
Introduction
Juvenile xanthogranuloma (JXG) is a rare non-Langerhans cell disorder [1], which is predominantly diagnosed during the first year of life or is present at birth [2, 3]. It is slightly more frequent in males [3]. Typically JXG involves the skin; however, systemic lesions may rarely appear (3.9–5%) [4]. Herein we present a case of a 13-year-old girl with isolated bronchial JXG.
Case report
Herein we present a case of a 13-year-old girl who was admitted to the Department of Paediatric Surgery, Traumatology, and Urology in Poznan. She reported chest discomfort, difficulty breathing, and a cough. A month prior to admission she had suffered from a respiratory tract infection. She was delivered at term as a firstborn child with an Apgar score of 10 and a normal birthweight of 3360 g. At the age of three years, she was diagnosed with erythrocyturia. Clinical examination on admission revealed pallor, left side rib prominence, and diminished vesicular breath sounds on the left (from base to shoulder blade angle). X-ray showed atelectasis of a large part of the superior left lobe and obstruction of the bronchus leading to the third segment of the left lung (Fig. 1).
Fig. 1
X-ray showed atelectasis of almost the whole left lung superior lobe and obstruction of the bronchus leading to the third segment of the left lung

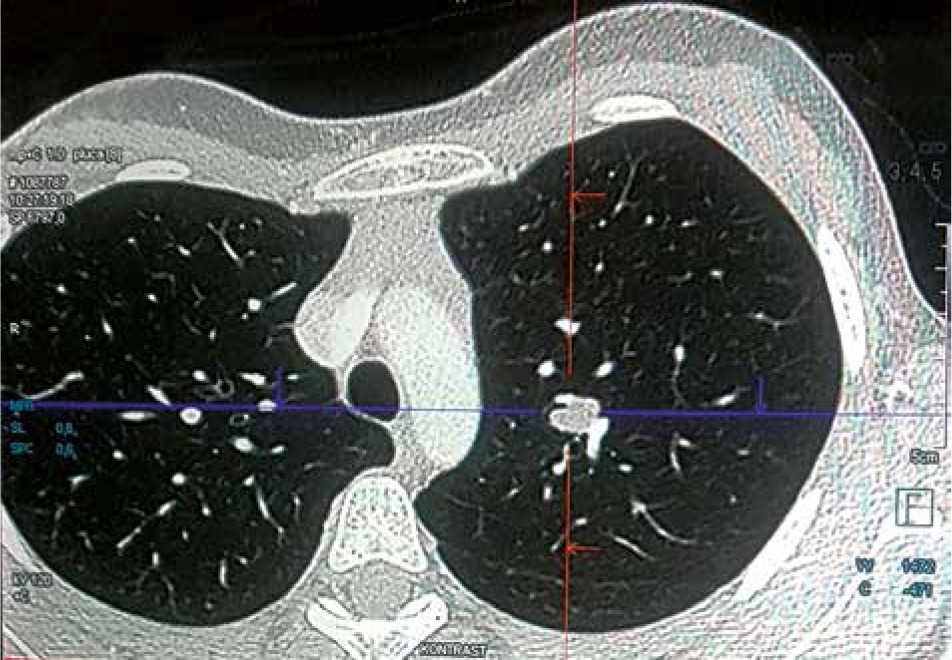
Computed tomography indicated a soft tissue lesion within the bronchus (Fig. 2).
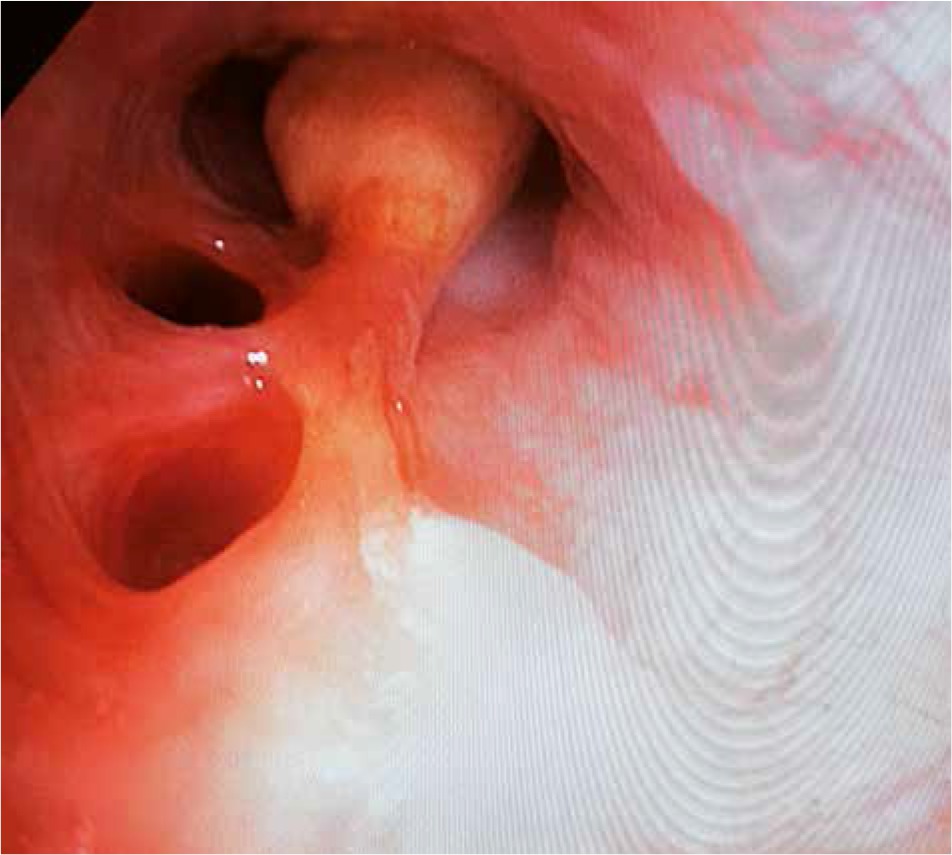
Bronchoscopy was performed, which revealed a pathological mass filling the left main bronchus (Fig. 3).
Despite the initial recanalisation of only the inferior lobar bronchus, the condition of the patient improved, and a week later the procedure was repeated to clear the superior lobar bronchus. Histopathological examination of the mass indicated an inflammatory myofibroblastic tumour. In the following two months, the tumour recurred and caused symptoms of breathing difficulty. Seven subsequent bronchoscopic decongestions were performed. Due to recurrence, a tissue biopsy was repeated and a second pathomorphological centre was involved in the histopathological interpretation of the biopsy sample. Cytomorphology showed typical Touton cells, and immunohistochemistry was negative for CD1a, s-100, and langerin and positive for CD163. With these results, the patient was diagnosed with juvenile xanthogranuloma. She was referred to an oncological centre for consideration of systemic chemotherapeutic treatment with vinblastine or cytarabine. The patient did not undergo chemotherapy due to the risk of adverse effects, and because the pathological mass was of a stable diameter. The tumour will be monitored, and chemotherapy considered at each future evaluation.
Discussion
Juvenile xanthogranuloma is a form of non-Langerhans cell histiocytosis that predominantly affects the skin (Table 1) [5]. The most common JXG manifestation is solitary or multifocal papular nodules varying from yellow through red to brown in colour. They mostly occur on the head and neck, but the trunk and extremities may be affected as well. JXG rarely manifests in extracutaneous locations (5%). The most frequent site is the eye (0.3–0.5%) [2, 3, 6]. Extracutaneous JXG lesions have been described in the lung, intestines, liver, spleen, adrenal gland, gonads, central nervous system, bone marrow, and kidney [2, 6]. The coexistence of cutaneous and extracutaneous lesions occurs in fewer than 50% of patients [2].
Table 1
Classification of the cell histiocytosis (group C and L, according to [5])
Pulmonary JXG lesions are extremely rare. They are usually multifocal, localised in the pulmonary parenchyma, and accompanied by other cutaneous and extracutaneous lesions. Pulmonary JXG tumours can present as pneumonia, haemoptysis, or airway obstruction, but they can also be asymptomatic [2, 6, 7]. Dehner recorded a three-year-old boy with pneumonia caused by a JXG lesion in the bronchus without skin manifestations, similar to our patient [6]. Biopsy and histopathological examination with immunohistochemistry of JXG are not generally required due to characteristic clinical presentation. However, they are useful in confirmation of diagnosis and differentiation of cell type and immunohistochemistry. Histopathological features of JXG include the presence of Touton cells and infiltrates of dermal histiocytes. Touton giant cells are multinucleated and characterised by peripherally located eosinophilic cytoplasm. They may be present in up to 85% of cases with skin manifestation but are a less common finding in extracutaneous sites [3, 6, 8]. In immunohistochemistry, JXG is marked by the positivity of marker factor XIIIa, CD163, CD68, CD14, or vimentin and the negativity of CD1a or S-100 protein [3, 6, 8]. According to Kraus et al., neither the presence of S-100 nor the absence of XIIIa precludes the diagnosis [9]. Recent studies have reported BRAF and MAP2K1 gene mutations in the course of JXG [10]. In our case, molecular diagnostics have not been performed yet.
Cutaneous lesions are generally benign, self-limiting, and regress spontaneously, and therefore usually do not require treatment. Management of pulmonary JXG depends on several factors. A surgical approach is indicated for lesions with severe symptoms, precarious location, and uncertain histopathological diagnosis at the time of operation. Large extracutaneous lesions can spontaneously regress, but extracutaneous JXG without skin presentation are usually surgically resected [2, 7]. Systemic treatment with vinblastine, prednisone, and methotrexate is reserved for patients with symptomatic JXG or involvement of the central nervous system [8]. Cauro et al. reported a case of a 13-month-old child with cerebellar and pulmonary JXG. Regression of pulmonary lesions after administration of chemotherapy with vinblastine was observed [11]. Maeda et al. described the use of both vinblastine and cytarabine in the treatment of pulmonary JXG lesions [10].
Conclusions
The clinical manifestation of JXG depends on the location of the tumour, which may be multifocal, involving both the skin and extracutaneous tissues. Isolated pulmonary JXG is an extremely rare finding, which requires correct diagnosis and careful planning of therapeutic treatment. Due to the low number of cases and lack of guidelines, it can be difficult to choose the best treatment option. Management of JXG should be based on the child’s age, lesion location, and clinical manifestations. Severe pulmonary symptoms, inconclusive histopathological examination, risk of malignancy, and large tumour size are indications for radical surgical resection of the tumour. Non-surgical treatment with chemotherapy is useful in cases of inoperable tumours. However, it is crucial to consider the advantages and disadvantages of both methods. More comparative studies are required to investigate management strategies.






