
Hemiplegic migraine (HM) is a relatively uncommon subtype of migraine with aura, characterized by temporary motor weakness or paralysis on one side of the body. The pathophysiology of HM involves genetic mutations that affect ion channels, leading to altered neuronal excitability and cortical spreading depression [1]. After transcatheter atrial septal defect (ASD) closure, newly onset migraine without HM is observed in approximately 15% of patients [1, 2]. Here, we report a case of HM occurring immediately after percutaneous ASD closure, which, to our knowledge, has not been previously documented in the literature as a detailed report of manifestations.
A 41-year-old male patient with a known 2.3 cm secundum-type ASD with left-to-right shunt presented for percutaneous ASD closure due to symptoms of exertional dyspnea and recurrent respiratory infections. The patient had no prior history of migraine or neurological disorders, except for occasional headaches following alcohol consumption. The procedure was successfully performed under general anesthesia with angiographic and transesophageal echocardiographic guidance, and the ASD was closed using a transcatheter Amplatzer occluder device (size 24) (Figure 1).
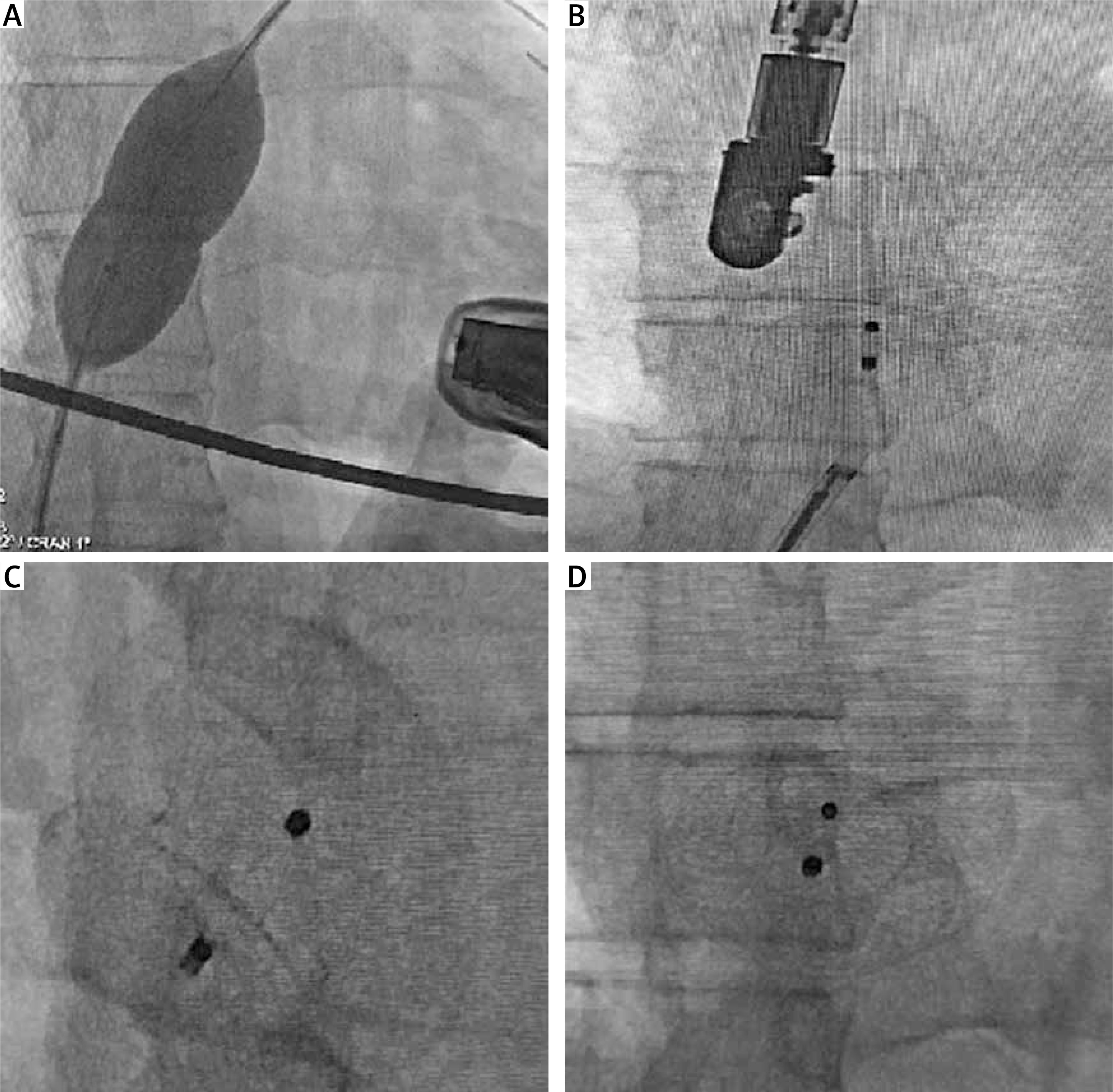
Figure 1
A – Measurement of atrial septal defect using a sizing balloon. B – Closure of atrial septal defect using an Amplatzer occluder. C – Angiographic view of the ASD closed with an Amplatzer occluder from a cranial perspective. D – Angiographic view of the ASD closed with an Amplatzer occluder from an anterior-posterior perspective
Within 24 hours after the procedure, the patient developed sudden-onset left-sided weakness, including weakness of his left arm and leg (4/5 and 3/5 respectively). He also experienced a severe throbbing headache, photophobia, and phonophobia. The neurological examination revealed a motor deficit affecting the left side of his body, consistent with hemiparesis. Additionally, he exhibited aphasia and confusion during the episode. Initial investigations, including brain diffusion magnetic resonance imaging (MRI) and cranial computed tomography (CT) scans, were performed to rule out any intracranial pathology, such as a stroke or bleeding. These imaging studies were unremarkable. The patient was initiated on enoxaparin bid subcutaneously, clopidogrel 75 mg p.o., acetylsalicylic acid 100 mg p.o., and dexamethasone 8 mg b.i.d. intravenously.
The patient’s symptoms gradually improved over the course of several hours, and he returned to his baseline neurological function within 48 hours.
The diagnosis of hemiplegic migraine was made based on the patient’s clinical presentation, which included the sudden onset of hemiparesis, severe headache, and the absence of any structural abnormalities on neuroimaging [1]. The temporal relationship between percutaneous ASD closure and the development of hemiplegic migraine symptoms strongly suggests a potential link between the two [1, 2].
In these patients, migraine attacks tend to occur primarily in the first few days and weeks after the closure procedure. Antiplatelet therapy with acetylsalicylic acid is typically administered for 6 months after closure. Early observational retrospective studies have shown that the addition of clopidogrel to aspirin is associated with a lower frequency and milder severity of migraine attacks [3, 4].
Although the exact mechanisms underlying the development of hemiplegic migraine following cardiac interventions such as ASD closure remain unclear, it is possible that the procedure may have triggered a cascade of events leading to cortical spreading depression and the subsequent neurological symptoms. Increased platelet aggregation has been demonstrated after ASD closure, leading to elevated release of substances such as serotonin, interleukins (IL-1, IL-6, IL-8), and tumor necrosis factor, which are associated with migraine attacks [5]. The striking feature is that all symptoms subside with immediate therapy.
In conclusion, this case report underscores the importance of recognizing and managing rare neurological complications, such as hemiplegic migraine, following percutaneous ASD closure. Healthcare providers should be aware of the potential for such complications and consider initiating aspirin and clopidogrel therapy for 6 months in these patients. Further research is needed to better understand the mechanisms underlying the development of hemiplegic migraine in this context and to optimize patient care in similar situations.









