
A 60-year-old man was admitted as an emergency due to unstable angina. He complained of severe chest pain occurring at rest and radiating to the left arm. He was a heavy smoker and had hypertension and dyslipidemia. The electrocardiogram showed QS complex with T-wave inversion in inferior leads, while myocardial injury markers were negative. Echocardiography revealed preserved systolic and diastolic function without wall motion abnormalities. Since his episodes of recurrent chest pain continued after the admission despite medical treatment, an early invasive strategy for unstable angina was indicated.
During coronary angiography the left coronary artery was successfully cannulated and visualized, revealing insignificant lesions. Despite multiple attempts with five different diagnostic catheters (Tiger, Judkins right 4.0, Amplatz right 1.0 and 2.0 and Amplatz left 1.0), the right coronary artery (RCA) could not be visualized. Since all the attempts FOR cannulation of the RCA failed, while the patient was stable during the procedure without significant elevation of high-sensitivity troponin, it was decided to stop the procedure and transfer the patient for computed tomography (CT) coronary angiography to localize the RCA. CT coronary angiography revealed a high take-off RCA with anomalous origin that was located 30 mm above the sinotubular junction (Figures 1 A, B), with a significant 80% lesion in its medial segment. Furthermore, the coronary ostium was positioned on the anterior aortic wall above the right coronary sinus of Valsalva, with a take-off angle less than 45°.
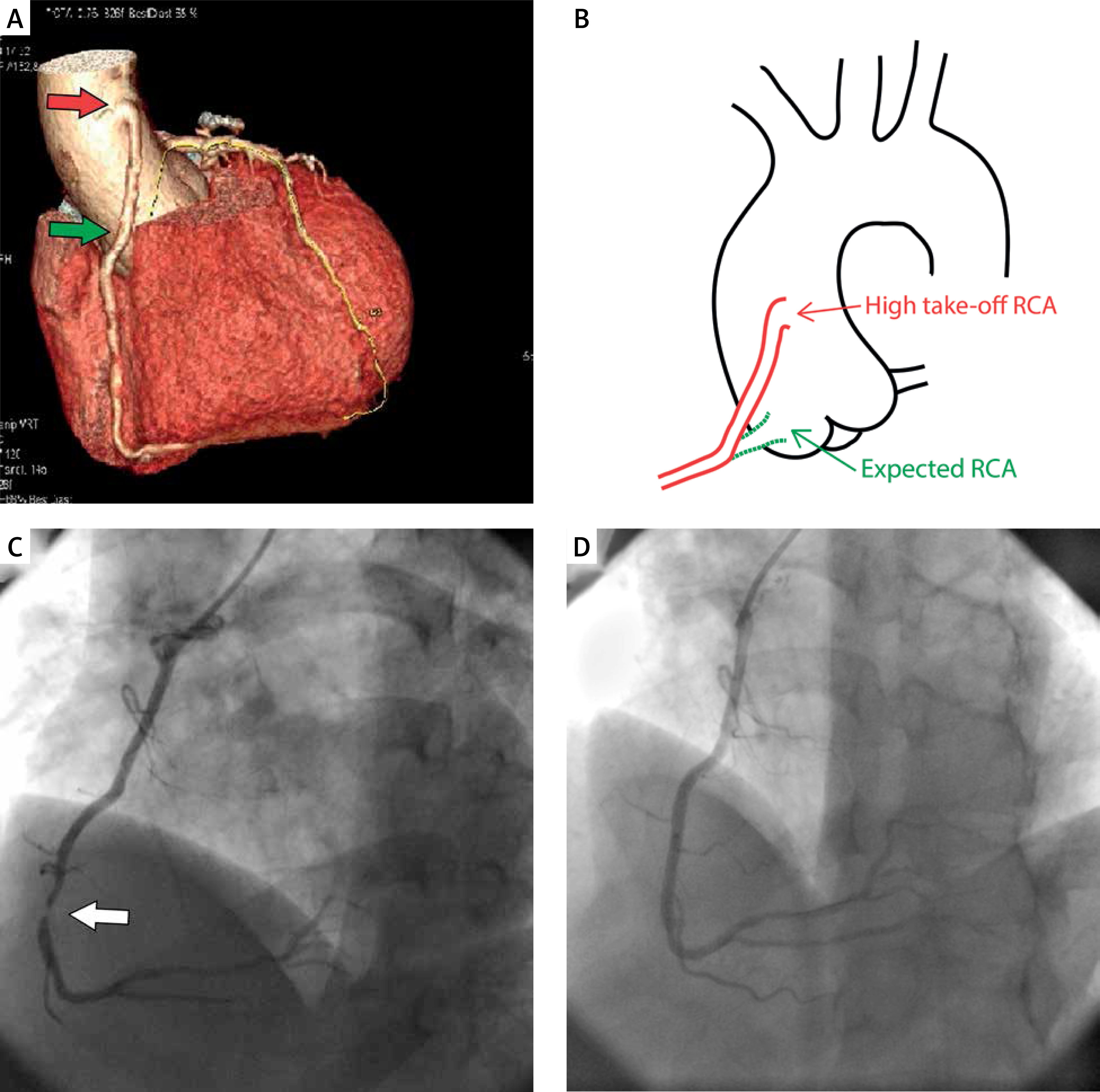
Figure 1
Anomalous origin of right coronary artery (RCA) (red arrow) and expected typical origin of RCA (green arrow) on computed tomography coronary angiography on three-dimensional reconstruction of the heart and aorta (A); scheme depicting the course of high take-off RCA presented in this case compared to typical localization of RCA (B); significant 95% lesion in medial part of RCA (white arrow) on invasive coronary angiography (LAO 38; CRA 24) (C); and optimal result after PCI (LAO 25; CRA 29) (D)
Invasive coronary angiography with CT guidance was repeated and the RCA was successfully cannulated with a right bypass guiding catheter, revealing an even more severe 95% lesion (Figure 1 C). Percutaneous coronary intervention (PCI) was then performed with one drug-eluting stent implanted, achieving optimal result (Figure 1 D). Five days later the patient was discharged in a good general condition and free of symptoms.
High take-off coronary arteries are rare anomalies of their origin that arise > 10 mm above the sinotubular junction. Prevalence of this anomaly is estimated between 0.006% and 0.2% in the general population [1, 2]. The present case is unique because this anomaly disrupted the appropriate management of acute coronary syndrome (unstable angina). Diagnostic aortography could have been an alternative to find the missing coronary artery, but the patient was completely stable and acute myocardial infarction was excluded, so it was estimated that CT would have provided better assessment of the missing coronary artery without a significant increase of contrast given. Although the current guidelines recommend CT coronary angiography primarily to exclude acute coronary syndrome in low-risk patients [3], we hereby show how it played a critical role in elucidating this peculiar anomaly and guiding the subsequent PCI as definite treatment.







