
Introduction
Endometriosis is a chronic inflammatory disorder characterized by the presence of ectopic endometrial-like glands and stroma, often involving the pelvic organs and frequently leading to anatomical distortion within the pelvis [1, 2]. The prevalence of this disease ranges between six and ten percent [3], while the incidence is believed to be above 33% for patients with acute pelvic pain [4]. Nevertheless, it is difficult to precisely estimate the incidence and prevalence of superficial peritoneal endometriosis because of the absence of an accurate non-invasive biomarker [5]. The main symptoms for affected women include chronic pelvic pain, dysmenorrhea, infertility [6], and deep dyspareunia [7]. However, the management of these symptoms is not standardized, and the disease can recur even after proper surgical [8] or pharmacological management [9]. In particular, we can consider surgery as a cytoreductive therapy, which removes the illness. However, endometriosis can recur. On the other hand, medical therapy acts with a suppressive effect on endometriosis. Similarly but differently, in the case of medical therapy cessation, the illness may be reactivated.
Different hypotheses explain the pathogenesis of en-- dometriosis [10, 11]. The most widely accepted theory involves retrograde menstruation [7], but the exact aetiology remains unknown. As long as the aetiology of endometriosis is not fully understood and the condition has no definitive treatment [12], women suffering from this chronic disease may greatly benefit from insights into environmental factors [13] or interventions that could prevent, modify, or cure endometriosis [14]. Endometriosis is a hormone-dependent chronic inflammatory condition that depends on oestrogen for growth and maintenance. Oestrogen is produced by the ovaries, skin and fatty tissue, and also could be produced locally by the endometriotic lesions themselves through a positive feedback loop between PGE2, aromatase, oestrogen, and COX-2 [15, 16]. In this scenario, an association has been found between diet and oestrogen-dependent diseases (similar to breast or endometrial cancer). Many dietary and lifestyle modifications can play a considerable role in symptom minimization [17] and may influence disease severity or progression [18–20].
The purpose of this paper is to review the literature to evaluate the impact of environment, lifestyle, and diet on symptom expression and endometriosis progression. We also aim to identify a potential diet to help women with endometriosis control their disease or at least find symptomatic relief.
Material and methods
A literature review was conducted using the electronic databases PubMed, EMBASE, and MEDLINE with the search terms ‘endometriosis’ (MeSH) and ‘nutrition’, ‘lifestyle’, ‘diet’, ‘irritable bowel disease’, ‘physical activity’, ‘weight’, or ‘body mass index’ (BMI). The review specifically evaluated articles published in the English language until February 2021. Multiple authors reviewed the papers and independently selected the articles included in this review.
Risk factors and pathogenesis of endometriosis
The incidence of dysmenorrhea has been quoted to be as high as 45–90% in developing countries, and it is a frequent complaint of women who suffer from endometriosis [21, 22], with a robust potential negative impact on the quality of life [23] and psychological wellbeing [24]. The combination of dysmenorrhoea and unexplained infertility [25] appears to be a significant predictor of endometriosis in women suffering from these two concomitant conditions [26, 27], which needs accurate differential diagnosis [28]. Early age at menarche and shorter menstrual cycles have been consistently associated with a higher risk of endometriosis [29–31], potentially as a result of an altered hormonal milieu and an increased duration of exposure to retrograde menstruation. However, with less consistent evidence, researchers have found that endometriosis may be related to the monthly duration of menses, the regularity of menstrual cycles, the heaviness of menstrual flow, and tampon use [30, 32, 33].
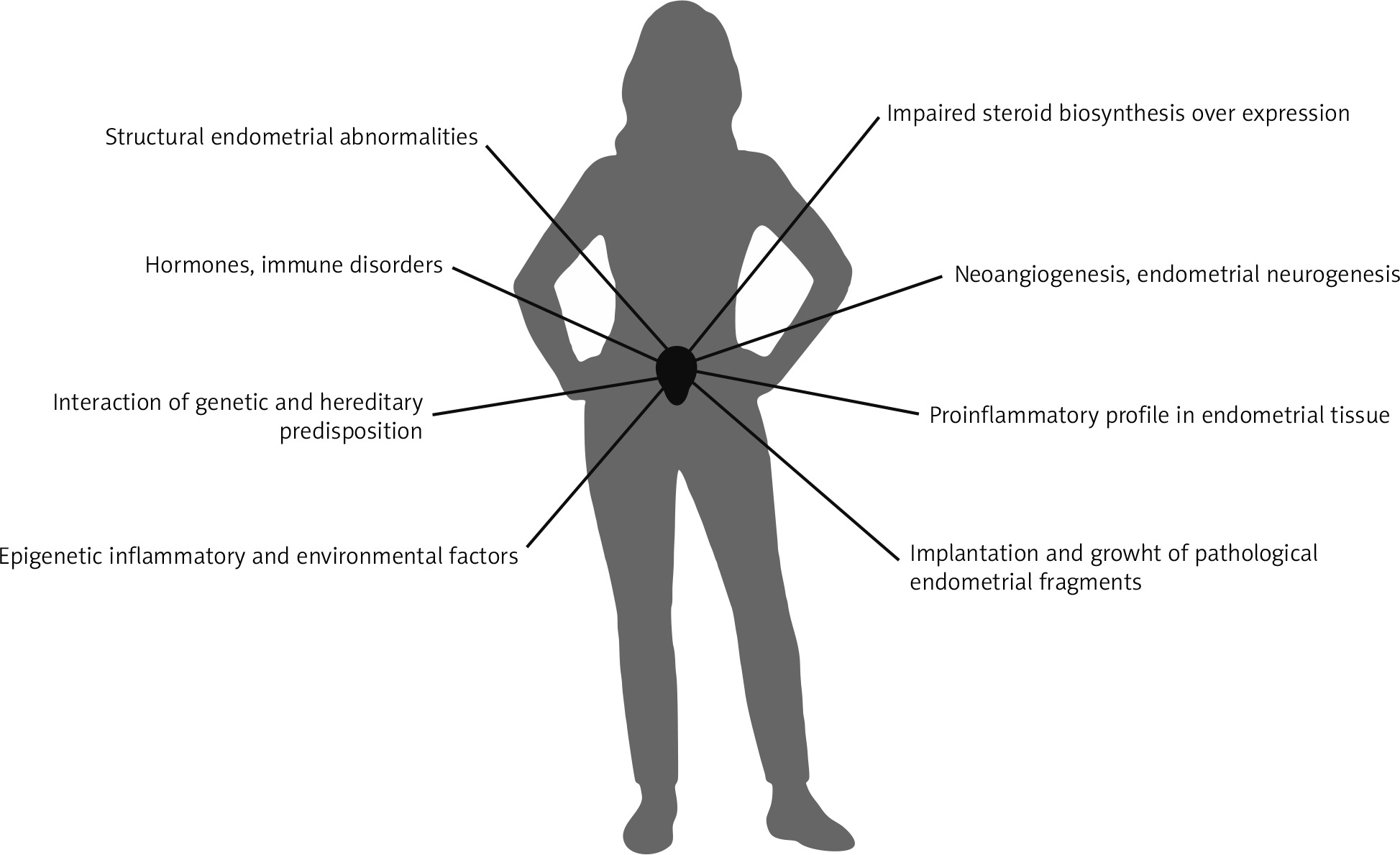
Along with its broad array of risk factors, endometriosis has a multifactorial pathogenesis (Fig. 1). The retrograde menstruation theory can explain the pathogenesis of endometriosis to a large extent, but not completely, as the theory notably lacks an explanation of how endometrial tissue grafts onto the peritoneum. It is obvious that endometriosis is a complex phenomenon caused by the interaction of genetic and hereditary predispositions, epigenetic inflammatory and environmental factors, hormones, immune disorders, and certain structural endometrial abnormalities [1, 34–36]. Indeed, impaired steroid biosynthesis (e.g., hyperoestrogenism, progesterone resistance, or aromatase over-expression) increases the endometrial invasive potential associated with neoangiogenesis, endometrial neurogenesis, and a pro-inflammatory profile in endometrial tissue compared with disease-free endometrium. These are examples of pre-existing endometrial abnormalities that could also promote the implantation and growth of pathological endometrial fragments outside the uterine cavity [37]. Meanwhile, it remains uncertain how these mechanisms participate to create the different phenotypes of endometriosis, and the potential cross-talk of these elements with the immune system within the pelvic cavity [38].
Genetically, women with a first-degree relative suffering from endometriosis are six times more likely to be diagnosed with endometriosis compared to the general population [26]. Moreover, large studies of twins reveal a heritability of approximately 50% [39, 40]. However, the identification of genetic factors causing this condition is incomplete, and the current evidence suggests that the likelihood of having a “major gene” involved in familial endometriosis is low [41–43]. Notably, whole-genome association studies have reported a dozen sensitive regions although these regions account for just over four percent of heritability [36].
The involvement of endocrine-disrupting chemicals in endometriosis remains questionable [44–46]. At present, the evidence of a direct relation between endometriosis and endocrine-disrupting chemicals is inconsistent [47].
New recent findings show that the glandular and stromal components of endometriosis originate from different sources. Moreover, the epithelial component of endometriosis harbours cancer-associated mutations, compared to the stromal component, which is mutation-free. These findings suggested that the stroma is regenerative, unlike the glands. Additionally, the endometriotic lesions were found to have epithelial progenitors and mesenchymal stem cells. All these insights show that endometriosis is derived from different sources and the pathogenetic mechanisms are more complex than expected [48].
Results
Physical factors
Birthweight
Scientific advances in medicine have revealed how intrauterine exposures impact the embryo or fetus by continuously reprogramming its development for extrauterine life [49, 50]. The relationship between birth weight and the risk of developing endometriosis has been the subject of several studies [29, 51–53]. Extremes of birthweight, both low and high, have been found to be associated with a higher risk of developing endometriosis over a woman’s lifetime (RR = 1.3, 95% CI: 1.0–1.8) [29, 51]. However, conflicting data exist regarding prematurity and endometriosis risk, with some studies reporting an increased risk [52–54] and others reporting no association [51, 55, 56]. For an accurate interpretation of the influence of birthweight on the risk of endometriosis, it is necessary to restrict analyses to term births, and for studies including preterm neonates to adjust for gestational age.
Childhood, adolescent, and adult weight
In the same sense as above, the relationship between childhood and adolescent weights and the development of endometriosis is counterbalanced. Early studies described the current state of being thin and underweight as hallmarks of patients suffering from endometriosis, without insight into whether this is a cause or a consequence of their disease or its symptoms [30, 33, 57–59]. Regardless of the patient’s age, current evidence suggests an inverse relationship between BMI and the prevalence of endometriosis [56, 60–62]. However, the association between obesity and endometriosis remains debatable. Some researchers have discovered an elevated incidence of endometriosis in obese women [63] with a correlation between the risk of developing endometriosis and prepubertal obesity [64]. Nagle et al. suggested that women who reported being overweight at 10 years of age had an increased risk of endometriosis (OR = 2.8; 95% CI: 1.1–7.5), whereas there was no clear evidence of an association between relative weight at 16 years of age and the risk of endometriosis [64]. Other researchers have reported an inverse relationship between obesity and the risk of endometriosis [32, 60, 65–69]. In a meta-analysis, Liu et al. found a significant inverse association; the overall analysis revealed a 33% reduction in the risk of endometriosis for each 5 kg/m2 increase in BMI (RR = 0.67; 95% CI: 0.53–0.84), with statistically significant heterogeneity across the studies (p < 0.001, I = 86.9%) [67]. These contradictory results confirm the need for studies with larger numbers to elucidate the real association between being overweight or obese and endometriosis while taking into account metabolic and biochemical parameters.
Physical activity
In view of the inflammatory [70] and oestrogen-dependent profile of the disease [1], the role that physical activity can play in reducing the risk of endometriosis seems highly possible on an intuitive level. Current evidence suggests that endometriosis symptoms may be reduced by physical activity [62, 71]. However, this association is inconsistent [72]. Case-control studies have inconclusively found that patients who exercised regularly had fewer symptoms compared to individuals without self-reported regular exercise [58, 73, 74]. When comparing women with the highest physical activity levels to the lowest, researchers discovered a non-significant decrease in the reporting of endometriosis-related symptoms (RR = 0.89, 95% CI: 0.77–1.03) [75]. Nevertheless, physical activity may influence endometriosis symptomatology and progression due to its known influence on hormonal levels, such as decreasing luteal oestrogens [76] and increasing sex hormone binding globulin levels [77].
Breastfeeding
In a prospective cohort study of 72,394 women, Farland et al. found that breastfeeding was a protective factor for endometriosis-related symptoms among the 3,296 (4.6%) women who had laparoscopically confirmed endometriosis [78]. Additionally, the rate of endometriosis-related symptoms was decreased among women with at least six months of postpartum breastfeeding. Although the causation behind this correlation is not fully understood, the present belief is that the symptomatic relief is due to amenorrhoea [78, 79].
Dietary factors
Alcohol consumption
Data are mixed regarding alcohol consumption and the development of endometriosis [68, 71, 80]. Several studies have identified an association between alcohol consumption and symptoms related to endometriosis, whereas others have not [30, 62, 71, 74, 81–83]. Still, the available evidence is not without limitations. In the studies where researchers found an association between endometriosis and alcohol consumption, it is difficult to ascertain whether the consumption is due to the disease or vice versa. At this time, it also remains unknown whether different types of alcohol affect this disease differently.
Diet
Inflammation, oestrogen activity, menstrual regularity, and prostaglandin physiology are important pathophysiologic processes to consider when diagnosing and treating endometriosis [80]. Diet is an integral component of these factors and, as such, consumption likely has a role in the development and progression of this disease. In fact, a recent case-control study found that women who consume diets with high inflammatory potential are significantly more likely to have endometriosis in comparison to those with less inflammatory diets [84].
A prospective cohort study of the Nurses’ Health Study II population found that women who consume more than two servings a day of red meat have a 56% higher risk of endometriosis diagnosis compared to those who consume less than one serving per week (95% CI: 1.22–1.99), with the association being highest for those who consume non-processed red meats [85]. In contrast, a case-control study comparing the frequency and consumption per week of selected items in the Iranian diet found the intake of red meat to be associated with a lower risk of endometriosis (OR = 0.61, 95% CI: 0.41–0.91) [86]. Jurkiewicz-Przondziono et al. highlighted dietary factors that potentially increase the risk of developing endometriosis, including the high intake of ham, red meat, and trans-unsaturated fatty acids [80]. The authors surmised that the pro-inflammatory profiles of these foods account for their associations with the disease [80].
Omega-6 fatty [87] acids derived from the diet are the precursors of the pro-inflammatory prostaglandins PGE2 and PGF2α, which likely increase uterine cramps and cause the painful symptoms of endometriosis [88]. In the same review, it was also suggested that antioxidant vitamins (D, E, and B-group vitamins) [89, 90], as well as foods rich in calcium and omega-3 fatty acids, may protect against the development of endometriosis [80]. In the cohort study by Darling et al. including 70,617 women (n = 1,383 for the experimental group with confirmed endometriosis and n = 69,234 for the control group), the consumption of products rich in vitamins such as folic acid (p = 0.003), vitamin C (p = 0.02), and vitamin E (p < 0.0001) was inversely proportional to the risk of developing endometriosis [91]. The authors did not find that endometriosis symptoms were mitigated by providing these same vitamins through dietary supplements [91]. A recent double-blind randomized placebo-controlled trial examining treatment with vitamin D [92], omega-3 fatty acids, or placebo in women with surgically confirmed endometriosis and pelvic pain found that women in both the vitamin D and placebo arms had similarly significant improvements in pain scores, while those in the omega-3 arm demonstrated lesser improvements [93]. Thus, while pro-inflammatory omega-6 fatty acids may increase endometriosis-related pain, antioxidant vitamins and omega-3 fatty acids may be protective against these symptoms.
Methylation changes [94], which are a hallmark of cancers and endometriosis [95], are influenced by dietary factors such as folate consumption, calorie intake, and polyphenol content. Such compounds tend to bioaccumulate in lipids contained particularly in meat, liver, and dairy products and can also be counted among the risk factors for endometriosis. However, nowhere in the literature is this association reported.
In a study of curcumin and its impact on endometriosis, the authors found that this spice might have potential benefits for the prevention and treatment of endometriosis. The benefits from curcumin are believed to be due to its anti-inflammatory, antioxidant, anti-tumour, and anti-angiogenic profile [96]. However, because of the limited studies on this topic and inconsistent data, further studies are needed to improve the knowledge of the true impact of curcumin on endometriosis.
Fasting
Fasting can help preserve energy levels [97], thereby providing the body time to regenerate and heal. Increased hormonal modulation, reduced inflammation [98], and increased stress resistance are ways in which fasting may help reduce chronic pain severity. In clinical practice, we have found that strategic fasting can help reduce symptomatic flares among patients suffering from symptoms related to endometriosis. We sometimes advise outpatients to eat lightly or to fast prior to their menstrual cycles in order to lessen the activity of the gastrointestinal (GI) tract, thereby reducing the uncomfortable and painful GI symptoms associated with endometriosis. Currently, there are no studies on the role of fasting in the management of endometriosis.
FODMAPs and irritable bowel syndrome
Irritable bowel syndrome (IBS) impacts 11.2% of the population worldwide and significantly affects quality of life for many women. The role of diet is very important in IBS, both in worsening and improving symptoms for patients suffering from this disorder. The fermentable oligo-, di-, and mono-saccharides and polyols (FODMAPs) comprise a group of carbohydrates resistant to digestion that are found in a broad range of foods. FODMAPs play a substantial role in initiating the symptoms of IBS [96, 99, 100]. Diets low in FODMAPs have a proven efficacy with a high level of evidence in alleviating symptoms related to IBS, and as such were adopted in the IBS treatment guidelines of the National Institute for Health and Care Excellence and the British Dietetic Association. Initiating a diet low in FODMAPs requires the expertise of a dietitian or a clinician with the proper training and experience in this approach [100].
Patients who suffer from IBS are often found to have concurrent symptoms of endometriosis. Women diagnosed with endometriosis are two to three times more likely to receive a concomitant diagnosis of IBS compared to women without endometriosis [96, 101]. Schink et al. found a nearly four-fold increase in food intolerances in patients with endometriosis compared to controls [102]. In addition, Schomacker et al. found a higher prevalence of IBS in women diagnosed with endometriosis compared to women with no endometriosis, regardless of whether or not there was endometriosis infiltrating the bowel [103]. Interestingly, a prospective cohort study found that although 52% of women with confirmed endometriosis had IBS, more severe IBS symptoms were found in patients with lower-stage endometriosis [104].
It seems plausible that the association between IBS and endometriosis is not only epidemiological but that there are also shared pathophysiological pathways. Both disorders cause similar symptoms for patients and are defined by their chronic low-grade inflammatory state. An awareness of the association between IBS and endometriosis is extremely important for the management of patients with endometriosis-associated pelvic pain. While observing a series of 160 women with IBS, Moore et al. reported a significant improvement in symptoms with the effect of the low-FODMAP diet for patients with IBS and endometriosis compared to patients with IBS alone (72% vs. 40%, respectively, p = 0.001) [99]. The authors concluded that a low-FODMAP diet may be beneficial for women suffering from symptoms related to both IBS and endometriosis [99]. Evidence suggests using a multidisciplinary approach to the care of patients with GI symptoms related to either IBS or endometriosis in order to reach an appropriate diagnosis followed by the correct therapy [105].
Soy and phytoestrogens
The weak oestrogenic effect of phytoestrogens present in soy has been found to be associated with an increased risk of oestrogen-dependent diseases [106, 107]. In Japan, soy is commonly consumed and the high phytoestrogen intake there has been associated with an elevated risk of endometriosis. Liu et al. compared the change of endometrial thickness before and after isoflavone supplementation [107]. The authors found that a daily isoflavone dose of more than 54 mg per day may decrease endometrial thickness in post-menopausal women and produce different effects on populations [107].
Nevertheless, it seems that not all phytoestrogens have the same impact on endometriosis. Some animal models have indicated that puerarin and genistein, two phytoestrogens with antineoplastic properties, reduce the burden of endometriotic lesions via inhibiting aromatase and oestrogen receptor-a expression and reducing oestrogen concentrations [107]. In a small case series, Chandrareddy et al. found that dietary phytoestrogens were associated with abnormal uterine bleeding in women [108]. Although these women had a variety of symptoms and pathologies discovered, they all had symptomatic improvement when phytoestrogens were withdrawn from their diet [108].
Gluten-free diet and coeliac disease
Oxidative stress, chronic inflammation, and immunological disorders are features shared between coeliac disease and endometriosis. The literature is scarce regarding the association between these two diseases. Santoro et al. investigated this hypothetical association and detected a higher prevalence of coeliac disease among women diagnosed with endometriosis, but the results were not statistically significant [109]. Caserta et al. reported a case of a woman suffering from endometriosis with concomitant coeliac disease, where a gluten-free diet improved her fertility [110]. Marziali et al. tested the gluten-free diet in 207 symptomatic women suffering from endometriosis and reported a statistically significant improvement in symptoms in 75% of the women [111]. Women exposed to a gluten-free diet had a significantly better quality of life in addition to improved physical and social functioning (p < 0.005) [110]. Both endometriosis and coeliac disease are associated with chronic inflammation, and both present with significant elevations of interferon-gamma (IFN-γ) and interleukin-6 (IL-6). Thus, the authors concluded that a gluten-free diet is efficient in improving endometriosis symptoms after 12 months of treatment and plays an antagonist role by decreasing IFN-γ and IL-6 [111].
High-fat diet
High fat consumption is associated with oxidative stress and inflammation – two key features of endometriosis. Some inflammatory markers, such as IL-6, are found in higher concentrations in women with endometriosis, and are increased by specific fatty acid exposure [112]. In contrast, decreasing oxidative stress using diets rich in antioxidants may be protective against the progression or development of endometriosis [113]. Heard et al. reported an increase in endometriosis lesion development in mouse models after exposure to a high-fat diet independent of overt obesity and weight gain [114]. This association was believed to be due to promoted oxidative stress and inflammatory pathways provoked by high-fat diets. Maintaining a healthy diet has considerable health benefits and may also decrease the risk of endometriosis [114, 115].
The missing link: new insights into fertility outcomes
Recent discoveries in micronutrients have made progress thanks to the pharmaceutical field. In particular, a great effort has been spent on inositol research. Inositols, in the form of myo-inositol and D-inositol, have been proposed as pharmaceutical agents with a positive effect on insulin sensitivity and PCOS women. For this reason, their administration is widely accepted and proposed as adjuvant therapy in women affected by PCOS with difficulty in conceiving [115–120]. Similarly, vitamin D has also been proposed as a possible adjuvant for fertility. However, unlike the inositols, vitamin D excessive levels may play a detrimental role in infertility [121–123].
Conclusions
This paper reviewed the impact of different lifestyle and dietary factors on the development and severity of endometriosis as reported in the literature, emphasizing that this disease is multifactorial with a concomitant inflammatory pattern. High-level evidence and well-designed randomized studies are lacking when it comes to studying the effect of these modifiable risk factors on endometriosis. However, certain studies indicate that fish oil may have a positive effect on reducing pain due to the effects of the anti-inflammatory prostaglandins PGE3 and PGE3α derived from omega-3 fatty acids. The same effects were seen with the introduction of the antioxidant vitamins C, D, and E. Current literature demonstrates that there is clinical viability of a low-FODMAP diet to successfully reduce the symptoms of patients who suffer from both endometriosis and IBS. Despite the low level of evidence, there are frequent associations between endometriosis and GI conditions in addition to the influence of different nutritional factors on the disease. There is also evidence that the adaptation of individualized dietary changes yields statistically significant improvements in endometriosis-related symptoms [124]. Thus, there may be great benefit to including a dietician in the management of these patients, especially at younger ages and in early stages. The management of endometriosis requires a holistic approach focused on reducing overall inflammation, increasing detoxification, and attenuating troublesome symptoms. Inarguably, further research with a more extensive focus is needed.








