
A 62-year old man with paroxysmal atrial fibrillation (AF), CHA2DS2-VASc score 6 and HAS-BLED score 4, with a history of multiple strokes in the right cerebral hemisphere, previous subdural bleeding and subdural hematoma during oral anticoagulation (OAC) requiring surgical craniotomy underwent uneventful atrial appendage occlusion (LAAO) with a LARIAT device (SentreHEART Inc, Redwood, CA) and was discharged home with aspirin monotherapy.
Two and half months later, another ischemic stroke was confirmed by brain computed tomography (CT). No critical stenosis of carotid and vertebral arteries was confirmed by duplex ultrasound (DUS).
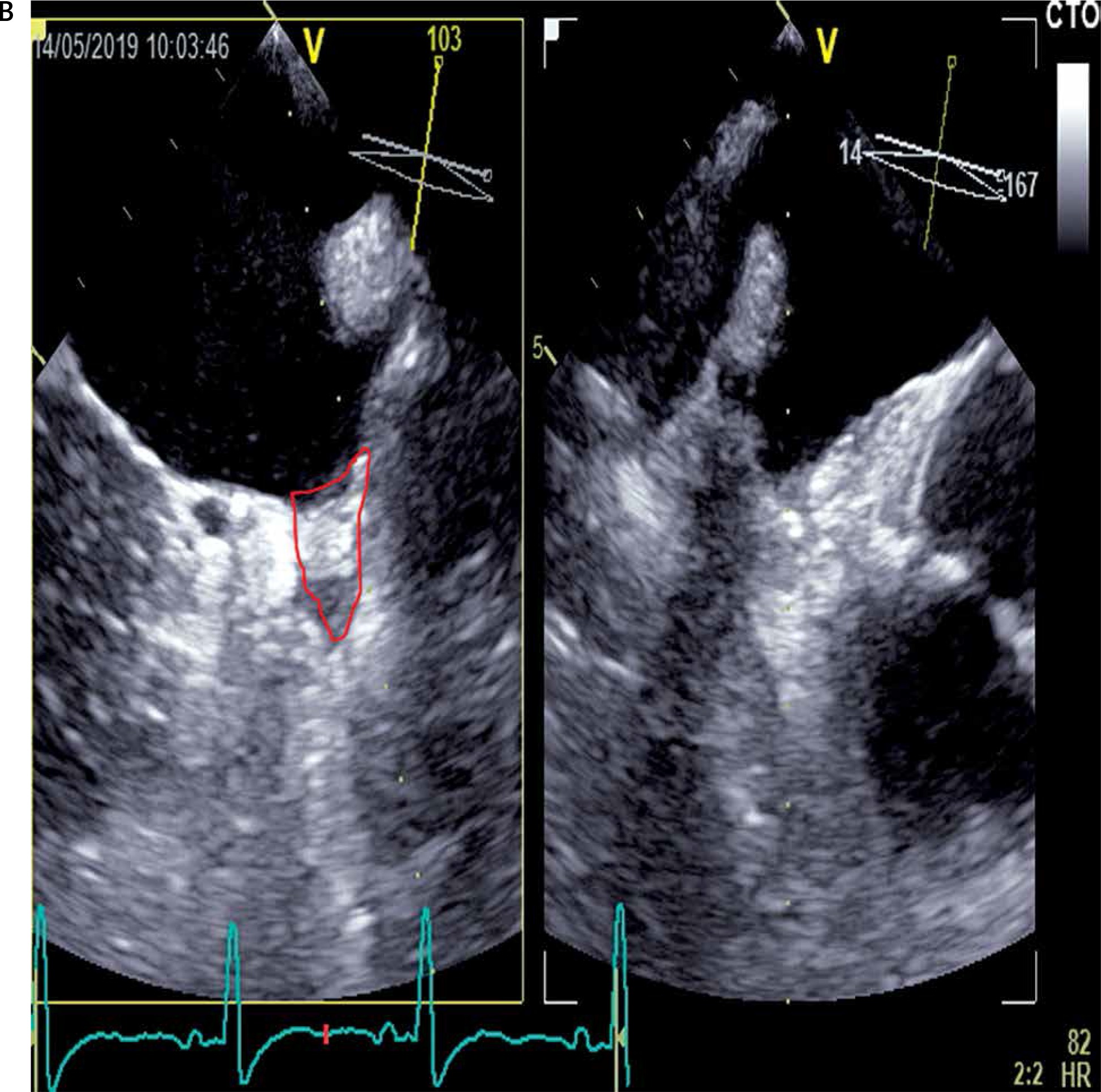
Transesophageal echocardiography with contrast was performed to evaluate the heart as a potential source of thrombus. The LAA was fully closed with no signs of recanalization and no thrombus formation was found in the LA, LAA neck (stump), or any other heart chambers (Figure 1 B).
Figure 1A
Computed tomography angiogram of the carotid arteries – a short (5 mm) critical stenosis (arrow)
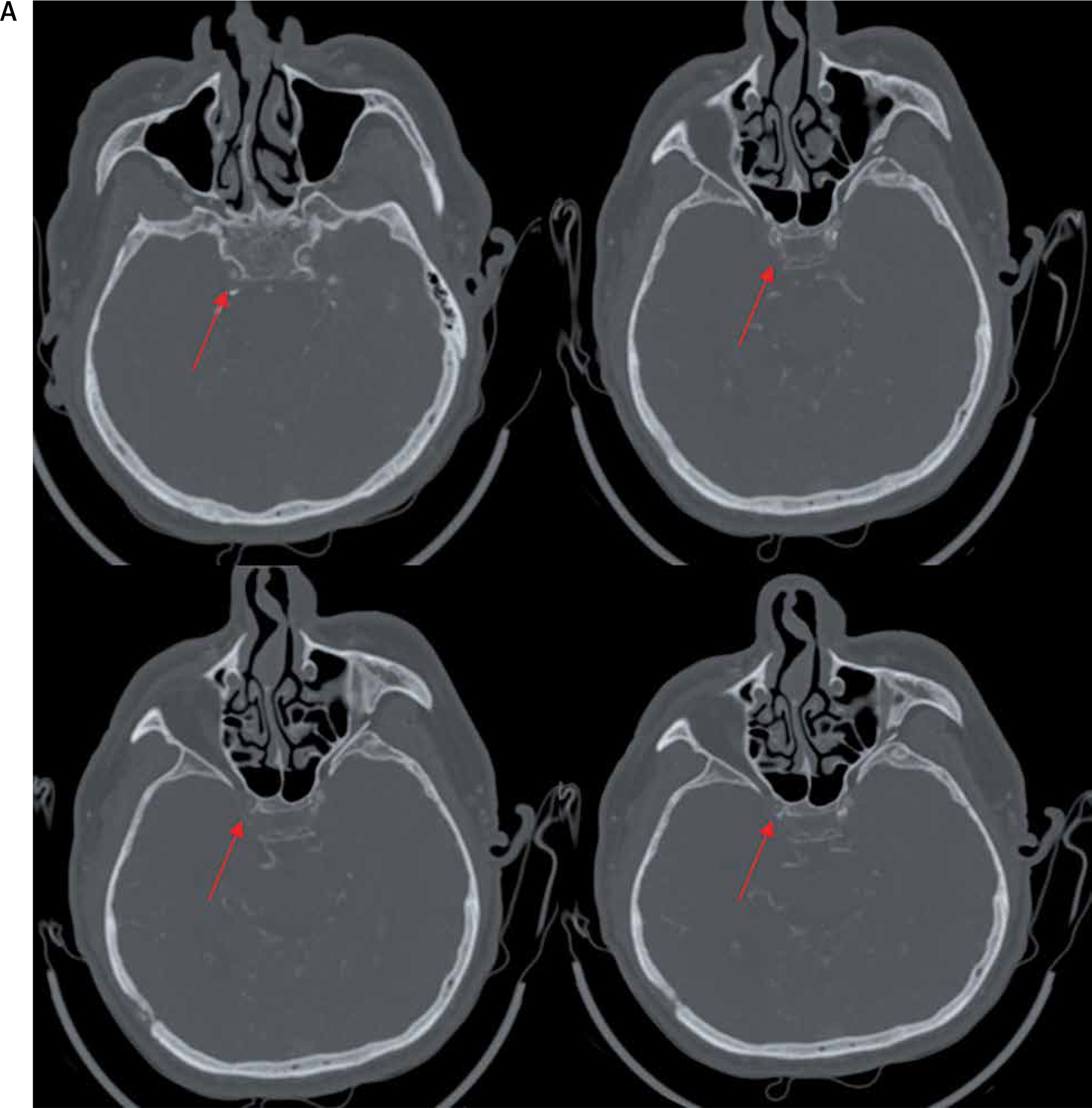
Figure 1B
Complete LAA closed with no signs of recanalization (red line - LAA stump). No signs of thrombus formation in LA
Despite the multiple negative ultrasound evaluations in the past, CT angiogram of the carotid arteries was done. A short (5 mm) critical stenosis not visible in ultrasound in the intracranial right internal carotid artery (RICA) was found (Figure 1 A). Additionally, coagulation marker examination showed increased clot lysis time (CLT) of 121 min, reduced clot permeability (Ks) of 6.3 × 10–9 cm2, elevated platelet count of 621 × 103/µl and a high fibrinogen level of 6.2 g/l.
In patients with intracranial stenosis aggressive medical treatment is superior to stenting [1]. However, in our case, due to the history of recurrent cerebral bleeding that caused neurological dysfunction and the current high HAS-BLED score, only aspirin monotherapy was continued and the patient was qualified for elective carotid artery stenting.
LAAO is very effective in the reduction of stroke risk in patients with non-valvular AF. Unfortunately, LAAO does not eliminate the thromboembolic risk completely [2]. Thrombus formation can take place in other heart chambers, and coagulation disorders can play a significant role in this process [3]. In contrast to endocardial devices, epicardial occlusion with a LARIAT device leaves no foreign thrombogenic material in the bloodstream and quick epithelialization occurs [4]. In our patient, the LAA was fully closed with no signs of recanalization, and due to negative duplex ultrasound of carotid and vertebral arteries he could be categorized as a low-risk patient. So, why did this patient develop another stroke?
The tests performed just after the stroke excluded heart, as well as carotid and vertebral arteries as the source of thrombus. However, the performance of DUS can be highly variable depending on the operator’s experience and lesion localization. Because of intracranial localization of RICA stenosis multiple DUS examinations were negative. Due to the similar location of all the strokes and an increased prothrombotic state, CT angiography was performed, confirming the presence of a critical stenosis in the intracranial RICA on a relatively short lesion. Importantly, carotid CT angiography after a negative duplex ultrasound, as well as coagulation profile assessment, is not routinely performed in patients scheduled for LAAO. Thus, in our opinion, a more detailed coagulation profile and CT scan evaluations might be justified in selected LAAO candidates, especially in cases of stroke recurrence after successful LAA occlusion.







