
Rotational atherectomy (RA) is a well-established treatment modality targeting calcified lesions [1]. Importantly, it is contraindicated if a coronary dissection occurs, since RA may cause its exacerbation and even a catastrophic coronary perforation. In such instances, alternative strategies should be considered. Herein, we present a patient who underwent intravascular lithotripsy (IVL) as a bail-out strategy due to an iatrogenic coronary dissection precluding the initially planned RA.
A 69-year-old male patient was referred for an intravascular ultrasound (IVUS)-guided percutaneous coronary intervention (PCI) of a calcified right coronary artery (RCA) lesion following an unsuccessful attempt in a tertiary centre (due to an uncrossable calcified lesion). Twelve years earlier he had undergone PCI of the RCA (third segment) with implantation of a bare metal stent (BMS).
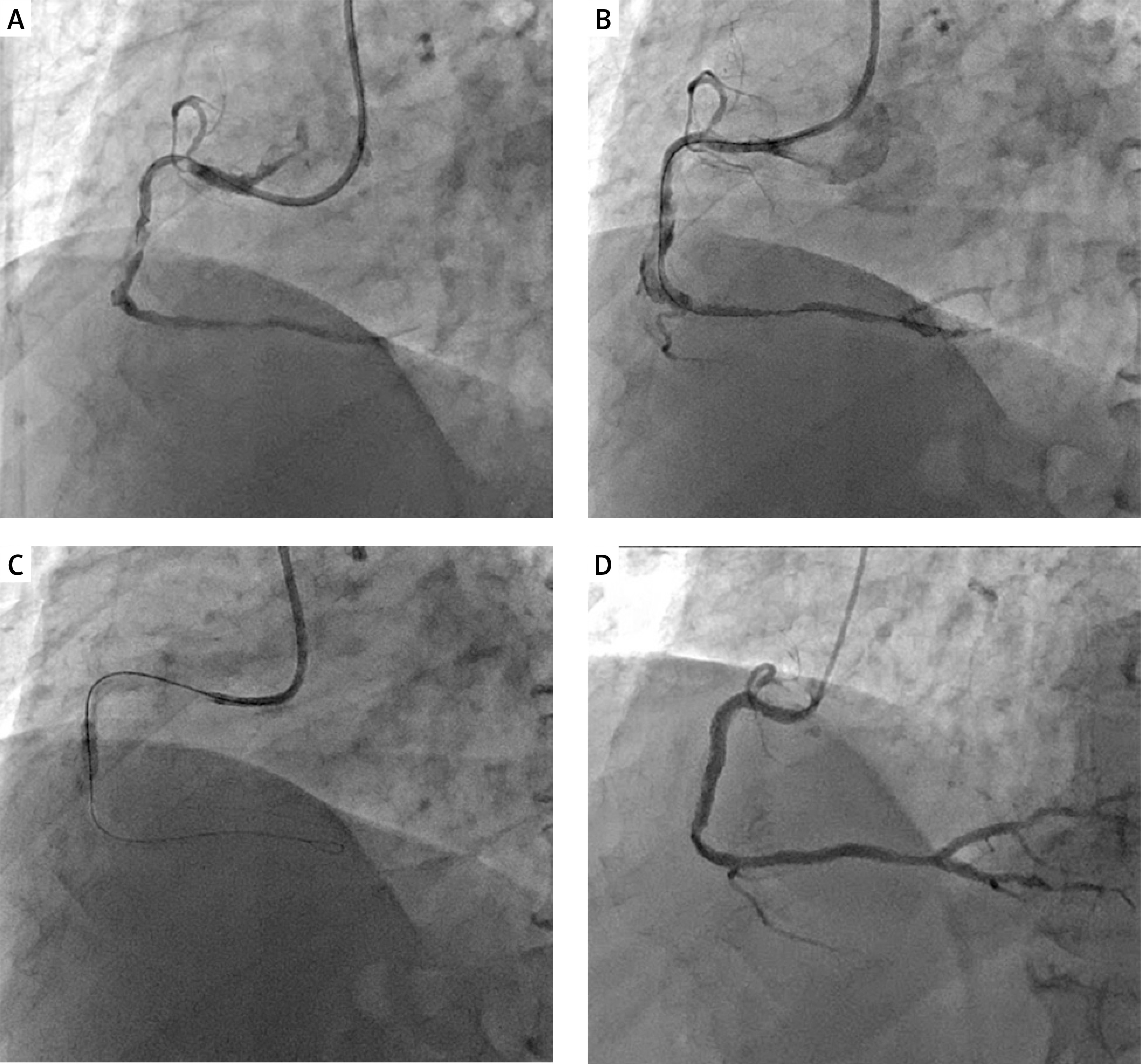
The patient’s coronary angiography revealed a subtotal lesion in the second segment and 85–90% lesion in the third segment of the RCA. Given the calcified uncrossable lesion, a decision was made to use RA. A 7-French EBU guiding catheter was used and a Fielder XT coronary guidewire was advanced into the distal portion of the RCA (Figure 1 A). An attempt to introduce a Caravel microcatheter in order to further exchange the coronary guidewire for a RotaWire was unsuccessful. The microcatheter became lodged in the second segment of the vessel, and a subsequent contrast injection revealed a massive coronary dissection, which precluded performing RA (Figure 1 B). Following several predilatations within the second segment of the vessel (escalating balloon inflations: MINI TREK 1.2/15.0 mm, MINI TREK 1.5/12.0 mm, MINI TREK 2.0/15.0, Accuforce 2.0/20.0 mm, NC Emerge 3.0/15.0), 80 intravascular lithotripsy (IVL) pulses were delivered (Shockwave 4.0/12.0 mm balloon sized 1 : 1 to the target vessel to avoid its rupture or dissection propagation) (60 pulses in the second segment – Figure 1 C, and 20 pulses focused on the border between the first and the second segment). Then, using an “anchor-balloon technique”, a Guidion Hydro guide extension catheter was advanced into the second segment of the RCA. Subsequently, following predilatations in the third segment (balloon NC Emerge 3.5/15.0 mm, 17 atm), an Ultimaster Tansei 3.5/24.0 mm stent was implanted (15 atm) and postdilated with an NC Emerge 3.75/12.0 mm balloon (21 atm). Finally, an Ultimaster Tansei 4.0/38.0 mm stent was implanted (15 atm) into the second segment of the RCA. The stent was postdilated with an NC Emerge 4.0/12.0 mm (25 atm) and, following IVUS evaluation, optimized with an NC Emerge 4.5/8.0 mm balloon (19 atm) (Figure 1 D). The further hospital stay was uneventful and the patient was discharged 2 days following the procedure.
Figure 1
A – Baseline coronary angiography demonstrating calcified lesions in the right coronary artery; B – A massive wire-induced dissection in the second segment of the right coronary artery; C – Delivery of shockwave pulses at the level of the coronary dissection; D – Final angiographic result following implantation of two drug-eluting stents
The present case demonstrates the potential role of IVL as a bail-out strategy in patients who become unamenable for RA due to an extensive wire-induced coronary dissection. The latter was an exclusion criterion in landmark Disrupt CAD studies confirming the effectiveness of IVL in calcified de novo lesions. However, since IVL disrupts calcium and preserve the integrity of soft tissues, we posit that theoretical IVL-related risk in such a clinical scenario may be the same as for regular balloons [2]. This may expand the array of off-label indications for this particular treatment modality already described in the literature, e.g. in the COIL registry evaluating IVL in stent failure patients [3, 4].







