
In percutaneous coronary intervention (PCI) for chronic total occlusion (CTO), various techniques such as parallel wiring or intravascular ultrasound (IVUS)-guided wiring have been developed. If the first guidewire goes into the subintimal space (Figure 1 A), parallel wiring is an option. The main drawback in parallel wiring is the lack of information where the first guidewire went into the subintimal space, i.e., near the distal cap (Figure 1 B), near the proximal cap (Figure 1 C), or somewhere in the middle (Figure 1 D). Although IVUS-guided wiring can provide information where the first guidewire went into the subintimal space, IVUS-guided wiring has been considered as a last resort in several algorithms for crossing the CTO [1], partly because IVUS-guided wiring requires expansion of the subintimal space by small balloon dilatation. Recently, a small profile IVUS catheter has been developed. In this case report, we describe IVUS-assisted parallel wiring technique, in which a small profile IVUS catheter was used just before parallel wiring.
Figure 1
A – The first guidewire goes into the subintimal space. B–D – The first guidewire goes to the subintimal space near the distal cap (B), near the proximal cap (C), or somewhere in the middle (D). E – Corsair advances via the first guidewire. F – IVUS advances via the first guidewire. G – IVUS revealed that the first guidewire remained within the intima from the beginning to the middle of the CTO. H – A double lumen catheter advances via the first guidewire to complete IVUS-guided parallel wiring. I – CTO in mid RCA. J, K – The first guidewire could not reach the distal true lumen. L – Corsair advanced via the first guidewire. M – IVUS advanced via the first guidewire after Corsair. N – White arrow shows the IVUS transducer. IVUS revealed that the first guidewire remained within the intima from the beginning to the middle of the CTO. O – A double lumen catheter advanced via the first guidewire. P, Q – The second guidewire (white arrow) successfully reached the distal true lumen
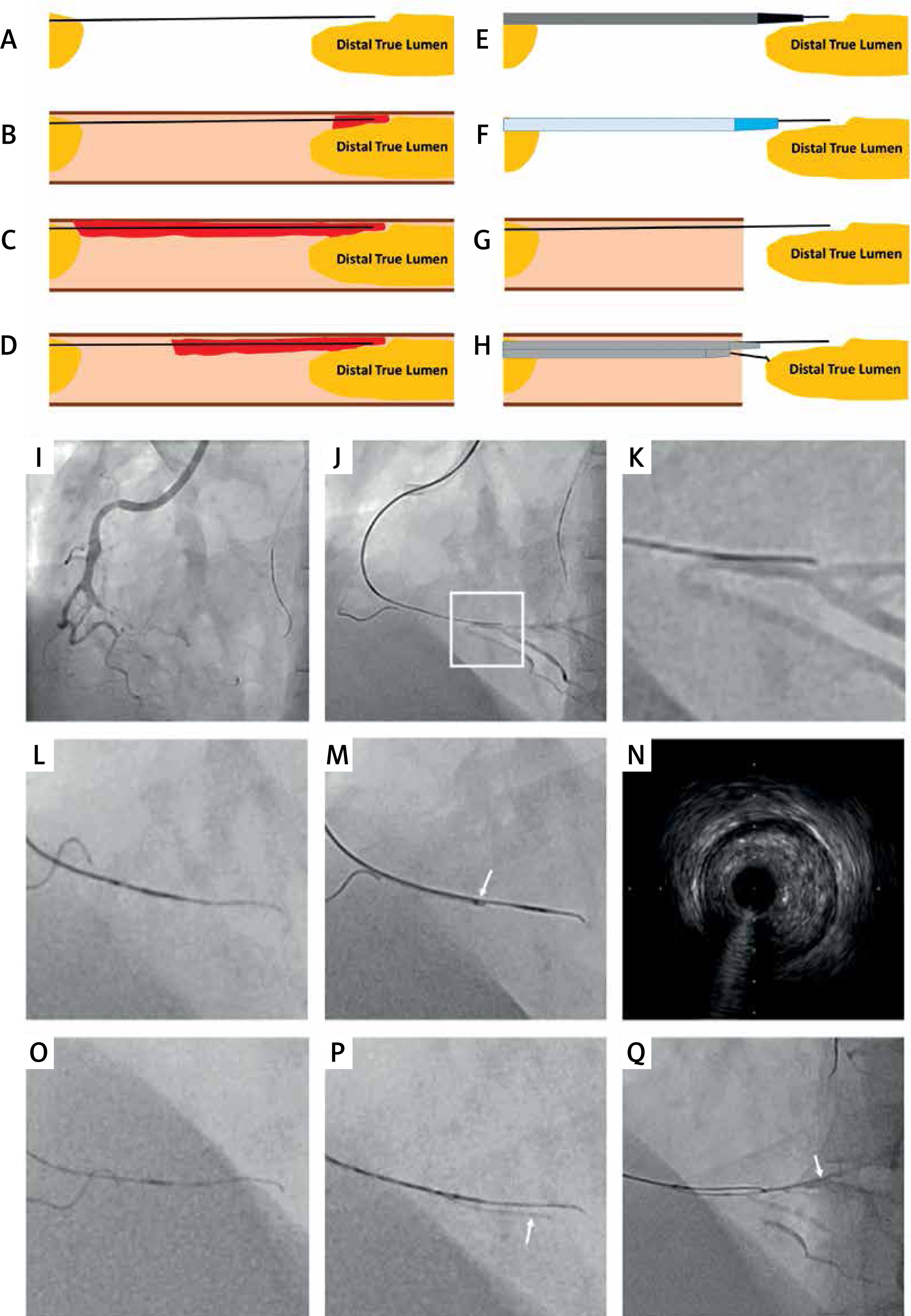
We performed PCI for CTO in the middle part of the right coronary artery (RCA) (Figure 1 I). The J-CTO score was 2 points. An 8 Fr JR4 guiding catheter was engaged in the RCA, and anchor balloon technique using a 2.0 mm balloon was performed to strengthen the back-up force. The Miracle Neo 3 (Asahi Intecc, Nagoya, Japan) with Corsair (Asahi Intecc, Nagoya, Japan) was inserted into the CTO, and advanced beyond the CTO distal cap (Figure 1 J). However, the guidewire could not reach the distal true lumen, and seemed to be in the subintima (Figures 1 A, K). We advanced the Corsair via the Miracle Neo 3 to make a space for the small profile IVUS (Figures 1 E, L). An IVUS catheter (AnteOwl WR, Terumo, Tokyo, Japan) could easily be advanced into the CTO after removal of the Corsair (Figures 1 F, M). IVUS revealed that the Miracle Neo 3 remained within the intima from the beginning to the middle of the CTO (Figures 1 G, N). We recognized that the Miracle Neo 3 finally went into the subintimal space, but the Miracle Neo 3 remained within the intimal space in the middle of the CTO. Therefore, we advanced a double lumen catheter near the distal cap and performed parallel wiring using the Gaia Next 2 (Asahi Intecc, Nagoya, Japan) (Figures 1 H, O, P). The Gaia Next 2 successfully reached the distal true lumen (Figure 1 Q).
IVUS-assisted parallel wiring applied in this case might be one of the useful options in the CTO procedure. In comparison with conventional parallel wiring, IVUS-assisted parallel wiring has the following advantages: (1) operators can understand where the first guidewire goes into the subintimal spaces or remains within the intima, which would help to manipulate the second guidewire; (2) if the first guidewire goes into the subintimal space from the beginning of the CTO or middle of the CTO, switching from parallel wiring to other techniques such as IVUS-guided wiring or a retrograde approach can be considered in the early phase of the CTO procedure, which may shorten the total procedure time. Furthermore, although IVUS-guided wiring usually requires an 8-Fr guide system, IVUS-assisted parallel wiring may be possible in 6-Fr or 7-Fr systems. A key to success for IVUS-assisted parallel wiring is to use a small profile IVUS, which would not expand the subintimal space.
Conflict of interest
Dr. Sakakura has received speaking honoraria from Abbott Vascular, Boston Scientific, Medtronic Cardiovascular, Terumo, OrbusNeich and NIPRO, He has served as a proctor for Rotablator for Boston Scientific; and has served as a consultant for Abbott Vascular and Boston Scientific.







