may have a greater impact on recurrence. A small mesh has been shown to be one of the independent risk factors for recurrence compared with a large one [11]. A significant trend toward reduced recurrence rates with increasing mesh size was noted (a “large” mesh was most often 10 × 15 cm in size). 3,017 patients who underwent TAPP showed a 5% recurrence rate using an 11 × 6 cm mesh in 325 repairs and a 0.16% recurrence rate using an 15 × 10 cm mesh [12]. It should be emphasized that dissection of the preperitoneal plane has to be adequate for the size of mesh to ensure that the mesh lies flat against the abdominal wall. it seems reasonable to suggest that the mesh should overlap the hernia defect by at least 3 cm in all directions. For an IIH with large IIR, the only way to prevent recurrence of the hernia is to expand the hernia patch. The IIR is L2 or L3 IIH, and the recurrence is reduced by continuously increasing the patch diameter. With the gradual maturity of endoscopic suture technology, can we narrow the IIR using self-tissues to reduce hernia recurrence?
The use of TA as a self-tissue during surgery acts as a barrier against hernia recurrence and plays a crucial role in IH repair. Jignesh Gandhi strongly feels that native body tissue is superior to any foreign prosthetic to achieve closure of the posterior fascia [13]. The Shouldice procedure, using crossed sutures to reconstruct the TA, has achieved the purpose of reducing hernia recurrence. The 2009 European Guidelines opined that the Shouldice was the best non-mesh technique [14]. Recently, LIHR has gained popularity among patients owing to its minimal invasiveness. However, multiple clinical issues need to be addressed in LIHR. First, laparoscopic repair requires an adequate free area dissection to cover the entire preperitoneal plane. A patch of 10 × 15 cm in size is generally selected. We have found that an L2 and L3 IIH with a large defect can be repaired by self-tissue to reduce the IIR. A smaller patch (9 × 15 cm) is subsequently used to reduce recurrence and the area of the preperitoneal plane. Although TA reconstruction produces good outcomes in open Shouldice surgery, it is difficult to achieve the desired results using TA as an auto-tissue repair in laparoscopy. Huynh reported 24 cases of robotic IH with iliopubic tract repair (ITR) achieved by suturing the TA arch to the iliopubic fascia [15]. It was one of the self-tissue repairs in IH. The LUF covering the IIR is our key solution for IIHs at this time. In fact, the suture of the DIH is relatively simple, and it will be discussed in the future. We met a patient with postoperative recurrence in group II, but the patient had no symptoms, and the patient temporarily refused the operation. There is no recurrence in group I. However, the total number of cases is very small, and the results need further observation.
IIH is the most common IH. The IIR was covered by the LUF when the IIH occurred. In fact, it focuses on the treatment of IIH and it doesnot focus on the treatment of DIH, it is part of treatment of IIH and not whole treatment of DIH and IIH. The patch repair covering the MPO emphasizes the whole treatment of the defect, and the part-whole treatments achieve harmony and unity. It is the unity of the part and the whole.
Feasibility of LUF coverage and the risk of DIH damage
The LUF was used to cover the IIR, which can be sutured accurately and knotted reliably to achieve a good effect of covering the IIR. The LUF covering the IIR has its advantages:
Close to the IIR: the LUF is located on the inside of the IIR, close to the IIR.
Wide range of motion: after the LUF moves laterally, the range of motion becomes wide, the tension is not high, enabling one to flip to the lateral IIR after surgical suturing.
The covering effect after the suture is good: the proper selection of the two-needle suture of the LUF can cover more than 90% of the IIR.
Few nerves in the LUF were observed with less postoperative pain: when the LUF was covered and the second needle was sutured under the outer part, the suture needle was away from the inside of the IIR to avoid the TOP. No significant difference in pain between group I and group II was recorded.
The DIH in the LUF is vascular tissue. Vascular tissue, especially arteries, such as the middle layer of arteries, has a large number of elastic fibrous tissue. Elastic fibers provide recoil to tissues that undergo repeated stretch [16], which may prevent hernia.
We recorded 1 case with recurrence in group II, caused by the large IIR and patch movement. However, there is a need for follow-up with many patients for further comparison due to the small sample size in the current study.
The Henle’s ligament investing fascia of the lateral margin of the rectus tendon is thickened, and it has been observed in 46% of cases in Condon’s dissection [17]. Henle’s ligament were sutured to TA of the external IIR which can enhance the coverage of the IIR.
The LUF covers the IIR, and if the effect is optimal, it can be applied in:
Strangulated IIH repair without a patch.
Repair of recurrent IIH in children.
Repair of small IIH without defect.
For strangulated IIH with intestinal necrosis, the use of a patch is still associated with a certain risk of infection.
The LUF covering the IIR has the following disadvantages:
The DEV, which include the inferior epigastric artery (IEA) and inferior epigastric vein (IEV), are easy to suture. During laparoscopic suturing, the artery was sutured once, and the vein was sutured once. In these cases, after vascular injury has occurred, the DEV were closed directly by suture and knotting to reduce the possibility of bleeding. During the operation, the main DEV was ligated near the external iliac artery, and the artery and vein were ligated together. No obvious bleeding was found. Considering that the vascular pressure decreased significantly after the main artery ligation, no rectus muscle ischemia was found after 0.5 h of observation. It is considered that there are usually anastomoses with the superior epigastric vessels and the obturator vessels, and internal iliac vessels [18]. After the operation, the pad on the operation side was covered, and the abdominal band was slightly pressurized and bandaged. No bleeding was found after the operation.
The straining and deformation of the DEV and vein after the suturing of the LUF may lead to venous thrombosis. Therefore, attention needs to be paid to early bed activity to prevent deep vein thrombosis. Subcutaneous injection of heparin requires the patient’s signature and consent.
Due to difficulty in suturing and tying the knot, the surgical time was significantly increased in group I compared with group II. The surgical time in the first 3 cases was significantly increased by 50 min. In addition, the cost of surgery was high. However, knot tying becomes challenging and frustrating when performed laparoscopically. Laparoscopic vessel ligation and suturing opened up a new horizon for laparoscopy [19].
ProGrip relieves pain and possibly laparoscopic suture technique increases pain
ProGrip mesh is a self-gripping composite hernia mesh. A monofilament polyethylene terephthalate mesh (PET) is lightweight and covered by a resorbable layer of polylactide acid (PLA) microgrips. With the pore size 1.8 × 1.8 mm (macroporous), it can reduce postoperative pain [20–22]. LIHR using the TAPP with implantation of the ProGrip laparoscopic mesh is a fast, effective and reliable method, which according to the results reduces the occurrence of CPIP with simultaneously a low recurrence rate [11]. The mesh can reduce the postoperative glue fixation and not use nail gun fixation. This can reduce the CPIP caused by interference factors such as fixation.
A common complication after LIHR is CPIP, which affects a patient’s quality of life postoperatively, with an incidence of about 2% to 20%. CPIP is regarded as the cause of postoperative pain in the OIHR. The LUF covering the IIR has some advantages because it is far from the pain triangle. In contrast to iliopubic tract repair (IPT), it was kept away from the ilioinguinal nerve in the second suture. Thus, the postoperative pain does not increase; however, it is difficult to suture. Whether the suture site is separated again due to the use of absorbable suture needs to be discussed. In addition, its reliability remains to be verified. In the future, only the LUF may be used to cover the IIR in the occult hernia, and no patch can be placed to verify the reliability of repair further.
1/0 Vicryl absorbable suture needle: The use of long-term absorbable suture in laparoscopic percutaneous extraperitoneal closure of the internal ring for pediatric inguinal hernia is associated with no suture knot reaction but a higher hernia recurrence rate. Tran N recommend non-absorbable monofilament such as Prolene in laparoscopic percutaneous extraperitoneal closure of the internal ring for inguinal hernia in children because of its low rate of both recurrence and suture knot reaction [23]. In addition, vicryl absorbable suture is soft and easy to knot during the operation. That is why we chose it.
The LUF covering the IIR is more emphasized in local treatment of IIH. We may also meet some challenges including injury of vessels, hemorrhage and even thrombosis and nerve suturing. We can only pursue the advantages and try to avoid the disadvantages. LUF may be an ideal material for self-tissue reconstruction and should be further studied and applied in IIH repair in the future. Whether the operation method of covering the IIR can reduce hernia recurrence still needs a lot of data for further study.
Conclusions
Covering the IIR with the LUF requires knowledge of the anatomy of the anterior abdominal wall and the ability to dissect the transversus abdominis plane by laparoscopy. Furthermore, since the suture technique takes a long time, it is extremely important to pay attention to all the nuances and details when using the suture techniques to perform this reconstruction, which is very ergonomic for the surgeon. The LUF can be used in IIH to cover the IIR and is a feasible approach. The LUF covering the IIR has no significant difference in pain.