
Introduction
Risk stratification applies to all types of interventions and forms the basis for making decisions [1]. The risk assessment of cardiac surgery involves risk calculators – in European conditions it is most often EuroSCORE II [2]. In practice, however, the risk calculators have many different limitations. They do not always accurately assess the severity of the disease and do not cover many important risk factors, such as the presence of the fragility syndrome. In clinical practice in various areas of cardiology, the risk assessment strategy using biological markers is of great interest [3, 4]. C-reactive protein (CRP) is one of the most important acute phase proteins. To date, numerous publications have shown a significant relationship between elevated CRP values and worse prognosis in patients with hypertension, myocardial infarction, chronic heart failure or diabetes mellitus [5, 6]. On the other hand, information on the predictive capacity of CRP in patients with valvular heart disease is limited.
Aim
Due to the need to supplement reliable tools for risk assessment in patients undergoing heart valve surgery in the present study, we tried to check the suitability of the CRP parameter for predicting death in in-hospital observation in this group of patients.
Material and methods
The present prospective study was conducted on a group of consecutive patients with haemodynamically significant valve disease (aortic stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation) who underwent a replacement or repair of the valve. The exclusion criteria were: patients under 18 years of age, a lack of consent to participate in the study, active neoplastic diseases and active endocarditis. The risk of surgery using EuroSCORE II was calculated for each patient. The day before surgery a blood sample for biomarkers was collected from each patient. Complete blood count was performed with K2-EDTA samples, using a Cobas 6000 electronic counter (Roche, Mannheim, Germany). The plasma levels of C-reactive protein were measured by the Cardiac C-Reactive Protein (Latex) High Sensitive Test (Roche, Germany), the plasma levels of NT-proBNP were measured by the electrochemiluminescent immunoassays Elecsys 2010 (Roche, Germany) and the plasma levels of high-sensitivity troponin T (TnT) were measured by the Troponin T hs-STAT (Roche, Germany). Baseline characteristics of the patients are presented in Table I. The mean age in the studied population was 63 ±12. The mean plasma preoperative CRP level was 0.39 ±0.3 mg/dl. All procedures were performed through a midline sternotomy incision under general anaesthesia in normothermia. All patients were given cold blood cardioplegia at the initial dose of 15–20 ml/kg followed by booster doses of 5–10 ml/kg every 20 minutes. The primary end-point was in-hospital death from all causes. Patients were followed by direct observation during hospitalization. The study was conducted at the Institute of Cardiology, Warsaw. The protocol was approved by the Institutional Ethics Committee.
Table I
Baseline characteristics of the study population (n = 562)
[i] Values are represented by the mean* and a measure of the variation of the internal standard deviation. AVR – aortic valve replacement, MVP – mitral valve plasty, MVR – mitral valve replacement, ICU - intensive care unit, GFR – glomerular filtration rate, CRP – C-reactive protein, TnT – troponin T, LV – left ventricle, NT-proBNP – N-terminal of the prohormone brain natriuretic peptide, NYHA – New York Heart Association.
Statistical analysis
All analyses were performed using SAS version 9.2. Intergroup comparisons were made using the Pearson χ2 test or Student’s t test. Logistic regression was used to assess relationships between variables. The pre-operative covariates age, body mass index, atrial fibrillation, diabetes mellitus, hypertension, peripheral atherosclerosis, bilirubin, creatinine, CRP, troponin T (TnT), N-terminal of the prohormone brain natriuretic peptide (NT-proBNP), as well as intraoperative covariates such as aortic cross-clamp time and cardiopulmonary bypass time, were investigated for association with the endpoint in univariate analysis. Significant determinants (p < 0.05) identified from univariate analysis were subsequently entered into multivariate models. Spearman’s rank correlation coefficient was used to search for associations between the pre-operative serum CRP level and haemoglobin, red cell distribution width (RDW), left ventricle ejection fraction (LVEF), TnT, creatinine and body mass index (BMI). The cut-off point for the CRP parameter which fulfils the criterion of maximum sensitivity and specificity for the primary endpoint was determined based on the Youden index.
Results
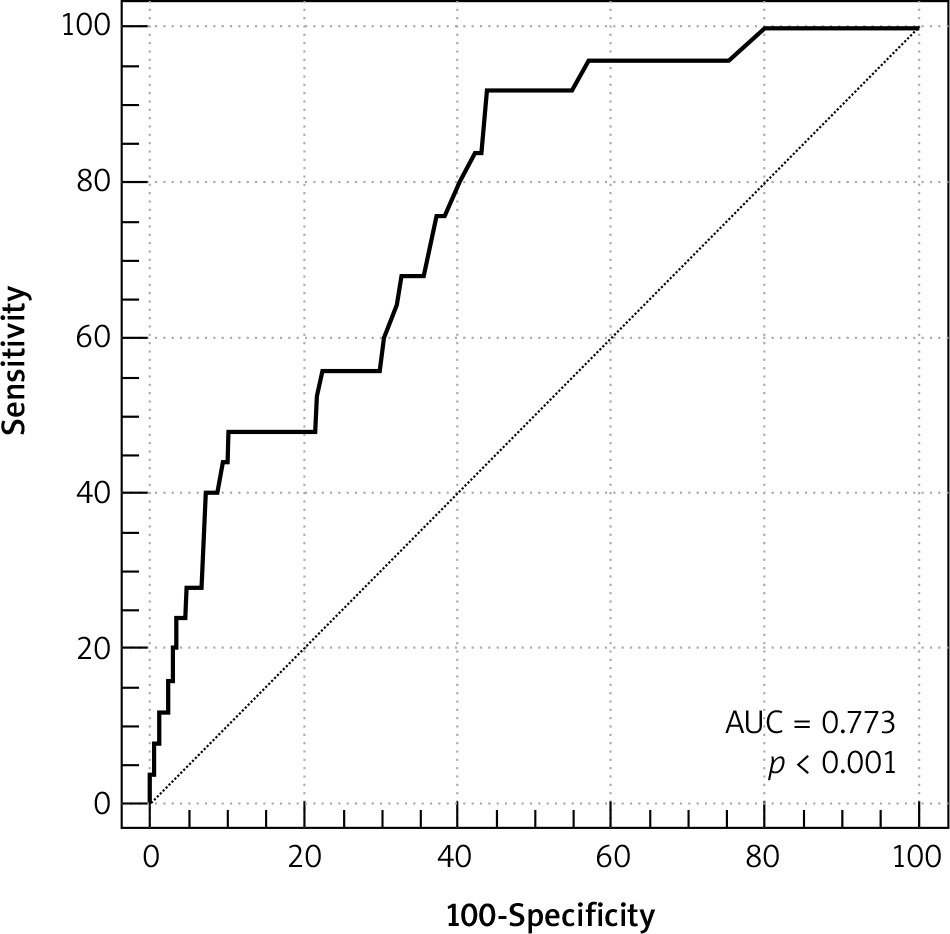
The study included 562 patients who underwent valve surgery. The primary end-point occurred in 25 patients as a result of gradually increasing multi-organ failure. The actual in-hospital mortality was 4.4% vs the mortality 3.5% predicted by the EuroSCORE II model. Statistically significant predictors of primary end-point in univariate analysis are presented in Table II. In multivariate analysis age (OR = 1.068; 95% CI: 1.015–1.124; p = 0.01), CRP (OR = 1.410; 95% CI: 1.038–1.916; p = 0.02), and NT-proBNP (OR = 1.010; 95% CI: 1.002–1.022; p = 0.03) remained independent predictors of the primary endpoint. The optimal cut-off point for the primary end-point was calculated at 0.5 mg/dl. The area under the receiver operator characteristic curve for in-hospital death for CRP is 0.773 (95% CI: 0.736–0.808) (Figure 1). A significant correlation was found between the level of CRP and haemoglobin (r = –0.3; p < 0.0001), RDW (r = 0.22; p < 0.0001), EF (r = –0.24, p = 0.007), TnT (r = 0.3;p < 0.0001), creatinine (r = 0.26; p = 0.001) and BMI (r = –0.29; p = 0.005). The mean value of preoperative hs-CRP in the group of patients who died in the postoperative period was 1.03 ±0.55 and was significantly higher compared to patients who survived 0.35 ±0.3 (p = 0.005). In addition, patients who died were older (71 ±14 vs. 62 ±12; p = 0.01), were characterized by a higher incidence of chronic diseases such as coronary artery disease (33% vs. 14%; p = 0.03), chronic kidney disease (46% vs. 30%; p = 0.02), atrial fibrillation (61% vs. 41%; p = 0.02) or diabetes (24% vs. 17%; p = 0.04). The risk of surgery calculated using the EuroSCORE II calculator in the group of patients who died was on average 7.4 ±5% and was significantly higher compared to patients who survived, 2.9 ±2.5. The average stay in the intensive care unit in the group of patients who finally died was 25 ±17 days and was significantly longer compared to patients who survived 4 ±2.
Discussion
An inflammatory reaction is a local or systemic response of the organs or tissues of the body to many damaging factors. The intensity of the inflammatory reaction in the tissue or organ structure depends on the efficiency of the body’s immune mechanisms, which limit the extent of this process. The presence of the inflammatory process is associated with the dominance of catabolic processes consuming energy reserves, as well as causing the breakdown of storage and structural proteins [7, 8]. Chronic inflammation is a process described in many disease entities. One of the exponents of the inflammatory process is CRP. CRP is a cyclic pentamer that binds ligands in calcium-dependent reactions [9]. CRP is also one of the most important acute phase proteins whose role is to participate in the body’s immune response by facilitating complement fixation and thus opsonization and phagocytosis [10]. CRP is produced in the liver as a result of induction by IL-1 and IL-6. Numerous publications have shown that the presence of inflammation in the body is associated with increased morbidity and mortality [11–14]. It was also described that an elevated CRP value is a predictor of inferior physical fitness and cognitive functions [7]. The lowest levels of CRP are found in people with normal body mass. The relationship between BMI and proinflammatory factors takes the form of the letter U. People with the lowest morbidity and mortality are characterized by normal weight or overweight. Persons in extreme weight groups are at least partially characterized by systemic inflammation [15, 16]. It has been demonstrated so far that elevated CRP values determined after transapical transcatheter aortic valve implantation are associated with worse prognosis [17]. On the other hand, in a study of a group of 416 patients with valvular heart disease, pre-operative CRP values were significantly correlated with the incidence of major postoperative complications in the 30-day observation [6]. In this study, however, due to the limited number of patients, the authors did not assess the usefulness of the CRP parameter as a predictor of only in-hospital death.
Not all patients with elevated CRP values are characterized by increased morbidity. The available literature suggests that morbidity in patients with elevated inflammatory parameters results from the balance between numerous proinflammatory and anti-inflammatory factors [18]. In addition, modifiable factors such as diet, physical activity levels, fat content in the body, smoking or genetic background may play an important role [19–21]. In the present study we found that the pre-operative level of CRP is an independent predictor of in-hospital death in patients undergoing heart valve surgery. It is worth noting that in the whole group of 25 patients in whom in-hospital death was observed, the cause of fatal outcome was a gradually increasing multiple organ dysfunction syndrome. It is also worth paying attention to the fact that the patients who died were older and were characterized by more frequent co-occurrence of chronic diseases such as diabetes, chronic kidney disease or atrial fibrillation in comparison to survivors. A healthy organism has properly functioning mechanisms that maintain its homeostasis and enable its adaptation to the environment, which is especially important in extreme conditions such as cardiac surgery due to cardiac valvular disease [8]. The results of the present study indicate that the ongoing inflammatory process is associated with worse work of individual organs and systems, as indicated by the significant correlation demonstrated between CRP and haemoglobin, RDW, LVEF, TnT, creatinine and BMI parameters, which may have a decisive effect on the cardiosurgical treatment. And although fairly good calibration and discrimination of the EuroSCORE II calculator have been confirmed in the group of Polish patients undergoing cardiac surgery, information about the predictive ability of the CRP parameter may be useful for doctors both during the process of qualifying patients for cardiac surgery and in the postoperative period during patient care in intensive care unit therapy [2, 22, 23].
Conclusions
The inflammatory process is a local or systemic response of the organs or tissues of the body to many damaging factors. One of the exponents of the inflammatory process is C-reactive protein. The present paper is one of the first to indicate the hs-CRP parameter as an independent predictor of the occurrence of a hard endpoint in the form of in-hospital death in patients undergoing heart valve surgery, which can be helpful both during the qualification process for surgical treatment and in the postoperative period when particular attention should be paid to this, especially in patients at risk.









