







Introduction
Endoscopic submucosal dissection (ESD) has been well developed as a therapeutic method for en-bloc resection of superficial gastrointestinal neoplasms without lymph node metastasis. However, colorectal ESD is more time-consuming and technique-challenging due to bowel peristalsis, variable gravity, fold anatomy, frequent fibrosis of the submucosal layer, difficult scope maneuverability and unstable platform with loop formation, and thinness of the muscularis propria [1].
Since 2016 the underwater ESD (UESD) technique has been reported to make ESD easier and safer [2, 3]. The current UESD method involves aspirating all the CO2 gas and changing the patient’s posture to place the lesion at the lower side of gravity to allow for saline solution accumulation around the lesion, which seems troublesome under the condition of endotracheal intubation. To avoid the trouble of repeatedly altering the patient’s body positions according to the gravity direction of the lesion during UESD [2, 3], a novel technique of colorectal ESD using the gas-alternating-water infusion method [4] (GAW-ESD), with or without internal traction assistance, depending on the level of exposure of the submucosal space, has been improved and introduced in our endoscopic center for treating large heavy colorectal tumors (≥ 3 cm in size).
Aim
Approved by Fujian Cancer Hospital Institutional Review Board (IRB), here we first report this novel technique of colorectal GAW-ESD with or without the assistance of one-matching-many repositionable clips attached to one rubber band internal traction (GAW-ESD with/without internal traction) based on our experience of 8 cases.
Material and methods
Patients
This study included 8 consecutive patients with large heavy colorectal tumors (≥ 3 cm in size) who received GAW-ESD with/without internal traction between December 2020 and July 2021. Contraindications included suspicious signs of submucosal deep invasiveness or lymph node metastasis. Each patient signed informed consent before colorectal GAW-ESD. The study was approved by Fujian Cancer Hospital IRB (Application of water-assisted colonoscopy. No. K2020-018-01).
GAW-ESD outcomes, including operative times, post-operative hospital days, number of clips used for internal traction, and complications, were evaluated.
Endoscopic technique
The procedure was carried out using a Dual Knife Q. A video endoscope allowing water jet function (GIF-Q260J/PCF-Q260JI, Olympus, Tokyo, Japan) fitted with a disposable tip attachment (D-201-11804; Olympus, Tokyo, Japan) was used. All the 8 patients were kept in the left lateral position regardless of the direction of gravity of the lesion. The detailed steps were as follows (Case #6 underwent GAW-ESD without internal traction as seen in Video 1, Case #2 underwent GAW-ESD with internal traction as seen in Photo 1 and Figure 1):
Figure 1
Schema of GAW-ESD with internal traction-assistance. A – The colorectal lumen was instilled with normal saline with no need to remove all the CO2 gas, maintaining the existence of a boundary line between CO2 gas and water. B – V-shaped submucosal dissection below the liquid surface. C – Internal traction using two repositionable clips attached to one rubber band. D – The third clip was used. E – The above-water part of V-shaped submucosal dissection. F – Resected specimen
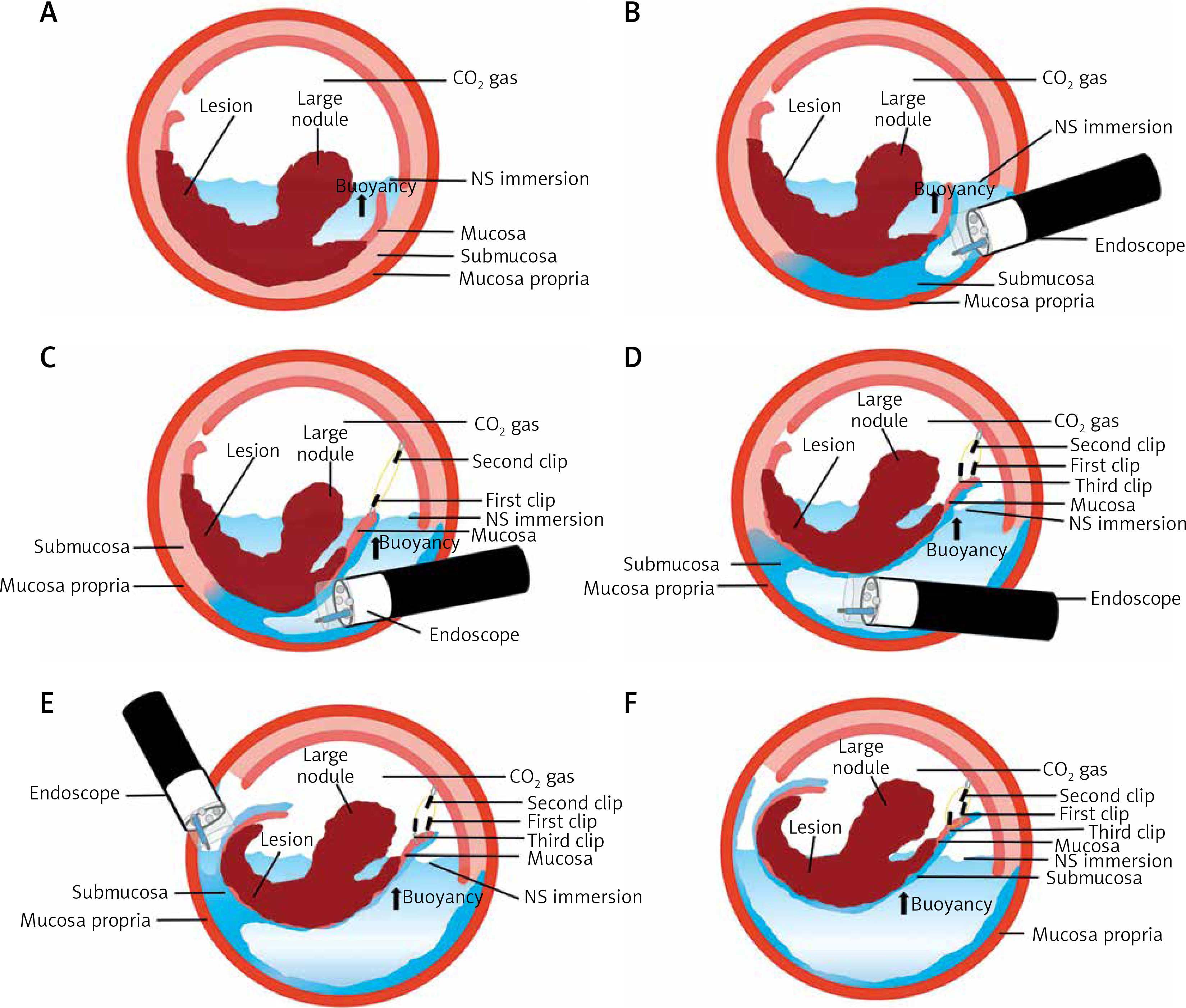
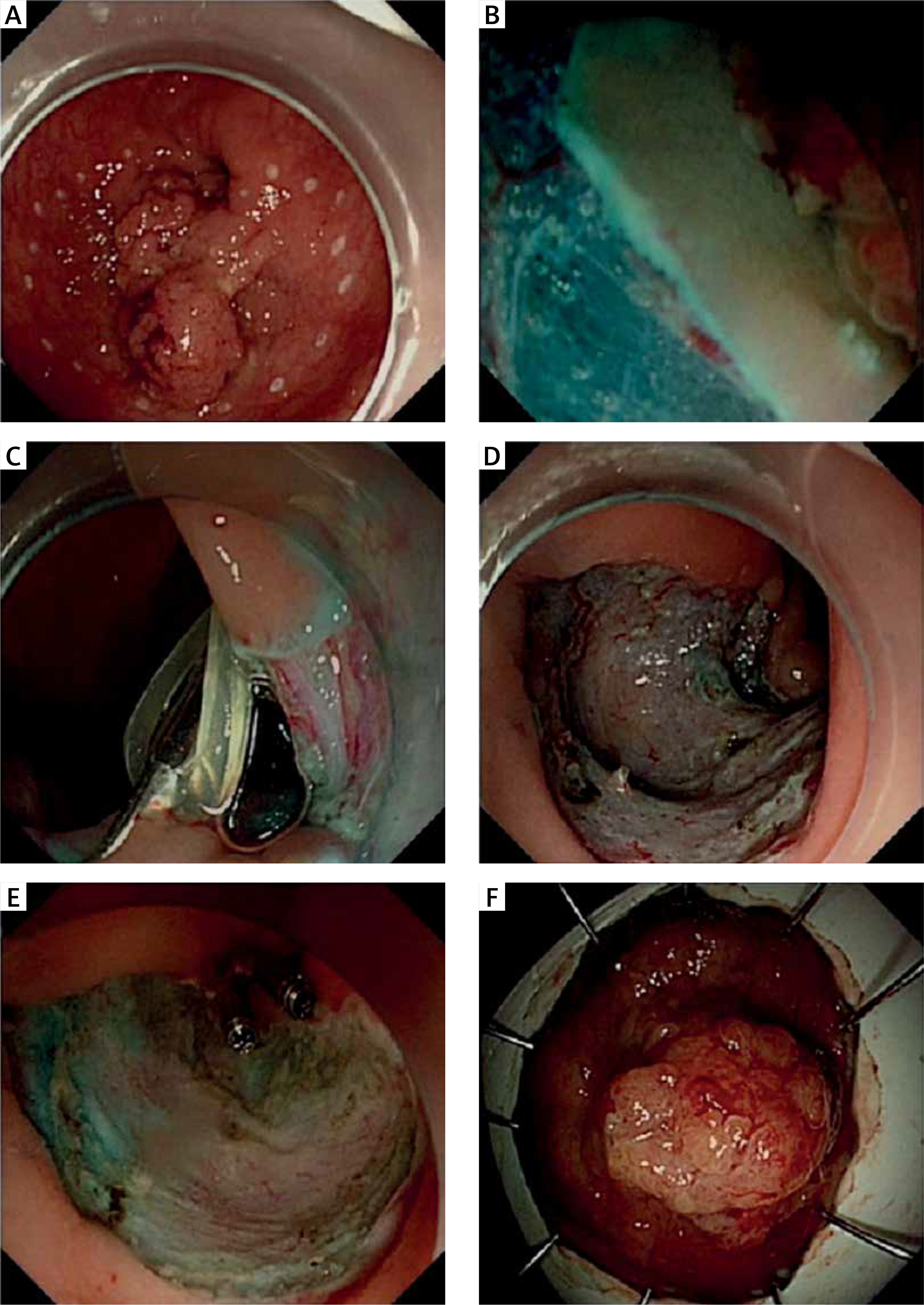
Photo 1
GAW-ESD with internal traction-assistance. A – Circumferential marking with Dual knife. B – V-shaped submucosal dissection below the liquid surface. C – Internal traction using one-matching-two repositionable clips attached to one rubber band. D – Post-ESD defect. E – Post-ESD defect closed underwater using repositionable clips. F – Resected specimen
– Circumferential margins of the lesion are marked with the Dual knife.
– Submucosal injection with normal saline mixed with methylene blue is performed to lift the lesion, then a C-shaped mucosal incision was made on the anal side.
– The colorectal lumen was instilled with normal saline with no need to remove all the CO2 gas, keeping the existence of a boundary line between CO2 gas and water (different from UESD [3]). After the creation of the mucosal flap on the lower side of gravity, assisted by the buoyancy effect, the under-water part of V-shaped submucosal dissection below the liquid surface was performed from the anal side to the oral side. Subsequently, the creation of the mucosal flap on the upper side of gravity was achieved followed by the above-water part of V-shaped submucosal dissection.
– During the under-water part of V-shaped dissection, if adequate exposure of the submucosal space could not be achieved due to the gravity of the large heavy nodule or severe fibrosis in the submucosal layer, a rubber band would be hooked with one-matching-one-or-more clips and attached to the dissected specimen and the colorectal wall opposite to the lesion respectively, resulting in sufficient internal countertraction. Similar but not identical to the double-clip traction (DCT) method [1, 5], in our study, one rubber band was grasped by the first clip outside the scope and inserted in the working channel of the endoscope. Then the first clip grasping the rubber band was positioned on the free anal part of the lesion. In other words, the first clip was attached to the anal side of the lesion, grasping both the dissected specimen and the rubber band. The second clip grasped the rubber band and was placed on the opposite wall to expose the submucosal space. With the dissection process, more and more free parts of the specimen may be grasped by clips (the third clip) and attached to the rubber band. Fox rubber band 3D (1/4’’), 3.5 OZ. (Orthodontic Tendon) [5] and repositionable clips (AGS MedTech, China) were used.
– Finally, the circumferential mucosal incision on the oral side was completed and the tumor was resected en-bloc.
– Post-ESD ulcer was assessed with CO2 insufflation, and exposed blood vessels were coagulated with hemostatic forceps.
– Water infusion was performed again to achieve a reduction in the size of the post-ESD defect, allowing easy underwater closure using several repositionable clips with the opening size 16 mm in length (AGS MedTech, China).
Results
The clinical characteristics of the patients and GAW-ESD outcomes are shown in Table I. Of the 8 patients, 3 were female, 5 were male. Mean age was 55.1 ±6.6 years. Mean size of the lesions was 42.1 × 37.8 mm. Mean duration of the procedure was 72 min (range: 42–151 min). During GAW-ESD, internal traction was used in 3 patients (3/8), with the number of clips ranging from 2 to 3. The rates of en bloc, R0 and curative resection were 100%, 100%, and 87.5 %, respectively. Hematochezia occurred in 1 patient 7 days after the procedure, and then was resolved by endoscopic clipping.
Table I
Characteristics and GAW-ESD outcomes of patients with large colorectal tumors
Discussion
To the best of our knowledge, this is the first study of large heavy colorectal tumors treated by GAW-ESD with/without internal traction assistance to be reported in the literature. During conventional UESD [2, 3], the body positions of patients must be changed depending on the direction of gravity with regard to the lesion, such as the left lateral decubitus position, right lateral decubitus position, supine position, and prone position. Unlike conventional UESD [2, 3], our GAW-ESD [4] allows all the patients to be kept in the left lateral position during the whole procedure, regardless of the direction of gravity of the lesion. For the part of the lesion on the lower side of gravity, submucosal dissection may be performed assisted by buoyancy below the liquid surface; and for the other part on the upper side of gravity, submucosal dissection will be performed assisted by gravity above the liquid surface. Furthermore, the purpose of V-shaped submucosal dissection is to improve efficiency. What is worth mentioning, unintended CO2 insufflation should be avoided to ensure operational stability and minimize the risk of perforation during dissection. Even for those difficult lesions located in intraperitoneal colons including the transverse colon and sigmoid colon, when the maneuverability of the endoscope may become poor, the gas-alternating-water infusion method also can ensure a stable operative platform, allowing the endoscopist to free up his/her right hand for manipulating the endoscopic knife with great precision, with no need to hold the endoscope with his/her right hand. One should note that adequate bowel preparation is an essential precondition for colonoscopy [6], and so it is for GAW-ESD. A clear view field in saline solution may ensure safety during the procedure.
For a granular-mixed laterally spreading tumor (LST-G-mix), it may be insufficient to expose the submucosal space under the large heavy nodule just relying on the buoyancy effect. Various methods [1, 5, 7–9] have been developed for traction-assisted ESD enabling the submucosal layer to be visualized, resulting in safe and quick dissection. Among them, the DCT method [1, 5] allows one to design freely the countertraction direction without the need to withdraw the endoscope. Based on this DCT method, we modified the internal traction technique using one-matching-many repositionable clips attached to one rubber band to avoid the visual field being obstructed by gravity of the large heavy nodule.
Conclusions
Our cases show that GAW-ESD with/without internal traction assistance depending on the level of exposure of the submucosal space is safe and effective for en-bloc resection of large colorectal lesions regardless of gravity direction, with the advantages of quick gas/liquid switch, stable platform, fixed position, buoyancy effect, counteraction design, dissection acceleration, heat-sink effect, optical zoom effect, and downsizing effect.