
Introduction
Urinary tract infections (UTIs) remain the leading cause of complaints in outpatient clinics and the most common infectious diseases among women of reproductive age [1]. This term defines various disease entities as cystitis or pyelonephritis. Every year, approximately 15% of sexually active women have an episode of UTIs, and up to 60% of them develop UTIs at some time in their life. The typical symptoms of simple infection include: suprapubic pain, polyuria, urinary frequency and urgency, painful micturition, and, in case of spreading the infection into the upper urinary tract: fever, flank pain, chills, and malaise. On the other hand, asymptomatic bacteriuria (AB) refers to isolation of bacteria in the urine of patient without any symptoms of UTIs. The most common pathogen isolating from the patients with the signs of UTIs or AB is the endogenous intestinal flora, especially Escherichia coli [2]. When it occurs at least twice every 6 months or 3 times a year and follows the resolution of a previous UTI it is classified as a recurrent urinary tract infection (rUTIs). Most often the infection is uncomplicated – it affects non-pregnant women, without anatomical or functional urinary tract defects or comorbidities. It is clinically significant to distinguish complicated UTIs, which are associated with an increased risk of severe course. It occurs, among others, in pregnant women, all men, patients with anatomical or functional abnormalities of the urinary tract, impaired antimicrobial defence mechanisms, renal diseases, inserted indwelling medical devices, or when UTIs are caused by atypical microorganisms
The diagnosis of UTIs is usually made on the basis of reported signs and symptoms supported by laboratory tests (urinalysis and urine culture). The presence of ≥ 105 bacteria per millilitre (colony forming units per millilitre – CFU/ml) confirms the infection, while the antibiogram allows us to verify the effectiveness of the therapy. Urine culture prior to therapy implementation is not obligatory in patients without any known risk factors of complicated UTIs (urologic abnormalities, immunosuppression, or poorly controlled diabetes mellitus); however, it reduces the possible development of drug resistance among uropathogens. It is highly advised when acute pyelonephritis or pregnancy is suspected or if the symptoms do not resolve or recur within 4 weeks after the completion of previous treatment. On the other hand, most infections occur in sexually active women without any identifiable predisposing condition. Close proximity of the reproductive tract indicates that the inflammatory process in the vagina is also well-known risk factor of urinary infections. It is estimated that more than half of UTIs in females are accompanied or preceded by vaginitis [3].
The following paper is an attempt to summarize the current state of the art regarding the treatment and prevention of UTIs in women to avoid the possibility of developing drug resistance by causal strains in the future.
Description of the current state of knowledge
Treatment of urinary tract infections
The choice of first-line therapy differs, depending on the diagnosed disease entity and the patient’s clinical situation.
The first-line treatment in patients with acute simple cystitis depends on the possible risk of infection with a multidrug-resistance (MDR) pathogen. Antibiotics targeted toward Escherichia coli, Proteus, Klebsiella, and Staphylococcus saprophyticus are the recommended first-line treatment. Empirical treatments are often eligible and include nitrofurantoin, trimethoprim-sulfamethoxazole, or fosfomycin [4, 5]. Beta-lactams and fluoroquinolones should be considered as second-line agents due to possible induction of MDR and higher risk of side effects than the aforementioned antimicrobials [6]. In patients with contradictions to the first-line agents or high risk of MDR Gram-negative infection, directed antimicrobial therapy should be introduced. Delayed antibiotic therapy based on the urine culture result is also acceptable.
The first-line treatment in patients with uncomplicated pyelonephritis who do not require hospitalization, should be commenced with a short course of fluoroquinolones.
Asymptomatic bacteriuria should be screened and treated if detected only in pregnant women and in patients prepared to urological procedures breaching the mucosa [7]. Targeted therapy should be preceded by a urine culture.
Pregnancy, especially if complicated by gestational diabetes mellitus, is a well-known risk factor for urinary infection. An increase in progesterone concentration leads to the relaxation of smooth muscles and ureteral dilatation. In combination with immune changes causing the state of relative immunocompromise, it predisposes pregnant women to UTIs [8]. Treatment of any kind of UTI as well as AB in gravid patients should always be targeted due to the high risk of further complications. It means that urine culture with an antibiogram must be performed prior to the introduction of antibiotics. It is estimated that pyelonephritis occurs in up to 2% of pregnancies. In this group of patients, early introduction of broad-spectrum antibiotic therapy is required. The route of administration and the possible management (outpatient vs. inpatient) depend on the baseline condition of the patient.
First-line therapy during pregnancy should include administration of cephalosporins (e.g. cefuroxime) or nitrofurantoin (avoided at term due to possible neonatal haemolysis) [9]. Amoxicillin with clavulanic acid should be carefully used in the third trimester due to the risk of necrotizing enterocolitis in newborns.
The duration of treatment varies by specific drug and type of infection, ranging from 3–7 days in uncomplicated cystitis to 7–14 days in pyelonephritis [10]. However, in the case of uncomplicated UTI treatment, 3 days of antibiotic therapy seem to have similar effectiveness as 5–10 days in achieving resolution of the symptoms [11].
Treatment and prophylaxis of recurrent urinary tract infection
The implementation of optimal therapy is extremely important in the case of recurrent UTIs. Of the 60% of women who develop a UTIs in their lifetime, 30% will struggle with rUTIs. Moreover, it is estimated that up to 20% of pregnant women will experience UTIs, with the recurrence rate of UTIs up to 23% during the same pregnancy or soon after the birth [8].
Recurrent urinary tract infection may cause serious adverse pregnancy outcomes for both mother and child. Meta-analyses have demonstrated that the occurrence of infection during pregnancy increases the risk of preeclampsia [12]. Moreover, the research also provided evidence that the consequence of the infection is lipopolysaccharide-induced damage to the red blood cell membranes clinically manifested by anaemia [13]. Other conditions proven to complicate acute pyelonephritis in pregnant women include preterm labour, intra- uterine growth restriction, and premature rupture of membranes. The last 2 mentioned occur more often, despite rapid and adequate therapy implementation [14]. Routine urinalysis screening and early treatment of detected UTIs should be an integral part of pregnancy management because they enable the prevention of certain complications.
The aetiological factor of the recurrent UTIs should always be diagnosed by urine culture [7].
As well from the aforementioned factors, women diagnosed with rUTIs more often suffer from chronic anxiety, fear, and depressed mood resulting from the unexpected, sudden, and distressing character of UTI episodes [15]. On the other hand, effective prophylaxis reducing recurrence rates improves individuals’ quality of life. Therefore, effective prevention without severe side effects that may impact the individual’s wellbeing would be the best choice.
Insufficient evidence supports the best way to prevent rUTIs. The available interventions that may impact the recurrence rates include pharmacological (antibiotics, immunostimulants) or non-pharmacological (cranberry products, probiotics, behavioural modifications) prophylaxis. All patients should be counselled on the possible risk factors for recurrent infections [16].
Nowadays, due to the possibility of inducing drug resistance among pathogenic strains and the greater number of contraindications, continuous or postcoital antimicrobial treatment as a prophylaxis against recurrent UTIs should be introduced only when available nonantimicrobial interventions have failed.
Pharmacological prophylaxis
Immunoprophylaxis
Vaccines and immunostimulants seem to be the most promising options in the near future. The idea is to stimulate the host’s immune system with the most common pathogens to enhance defence mechanisms against UTIs. Mucosa-associated lymphoid tissue plays a crucial role in humoral and cellular immune response in the urinary tract. Activation of dendritic cells as well as continuous presentation of the antigens seem to be the most rational targets for immunotherapy, based on its unique ability to induce immunity.
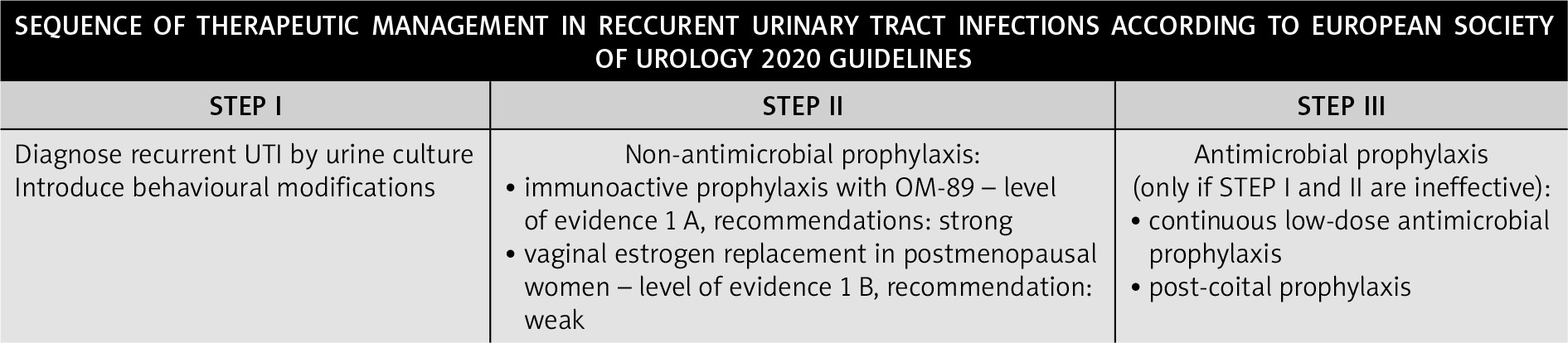
Until now only one product – oral immunostimulant OM-89 (Uro-Vaxom) – has been sufficiently investigated to draw clear recommendations in accordance with current standards. Lyophilized lysate of 18 Escherichia coli strains enhances both innate and acquired immunity (humoral and cellular one) against the most common aetiological factors of urinary infections. Beerepoot et al. assessed the effectiveness, tolerability, and safety of nonantibiotic prophylaxis in adults with rUTIs. According to the available data, the authors concluded that OM-89 decreased the rate of recurrence (RR 0.61, 95% CI: 0.48–0.78) with a good safety profile [17]. After 6 months the mean difference in the recurrence rates between the study group and placebo equalled –0.26 (95% CI: –0.36 to –0.16, p = 0.0004) [18]. Significant reduction in the number of UTIs within the year following initiation of immunostimulant compared to the year preceding administration (3.14 vs. 1.53, p < 0.05) was observed by Brodie et al. [19]. Oral immunization with OM-89 is recommended by the European Society of Urology (EAU) (Fig. 1) and by the Polish Society of Urology in cases of uncomplicated rUTIs (strong evidence, highest level of recommendation – 1 A), in order to reduce the recurrence rates, severity of reported symptoms, the amount of prescribed antibiotics, and the possible MDR strains development in the future [7]. The drug is available orally, due to its resistance to intestinal proteases. It is administered once a day, on an empty stomach (30 minutes before a meal), for 90 days in order to prevent recurrent UTIs. Moreover OM-89 is generally safe and well tolerated by patients. No serious side effects were reported so far. It can be safely administered to immunocompromised patients, elderly people, and women in the second and third trimesters of pregnancy.
Oestrogens in postmenopausal women
Hypoestrogenism, resulting from menopausal transition, is another well-known risk factor related with UTIs. Recurrent infections occur in every fifth women after menopause. Exogenous oestrogens contribute to the restitution of the normal vaginal ecosystem, which poses the theoretical justification for their use in the prevention of rUTIs in this group of patients. Long-term vaginal oestrogen replacement therapy in older women effectively reduces the amount of symptomatic UTI episodes by more than 50% [20, 21].
All the aforementioned contents indicate the necessity for further investigations in order to select the most effective and possibly least invasive preventive strategy of rUTI management. Non-pharmacological treatment should be recommended for all women with recurrent UTIs.
Antibiotic prophylaxis
Continuous antibiotic prophylaxis may be considered in patients with recurrent cystitis not related to sexual activity. Regular long-term prevention with the usage of nitrofurantoin, trimethoprim-sulfamethoxazole, or cephalexin medications is an option in nonpregnant women. The dose of antibiotics is generally lower than that given in acute infection (nitrofurantoin 50–100 mg once daily, trimethoprim-sulfamethoxazole 240–480 mg once daily, or cephalexin 125–250 mg once daily). A comprehensive metanalysis prepared by Albert et al. proved that prophylactic antibiotics used to prevent uncomplicated rUTIs in adult non-pregnant women significantly (more than 6-fold) reduced the recurrence rates (RR was 0.15, 95% CI: 0.08–0.28) while the number needed to treat equalled 1.85 [22] On the other hand, another study showed that approximately 50% of patients develop recurrent cystitis with a similar frequency as before the antibiotic prophylaxis [23].
The recommendations of the World Health Organization regarding antenatal care emphasize that antibiotic prophylaxis in pregnant women may prevent recurrence relapse of UTIs [24]. However, according to the Cochrane Database, a daily dose of nitrofurantoin together with close surveillance has not been shown to prevent rUTIs compared with close surveillance alone [25]. The authors did not find any significant differences regarding recurrent pyelonephritis, rUTIs before birth, and preterm birth. Moreover, it is worth emphasizing that antibiotic prophylaxis may have an impact on the pregnancy-related outcomes and might increase the risk of antimicrobial resistance in the future. According to previous studies, the percentages of strains resistant to selected antibiotics are as follows: trimethoprim-sulfamethoxazole – 30.3%, cefixime 9.9%, pivampicillin 7.5%, and nitrofurantoin 2.5% [9]. Systemic antibiotics may also lead to alternations in human microbiome, especially intestinal and genital tract. Although most therapeutics are well tolerated, the patients should be aware of potential drug toxicities. The most commonly reported complaints include gastrointestinal symptoms (nausea, vomiting, diarrhoea, or stomach pain), skin (rash, pruritus), as well as recurrent vaginal and oral candidiasis [22]. Trimethoprim sulfamethoxazole should be avoided during the first and third trimester of pregnancy, while nitrofurantoin cannot be used by patients with severe renal failure [26, 27].
Nonpharmacological prophylaxis
However, adequate phase III studies are necessary, effectiveness of behavioural changes as liberal fluid intake were proved in previous studies. Increased water uptake of an additional 1.5 litres a day reduces the recurrence of acute cystitis and decreases the risk of antimicrobial therapy use [28]. Other approaches such as postcoital micturition, hygienic habits, urinary alkalisers, or cranberry products, although routinely recommended, have not been proven to be beneficial [29]. In-vitro studies support the biological plausibility of cranberry juice, due to reduced adherence of uropathogens to uroepithelial cells and strain formulation [30, 31]. Although some small studies have demonstrated encouraging results, the recent metanalysis suggests that it is less effective than previously indicated and should not be recommended for the prevention of UTIs [32].
Most previous studies regarding oral probiotics did not demonstrate significant reduction in the incidence of rUTIs [33]. On the other hand, the route of administration may be crucial. Vaginal administration of Lactobacillus decreased recurrence rates [34]. D-mannose has been used in the prevention of rUTIs. This preparation may prevent bacteria from adhering to the epithelium of the urinary tract; however, further studies are required.
Conclusions
In recent years empirical or targeted anti-infective agents together with long-term low-dose prophylactic antibiotics have been the cornerstone in the treatment and prevention of UTIs. However, against the growing drug resistance within the uropathogens, alternative non-antibiotic strategies are becoming an extremely attractive and reasonable solution. Antibiotics should be used for as short as possible, while the dosage and duration of therapy depend on the type of infection. Most recommendations, such as from the EAU, suggest not using antibiotic prophylaxis routinely as a first-line option. In the case of frequent relapses, urine culture prior to the therapy is highly advised. Growing evidence favours non-antibiotic prophylaxis regimens for recurrent UTIs. Wider implementation of immunoprophylaxis in the future may reduce possible side effects of inappropriate antibiotic consumption and may help in reducing drug resistance in causal strains.








