








Introduction
Thyroidectomy remains one of the most commonly performed procedures with an increasing demand in the population [1]. It is estimated that 10–15% of the adult population has thyroid disease, with a strong predominance of women [2]. Thyroidectomy is offered to patients who have benign goitres if they are experiencing compressive symptoms or have hyperfunction [3]. Therefore, the main aim of these operations is to alleviate the symptoms and improve quality of life (QOL). However, as with any surgery, there are certain difficulties that can lead to adverse outcomes.
Conventional open thyroidectomy (COT) has been the standard of care for surgical treatment [4]. An open thyroidectomy is traditionally performed through a transverse cervical incision, which leaves a scar on the neck in an unfavourable location from a cosmetic point of view, and although COT remains the gold standard, the neck scar is most concerning for young women [5].
As with every surgical procedure, there is constant search for better and safer surgical techniques and methods to achieve better outcomes. In 1996. Gagner et al. were the first to introduce the concept of endoscopic neck surgery of the thyroid or parathyroid glands, reporting the first case of endoscopic parathyroidectomy [6]. Subsequently, in 1997, Hüscher et al. published the first endoscopically performed case of thyroid lobectomy [7]. Since then, the minimally invasive concept for thyroid surgeries has been introduced. Compared to COT, minimally invasive thyroidectomy has the advantage of better cosmesis, shorter scar length, and reduced postoperative pain [8–10].
Various surgical techniques are emerging because of advancements in endoscopic thyroidectomy (ET). A gasless ET may be performed using an anterior chest approach, a transoral approach, an axillary approach, a postauricular approach, or a facelift approach. With CO2 insufflation, there are a number of approaches, including cervical, axillary, anterior chest, breast, transoral, and axillo-breast ones [11–15].
Besides disease control, postoperative QOL after thyroidectomy is of equal importance [16]. Especially since patients with thyroid diseases usually have a lower health-related quality of life (HRQOL) than the general population [17]. A number of factors are known to impact QOL after thyroidectomy, including voice and swallowing functions, postoperative pain, shoulder discomfort, sensory abnormalities, dyskinesia, and cosmetic effects [18, 19]. Even with no complications, thyroidectomy can negatively affect daily life due to lifetime hormonal replacement or persistent voice or swallowing discomfort [20].
The most widely used method to achieve particularly good cosmetic results after hemithyroidectomy is transaxillary endoscopic lobectomy. In comparison to COT, its only disadvantage appears to be more pain after surgery due to a greater surface area of tissue dissection, resulting in slower postoperative recovery and poorer postoperative QOL [21]. However, there is currently a lack of studies that have analysed HRQOL after transaxillary endoscopic hemithyroidectomy to identify possible causes and allow improvements to be made to achieve better results [20].
Aim
We conducted this study to investigate and evaluate HRQOL after transaxillary endoscopic lobectomy.
Material and methods
We performed a prospective clinical study with patients who underwent transaxillary endoscopic gasless hemithyroidectomy (TAH). This procedure was performed by one surgeon. Routine preoperative diagnostic tests such as neck ultrasound, fine needle aspiration cytology, and thyroid function laboratory tests were performed for all patients. Patients answered the Short-Form 36 Health Survey (SF-36) [22] before surgery, at 1 and 6 months after surgery, and declared postoperative symptoms after the surgery during a visit in the outpatient clinic. Hemithyroidectomy patient HRQOL preoperative scores (trial group) were compared with the general population, who had a visit to their family doctor in the outpatient clinic for preventive healthcare (control group), to make sure that our trial patients had no major health problems.
We collected data on patient hospital stay, surgery time, removed lobe volume and weight, node diameter, drain placement, drainage duration, complications, and histological examination details. Removed lobe volume was calculated using the formula: height*width*depth*correction factor (0.63) [23].
Patient inclusion criteria for TAH were adapted in our clinic from Ikeda et al. [24]:
Motivated patients (committed to scar-free neck).
Dominant thyroid nodule size < 6 cm at the greatest diameter.
Benign, according to thyroid cytology, or papillary carcinoma (< 1 cm) without risk factors.
Ability to understand the surgical options and provide informed consent.
No previous neck surgery, except cases when previous endoscopic lobe resection was performed and microcarcinoma without vascular spread or overgrown thyroid gland capsule without lymph node invasion was identified histologically.
Exclusion criteria:
Preoperative diagnosis of thyroid cancer > 1 cm.
Presence of cervical lymph nodes.
Retrosternal extension.
Previous neck surgery.
Thyrotoxic goiter.
Laboratory tests and thyroid ultrasound positive for thyroiditis.
The TAH surgery procedure was described originally by Yoon et al. [25]. In our center the TAH procedure was slightly modified. This modified procedure was described by us before [26].
Statistical analysis
Continuous variables are reported as mean and SD. Median and range (min.–max.) are used for non-parametric data. Comparisons between groups were performed using Student’s t-test for parametric variables and Mann-Whitney test for non-parametric variables, while χ2 was used for categorical variables. The threshold of statistical significance was set at p < 0.05. Data were analyzed using SPSS software for Windows (version 22.0, SPSS Inc., Chicago, USA).
Results
Forty patients were included in this study. All patients were female, with a median age of 32 years and a median BMI of 23 kg/m2 (Table I).
Table I
Patient demographic characteristics
| Parameter | TAH | |
|---|---|---|
| Patient | 40 | |
| Age, median (range) | 32 (20–63) | |
| Gender, n (%): | ||
| Female | 40 (100) | |
| Male | 0 | |
| BMI [kg/m2] median (range) | 23 (18.04–34.2) | |
Eighty percent of patients had a drain after surgery and in most cases (93.8%) drains were removed on the first postoperative day (POD 1). Most patients were discharged on POD 2. Benign thyroid gland nodes were found in 87.5% of cases (Table II).
Table II
Clinical data
Complications were observed in 12.5% of patients (Table III). All of them were mild and did not require reoperation or long-term treatment. Hypoesthesia of the surgical site was quite common after TAH, although the rate of hypoesthesia decreased 6 months after surgery. We did not include this symptom in the overall complication rate.
Table III
Complication
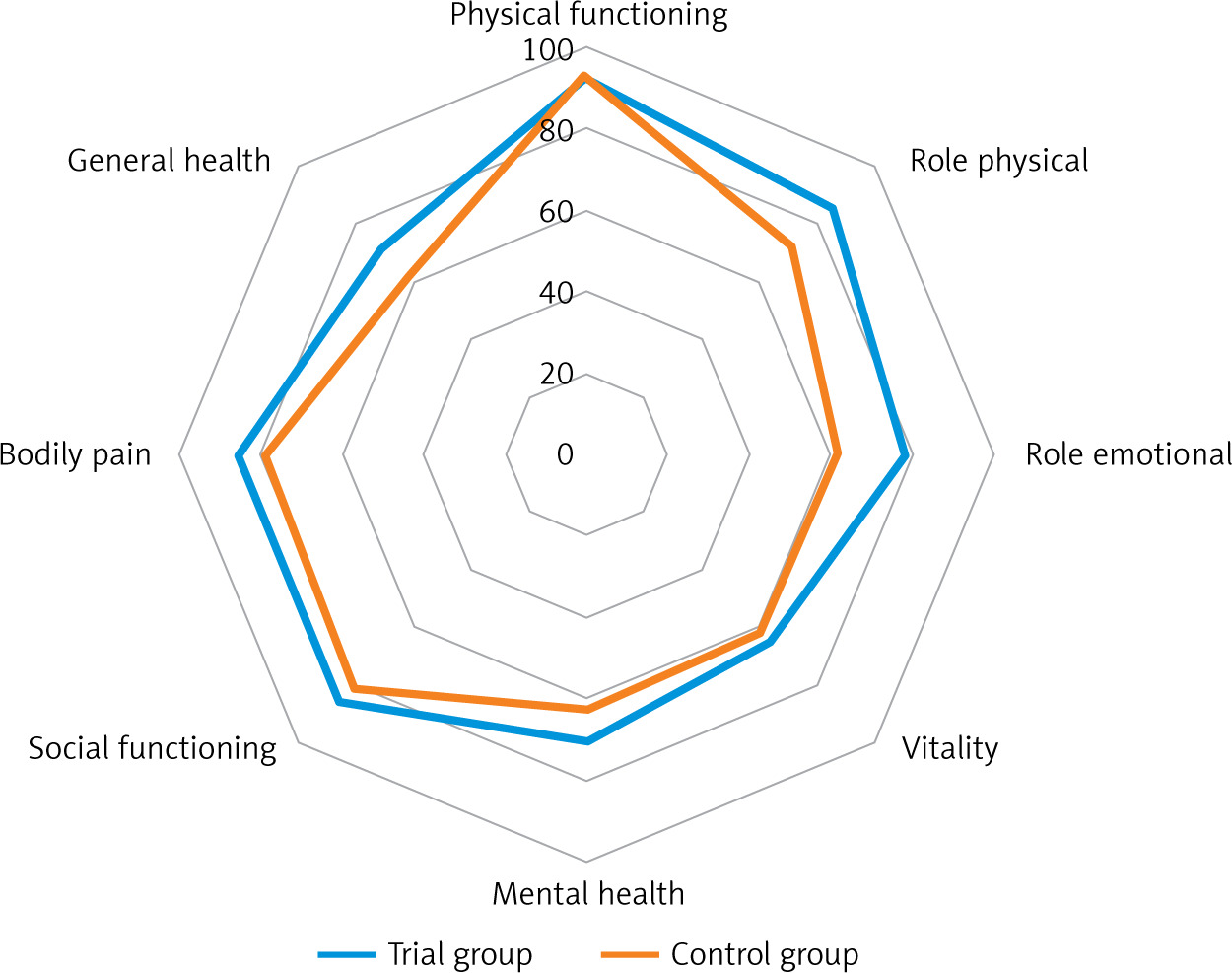
We matched the SF-36 preoperative scores of patients who underwent hemithyroidectomy with people who had a visit to the outpatient clinic for different reasons (excluding thyroid gland surgery). All of them had no major health problems and had to visit the family doctor for preventive healthcare. The control group was matched to the trial group by patient age, gender, and BMI. Overall, 328 patients were included in the control group. HRQOL results showed that the trial group patient health is better in role physical (RP), vitality (V), mental health (MH), bodily pain (P), and general health (GH) aspects prior to surgery than control group (p < 0.05). Role emotional (RE), social functioning (SF) and physical functioning (PF) scores were the same in both groups (p > 0.05) (Figure 1).
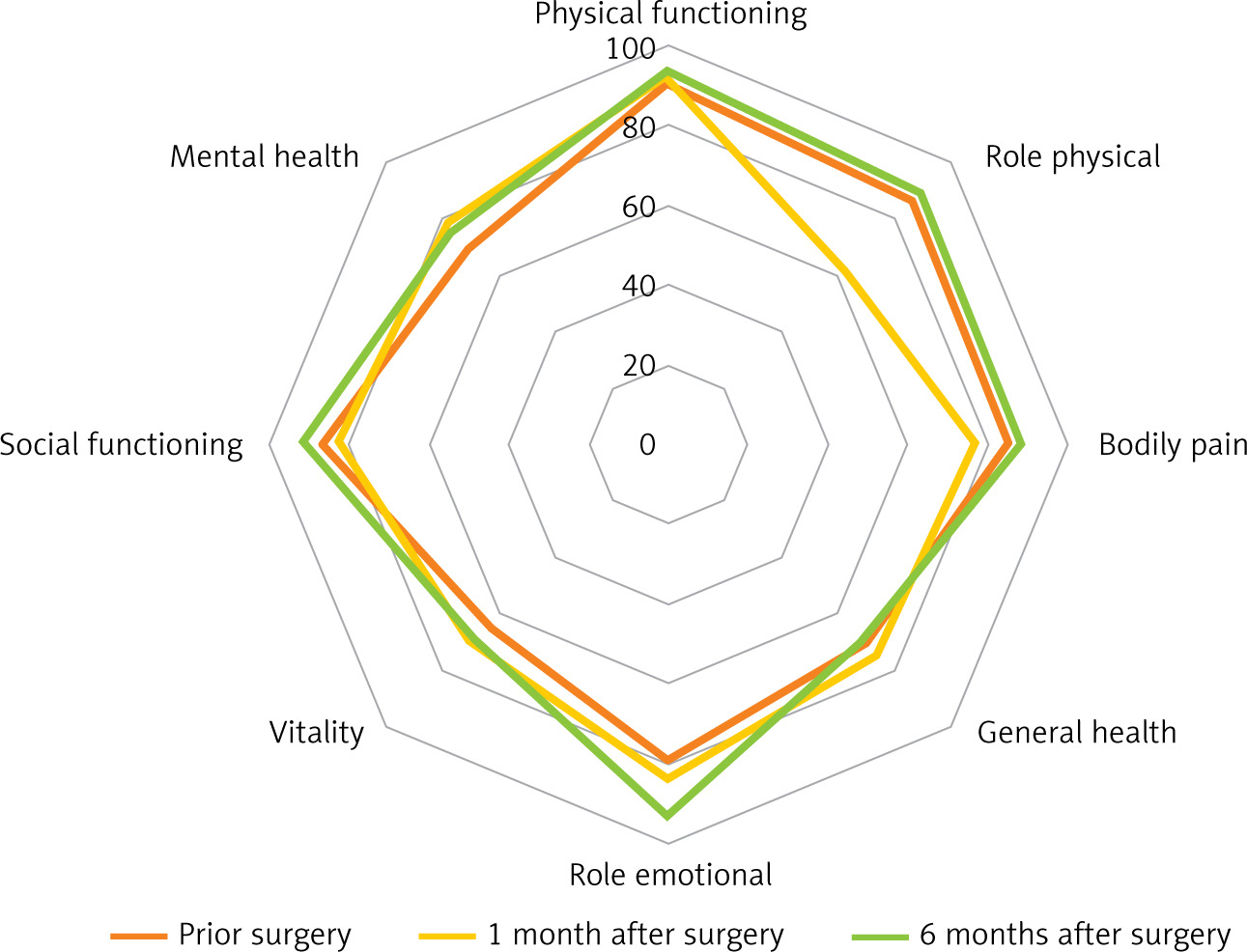
The SF-36 was used to assess pre- and postoperative HRQOL. One month after surgery, patient RP rate was lower compared with preoperative results (86.18 ±27.07 vs. 62 ±37.58; p < 0.05). BP score 1 month after surgery was also lower (85.19 ±22.4 vs. 76.8 ±20.49; p < 0.05). RP and BP scores reached the preoperative level 6 months after surgery. Patient RE status 6 months after surgery was higher than before surgery (78.94 ±34.16 vs. 93.38 ±19.24; p < 0.05). Other SF-36 variables were not statistically different before and after TAH, although a tendency to better results after surgery in V and MH variables exists (Figure 2).
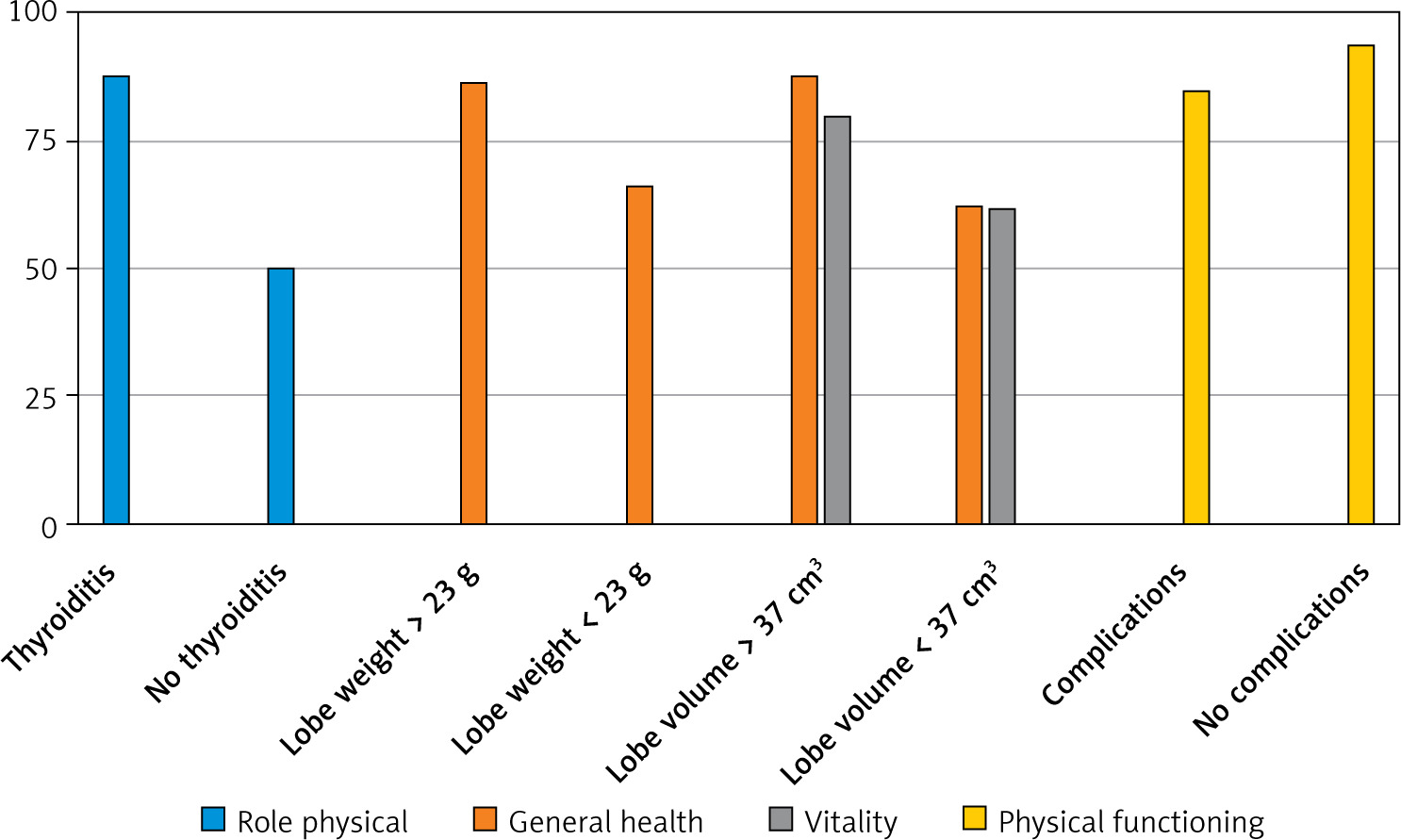
Patients were matched and divided in two groups by a lower and higher level of median age and BMI, mean surgery time, mean resected thyroid gland lobe weight and volume, thyroid gland node size, presence of drainage, thyroiditis in pathological examination, and postoperative complications. HRQOL scores were compared between these different groups. Analysis showed a statistical difference in some clinical groups. RP, GH, PF and V scores were changed (p < 0.05) 1 month after surgery in patients with different pathological examination results, lobe weight, lobe volume, and postoperative complications (Figure 3). PF score 6 months after surgery decreased in patients who had postoperative complications (95.26 ±7.16 vs. 87 ±9.08; p = 0.036).
Eighteen cases of hypoesthesia of the neck or forearm area after surgery were diagnosed. We matched patients with and without postoperative hypoesthesia HRQOL scores. Before surgery, patients with and without postoperative hypoesthesia HRQOL rates were not statistically different. One month after surgery, there also are no statistical difference between patients with and without hypoesthesia.
Patients who complained of hypoesthesia 6 months after surgery had lower MH (78.2 ±13.57 vs. 62 ±6.92; p = 0.029) and GH (74.25 ±17.56 vs. 46.25 ±13.14; p = 0.007) results compared with patients without hypoesthesia.
Discussion
This study shows SF-36 PF, GH, RE, V and MH score improvement and RP, BP, SF score worsening 1 month after surgery, although statistical differences are observed in RP and BP only (p < 0.05). HRQOL results are similar to other studies [20, 27]. RP decrease after surgery may be related to postoperative pain or restriction of mobility. Improved RE, GH, V, and MH scores after surgery may be related to the patient psychological status after surgery as patients feel free of thyroid gland disease.
Six months after surgery, almost all HRQOL scores improve in comparison with preoperative scores, although the statistical difference is noted in RE only (p < 0.05). Results are also comparable to previous studies [20].
Clinical factors and HRQOL correlation were assessed in our study. One month after surgery, RP score was higher in patients who had thyroiditis in pathological examination, but with no clinical symptoms (p = 0.003). The same results were demonstrated in a previous study [28]. Such thyroiditis may be in the form of “painless thyroiditis” wherein there are no clinical symptoms or lab test changes, or they are mild [29, 30]. Higher HRQOL scores in patients with thyroiditis in pathological examination may be a result of hormone level normalization after surgery. Another reason for worse health before hemithyroidectomy and better HRQOL scores after surgery in thyroiditis patients may be the changed, harder tissue of thyroid gland. According to Alfonso et al., the incidence of tracheoesophageal compression is higher in patients with thyroiditis (67%) than in those with colloid goitre (46%) [31]. After surgery, patients may experience release of compression to the trachea and oesophagus, resulting in better results in HRQOL and other questionnaires [32].
Another clinical factor that correlates with patient health is removed thyroid gland lobe weight and volume. GH scores in the short-term period after surgery were better (p < 0.05) in patients whose resected lobe volume and weight were larger. Also, for patients with larger lobe volume, V scores 1 month after surgery were better in comparison with patients with smaller thyroid gland lobes (p < 0.05). Our results match other studies, which found that larger nodes caused expressed thyroid gland disease symptoms and better results after surgery [32, 33].
We compared SF-36 scores of patients with thyroid gland pathology (trial group) and general patients who visited their family doctor in the outpatient clinic (control group). Better SF-36 scores were found in trial group patients, even though all the control group were healthy and had visits to their family doctor for preventive healthcare. Previous study data are different and found better scores in the general population compared with patients with thyroid gland diseases. The reason for our better results in the trial group may be a low number of patients. The second difference from other studies is that we compared not the general population, but outpatient clinic visitors.
In our study, complications were mild and the complication rate matched previous studies [34]. However, mild complications were reflected in patient health according to worse PF score 1 and 6 month after surgery (p < 0.05). Similar results have been found in another study [32].
Hypoesthesia in the forearm and neck areas seems common after endoscopic thyroidectomy. Our study found a 45% rate of hypoesthesia after TAH. Other studies demonstrate an even higher rate of hypoesthesia after endoscopic surgery [26, 35]. Our experience shows that hypoesthesia after surgery may be related to wide subcutaneous dissection during the surgery. Ikeda et al. reported that large skin flap adhesion between the scar and the subcutaneous tissue in the neck may be the cause of hypoesthesia [24].
We found that most hypoesthesia cases resolve within 6 months. A prospective multicentre European study found that there was no hypoesthesia 12 months after surgery [36].
Patients with temporary hypoesthesia in the forearm and neck areas have no difference of SF-36 scores 6 months after surgery in comparison with patients who had no hypoesthesia after surgery. In our opinion, transient hypoesthesia should not be classified as a surgical complication, because it does not worsen patient health in the long term. However, long-term hypoesthesia negatively affects patient MH and GH. Other studies investigated HRQOL score association with complications after surgery, although hypoesthesia was not included in these studies. Lubitz et al. did not find HRQOL score impairment for patients with and without complications after thyroidectomy [37].
One of the major limitations of our study was that we used SF-36, which is the only questionnaire validated in our language, but it is not a disease-specific questionnaire, such as ThyPRO. The disadvantage of SF-36 questionnaire is the score association with patients’ socioeconomic status, age and gender [38]. Therefore we matched patients by age, gender and disease. Our study did not include patients with thyrotoxicosis, hypothyrosis or carcinomas (microcarcinomas only), which may influence patient’s quality of life negatively. Secondly, larger groups are needed for better power analysis. Although all our patients after TAH were involved in this study and our aim was to determine early results of HRQOL after endoscopic thyroid gland surgery. Also comparison of different thyroidectomy techniques should be performed to better define the outcome of transaxillary endoscopic surgery.
Conclusions
TAH is the procedure most chosen by young females for better aesthetic results. In general, the complication rate after TAH is low, although paraesthesia of the neck and forearm areas occurs quite often. According to the SF-36, patient health 1 month after TAH decreases in RP and BP scores only. However, 6 months after surgery, patients feel better in emotional, physical, and other SF-36 aspects in comparison with preoperative HRQOL scores.