
We present a case of a 74-year old woman with a history of diabetes, hypertension, carotid endarterectomy and stenting of iliac arteries because of peripheral artery disease (PAD), admitted with the recognition of non ST-segment elevation myocardial infarction. Immediate coronary angiography revealed multivessel disease with critical calcified left main (LM) stenosis (Figure 1 A). Additionally, tight aortic stenosis (AS) with reduced left ventricle ejection fraction (LVEF 40%) was diagnosed. Unfortunately, after transfer to the intensive care unit pulmonary oedema occurred, successfully treated with pharmacotherapy. An urgent heart team meeting was held and the patient was disqualified from open-heart surgery because of comorbidities and high risk (EuroSCORE II – 17%). We decided to perform a hybrid procedure, including one stage balloon aortic valvuloplasty (BAV), percutaneous coronary intervention (PCI) and finally transcatheter aortic valve implantation (TAVI). Moreover, computed tomography revealed highly calcified aortic annulus and due to PAD only an alternative approach for TAVI was possible (Figure 1 B corner).
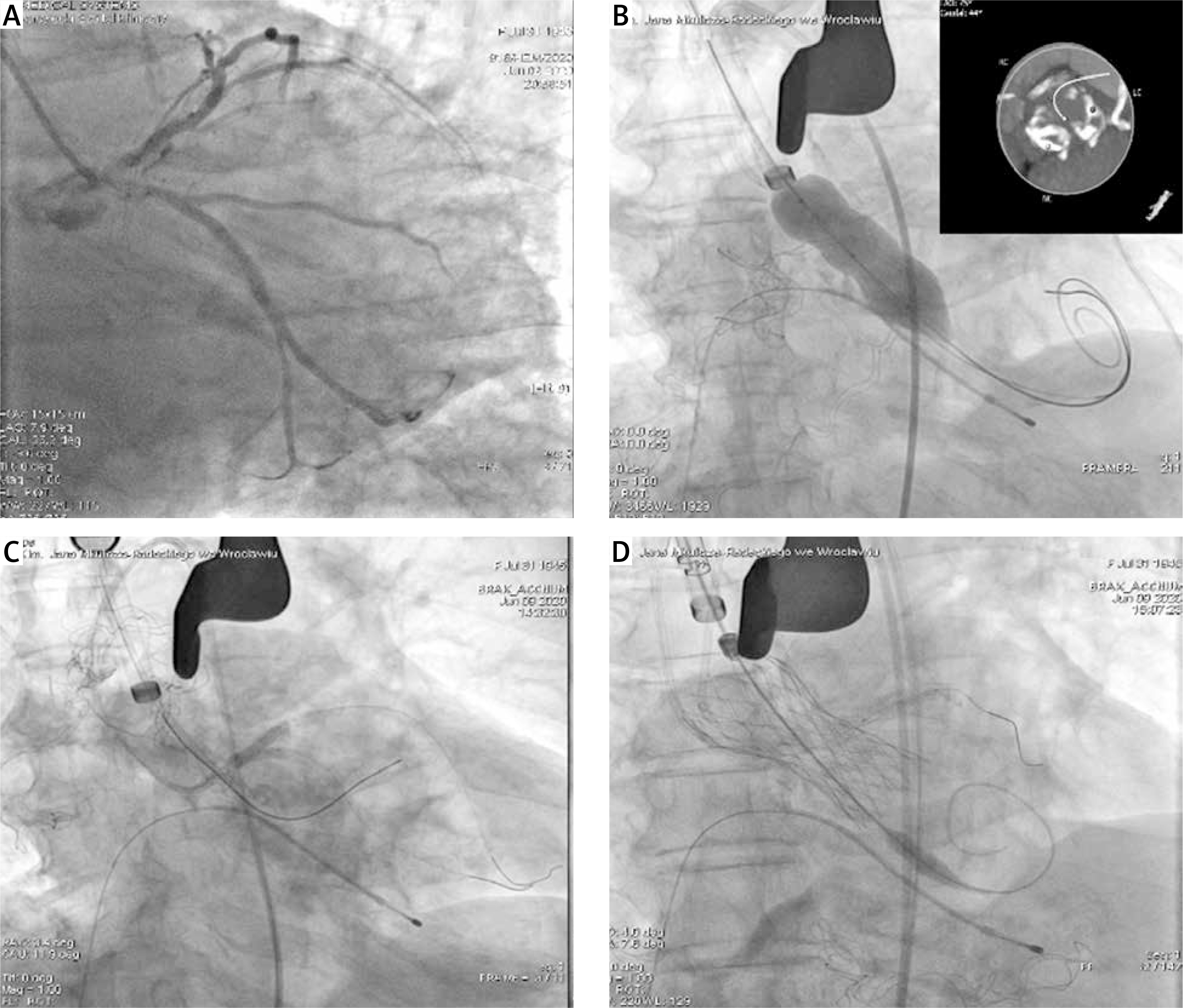
Figure 1
A – Coronary angiography showing critical calcified left main stenosis. B – Balloon aortic valvuloplasty through transaortic approach, parallel second wire for Impella system is inserted into the left ventricle, in the corner computed tomography showing advanced calcifications in aortic annulus and cusps. C – Kissing balloons inflation in the area of left main. D – Successful implantation of the Medtronic Evolut valve through direct aortic access
The procedure started with ministernotomy to perform direct aortic BAV. Moreover, we prepared the Impella (Abiomed, Danvers, MA, US) system in case of emergency and the Impella wire was inserted into the left ventricle, parallel to the valvuloplasty balloon. BAV was performed without haemodynamic compromise (Figure 1 B). Then, through transfemoral access PCI of the LM with two drug-eluting stents (DES) using the Culotte technique was successfully performed with intravascular ultrasound control (Figure 1 C). The rotablator system (Boston Scientific, Marlborough, MA, US) was ready to use, but predilatations of the calcified LM were successful without rotablation. Subsequently, after Impella wire removal direct aortic TAVI procedure was performed and an Evolut R 26 mm (Medtronic, Minneapolis, US) valve was implanted (Figure 1 D). The patient was stable after the whole procedure and discharged home after 5 days with double antiplatelet therapy according to current standards [1]. LVEF at discharge reached 55%.
Different modifications of hybrid procedures including percutaneous or surgical revascularization with transcatheter or surgical aortic valve replacement are possible. They are relatively rarely performed, because of complex logistic and equipment requirements. We had to manage two critical diseases – tight AS and calcified LM stenosis – and we decided to perform simultaneous treatment of both disorders. The correct sequence was however debatable. Which first? The situation was not routine, because performing PCI of the calcified LM first, in case of some complications, could destabilize the patient with tight AS. And vice versa, performing TAVI in a patient with tight LM stenosis carries a risk of coronary occlusion. Therefore, our first step was BAV. From case report descriptions the Impella has been used in patients with AS, so we decided to have it ready to use [2]. The second step was PCI of the calcified LM. Calcified lesions are associated with restenosis, thrombosis and poor long-term prognosis, so we decided to have the rotablator ready – the lesions were however successfully treated with thin struts DES without rotablation [3, 4]. Finally, TAVI through the transaortic approach, which is one of the accepted alternative routes, was performed. The transapical approach was also potentially possible in our patient, but would have excluded Impella support, and a balloon expandable valve might have been inappropriate because of the highly calcified aortic annulus. Hybrid procedures including revascularization and valve treatment are necessary in some patients and tertiary centres should be prepared to perform such complex cases.







