
Introduction
Menopause is a natural biological transition marking the permanent cessation of menstruation and the end of a woman’s reproductive life [1]. Globally, most women experience menopause between the ages of 45 and 55, with a mean age of approximately 50 years [2]. This transition is accompanied by a wide spectrum of physiological and psychological changes that can affect quality of life and overall well-being. Common symptoms include vasomotor disturbances such as hot flashes and night sweats, sleep problems, mood changes, and urogenital complaints, which may interfere with daily functioning, interpersonal relationships, and work productivity [3]. International research has shown that women with limited knowledge or negative attitudes towards menopause are less prepared to manage these symptoms and may be less likely to seek medical advice [4].
Despite growing global attention to midlife women’s health, substantial regional disparities persist. In many Asian societies, menopause remains a sensitive and often neglected topic [5, 6]. Cultural beliefs, societal taboos, and limited access to reliable information may contribute to misconceptions and delayed health-seeking behaviours. Vietnam shares several of these cultural characteristics with neighbouring countries, where menopause is often considered a private topic, leading to gaps in communication and insufficient education [7].
Female health workers, who represent the majority of staff in maternity hospitals, are themselves approaching or experiencing menopause. Their understanding and attitudes towards this transition not only affect their personal well-being but also influence their ability to counsel patients and raise community awareness. Although some studies have shown that even healthcare professionals may lack adequate training on menopause [8], evidence from Southeast Asia – and from Vietnam in particular – remains limited. This scarcity of data constrains the development of evidence-based interventions to support women in the workforce and improve the quality of menopause-related patient care. Despite their central role in reproductive health services, there is still a notable absence of research examining menopause-related knowledge, attitude, practice (KAP) among health workers in Vietnam.
The knowledge, attitude, practice model has been widely applied in public health to explain how awareness and perceptions influence behaviours [9]. Applying this model to female health workers provides an opportunity to identify educational gaps, inform workplace policies, and support interventions that enhance both staff well-being and patient care.
Therefore, this study aimed to evaluate KAP regarding menopause among female health workers at Hung Vuong Hospital – a tertiary obstetrics and gynaecology hospital in Vietnam – and to explore factors associated with these outcomes. Generating such evidence is essential for developing tailored training programs and improving support mechanisms for this workforce, with implications for similar settings globally.
Material and methods
Study design and population
This descriptive cross-sectional study was conducted at Hung Vuong Hospital, Ho Chi Minh City, Vietnam, from March to June 2024. The study targeted female health workers aged 40–60 years who were employed at the hospital during the study period. The selected age range aligns with the STRAW+10 staging system and global epidemiological evidence, which indicate that the menopausal transition typically begins in the early to mid-40s, natural menopause occurs for most women between ages of 45 and 55, and clinically significant postmenopausal symptoms may persist into the late 50s [10]. Including women aged 40–60 therefore ensured that the study population encompassed individuals who were most likely to be approaching, experiencing, or having recently undergone menopause, consistent with international research on menopausal knowledge and attitudes.
Eligible participants included physicians, specialists, nurses, pharmacists, attendants, accountants, and other staffs who consented to take part after being fully informed about the study, and who participated in the hospital’s 2024 perimenopausal and menopausal health screening program. Exclusion criteria included non-hospital employees working under outsourced service contracts and individuals who declined to participate.
Eligible participants were invited through internal hospital announcements conducted by the research team. Those who expressed interest were directed to a private meeting room arranged for the study. Before participation, all individuals received a brief explanation of the study objectives, procedures, and confidentiality protections, after which written informed consent was obtained. Participants completed the paper-based questionnaire themselves during scheduled times. Research staff were available nearby to clarify procedural questions but did not assist with or influence questionnaire responses.
Sample size
The sample size was estimated based on a single population proportion with a 95% confidence level and a 5% margin of error. The expected proportion of correct knowledge regarding menopause was derived from the study by Pathak et al. [11], resulting in a minimum required sample size of 359 participants.
Questionnaire
The questionnaire was developed based on previous studies by Pathak et al. [11] and Saswatika et al. [12], then translated into Vietnamese and pilot-tested with 30 participants to ensure clarity and reliability. Internal consistency reliability, measured using Cronbach’s alpha, was 0.88 for knowledge, 0.72 for attitudes, and 0.81 for practices.
The final instrument consisted of 45 items, divided into two sections:
Section A: 12 questions on sociodemographic and background information,
Section B: 33 questions assessing KAP regarding perimenopause and menopause.
The knowledge domain (15 items) assessed understanding of menopausal physiology, symptoms, and management. Each correct answer was scored as one, and total scores were categorized as poor (0–5), average (6–10), or good (11–15).
The attitude domain (7 items) was scored as positive (1) or negative (0), yielding total scores classified as negative (0–3) or positive (4–7).
The practice domain (11 items) evaluated self-care and health-seeking behaviours, scored as poor (0–3), average (4–7), or good (8–11).
Data analysis
Data were entered in EpiData 3.1 and analysed using Stata 14.2. Descriptive statistics summarised baseline characteristics and KAP outcomes. Knowledge and practice scores were categorized into poor, average, and good. Attitude was classified as positive or negative. The χ2 test or Fisher’s exact test was applied to examine associations between categorical variables, and independent-sample t-tests or ANOVA were used for continuous variables where appropriate. Variables significant in bivariate analysis were entered into multivariable regression to identify independent predictors. Crude prevalence ratios (PR) and 95% CI were calculated to estimate associations. Statistical significance was set at p < 0.05.
Results
Eligibility
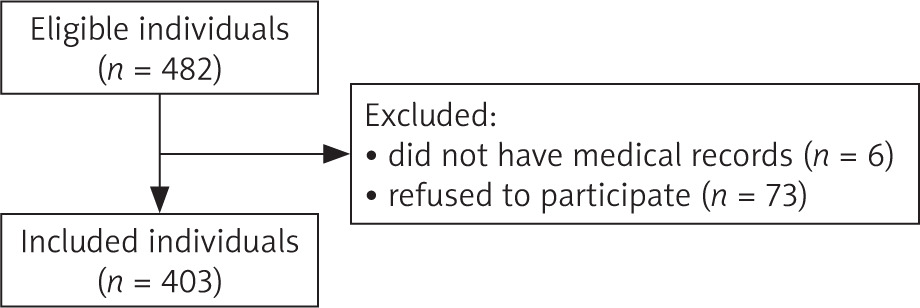
Of the 482 eligible female health workers aged 40–60 years, 79 were excluded – 6 who did not participate in the annual health screening and 73 who declined to join the study. A total of 403 participants were enrolled and completed the questionnaire (Figure 1).
Participant characteristics
Most participants worked in clinical departments (74.7%), were aged 40–45 years (57.6%), and resided in Ho Chi Minh City (98.8%). The majority held a university degree (61.0%) and were employed as nurses (65.3%). Nearly all participants were of Kinh ethnicity (97.5%) and married (79.9%), with two children (64.5%) being the most common. Most women reported no chronic medical conditions (70.2%) and were in the premenopausal stage (52.9%) (Table 1).
Table 1
General characteristics of participants (N = 403)
Knowledge about menopause
Most participants demonstrated a good understanding of menopause. They correctly identified the diagnostic criterion of 12 months without menstruation (80.7%) and acknowledged genetic influences on menopausal age (75.9%). Awareness was high regarding postmenopausal bleeding (84.9%), sexual health (83.1%), and the benefits of a healthy lifestyle (96.5%). However, misconceptions persisted – only 11.2% believed that thin women experience earlier menopause, and knowledge of hormone replacement therapy (HRT) remained moderate (64.8%). Overall, 73.5% demonstrated good knowledge, 22.8% average, and 3.7% poor (Tables 2, 3).
Table 2
Knowledge about menopause among participants
Attitudes towards menopause
Most respondents expressed positive attitudes towards menopause. Although nearly half viewed it as a loss of youth (48.6%), the majority regarded it as a natural and acceptable stage (83.1%) and not the end of sexual life (81.9%). Overall, 65.3% demonstrated positive attitudes, while 34.7% expressed negative views (Table 4).
Table 4
Attitudes of women in the perimenopausal and menopausal period
Practices related to menopause
Most participants discussed menopausal symptoms with others (79.9%) and sought medical advice when symptoms appeared (70.7%). More than half had received medical treatment (54.8%) and emphasized personal hygiene (76.4%). Regular exercise was reported by 59.8%. Healthy eating (81.4%), stress management (62.5%), and maintaining interpersonal relationships (87.6%) were common coping strategies. Overall, 39.7% showed good practices, 44.9% average, and 15.4% poor (Tables 5, 6).
Table 5
Practices of women in the perimenopausal and menopausal period
Factors associated with knowledge, attitudes, and practices
Education level was significantly associated with knowledge about menopause (p < 0.001), with higher-educated participants showing better knowledge (Table 7). No significant associations were found between attitudes and any sociodemographic or clinical characteristics (Table 8). Contraceptive use was significantly related to better practices (p = 0.026), whereas no other background factors showed associations (Table 9). Multivariable regression revealed no significant predictors of overall attitude towards menopause (Table 10).
Table 7
Association between baseline characteristics and knowledge of women in the perimenopausal-menopausal period
Table 8
Association between baseline characteristics and attitude of women in the perimenopausal-menopausal period
Table 9
Association between baseline characteristics and practice of women in the perimenopausal-menopausal period
Table 10
Multivariable analysis of factors associated with overall attitude of women in the perimenopausal-menopausal period
A significant positive relationship was found between KAP with good knowledge were 3.55 times more likely to have positive attitudes than those with poor knowledge (p = 0.015; 95% CI: 1.28–9.80) (Table 11). Similarly, those with good practices were 1.55 times more likely to have positive attitudes (p = 0.002; 95% CI: 1.18–2.04) (Table 12). Knowledge was also significantly associated with practice levels (p < 0.001) (Table 13).
Table 11
Association between knowledge and attitude of women in the perimenopausal-menopausal period
| Characteristic | Attitude, n (%) | p-value | PR (95% CI) | ||
|---|---|---|---|---|---|
| Negative | Positive | ||||
| Knowledge level | |||||
| Poor | 12 (80.0) | 3 (20.0) | 1 | ||
| Average | 42 (45.65) | 50 (54.35) | 0.057 | 2.72 (0.97–7.62) | |
| Good | 86 (29.05) | 210 (70.95) | 0.015 | 3.55 (1.28–9.8) | |
Discussion
Principal findings
This study assessed KAP regarding perimenopause and menopause among 403 female health workers aged 40–60 years at a large tertiary maternity hospital in Vietnam. There was a strong and consistent relationship among KAP regarding menopause. Most participants demonstrated good knowledge (73.5%) and positive attitudes (65.3%), whereas fewer reported good practices (39.7%). Knowledge was significantly associated with both attitude and practice: women with good knowledge were 3.55 times more likely to have a positive attitude and nearly half of them demonstrated good practice. Similarly, a positive attitude correlated strongly with better practice behaviour (PR = 1.55, p = 0.002). Overall, these findings highlight a clear KAP pathway, suggesting that improved understanding of menopause contributes to more favourable perceptions and healthier self-care behaviours among women.
The findings are consistent with previous research indicating that adequate knowledge predicts more positive perceptions and adaptive coping with menopausal symptoms. Several studies have also observed that women with higher educational attainment tend to have greater awareness and adopt healthier lifestyle modifications during the menopausal transition [13, 14].
Interpretation
Our results reinforce the conceptual model in which knowledge shapes attitude and attitude influences practice. Women who understood the physiological and emotional changes associated with menopause were more accepting of this natural life transition and more likely to adopt beneficial practices. Interestingly, the absence of significant associations between age or marital status and KAP variables implies that access to information and health education – rather than demographic background – play a pivotal role in shaping menopausal adaptation. Knowledge was generally strong on fundamental concepts; however, content gaps persisted around HRT, where awareness levels were only average. Given that HRT remains a sensitive and often misunderstood topic [15], targeted updates for health workers could improve their capacity to counsel patients and to make informed personal choices.
Attitudes are predominantly positive, though ambivalence remained. Approximately two-thirds of participants expressed positive attitudes and most did not view menopause as the end of sexual life or an unacceptable transition. Nevertheless, nearly half perceived menopause as a “loss of youth”, reflecting persistent cultural narratives and the psychological impact of menopausal symptoms, as reported in related studies [16–18]. The strong link between knowledge and attitudes observed in our data suggests that addressing these knowledge gaps could further foster positive and adaptive perceptions of menopause.
Engagement in menopausal-related practices was uneven. Many participants reported discussing symptoms with others and seeking medical advice, yet only 39.7% demonstrated good practice behaviours. Similar studies have identified barriers to seeking medical support for sexual and menopausal issues among older women [19, 20]. The observed association between knowledge and practice highlights the need for skill-based education that goes beyond awareness to promote practical, actionable self-care behaviours.
Implications for practice and future research
These findings support the development of workplace-based educational programs that simultaneously address specific knowledge gaps, strengthen behavioural skills, and equip staff with practical counselling tools. Because both knowledge and practice were associated with more positive attitudes, interventions that combine up-to-date clinical information with structured behaviour-change strategies are likely to enhance attitudes and everyday self-care behaviours.
Future research should employ longitudinal or interventional designs to evaluate the causal effect of educational programs on improving attitude and practice. In addition, multi-centre studies across different regions would also help validate and expand the current findings.
Strengths and limitations
The strengths of this study include its relatively large sample size, the use of standardized questionnaires, and the application of comprehensive statistical analyses. However, several limitations should be acknowledged. First, the cross-sectional design limits causal inference, as the observed associations cannot establish temporal relationships. Second, the reliance on self-reported data may introduce bias, particularly regarding sensitive topics such as sexual activity. Third, because the study was conducted in a single tertiary hospital, the findings may not be generalizable to women in rural areas.
Conclusions
In conclusion, most female health workers had good knowledge and positive attitudes towards menopause, though their practical behaviours were less consistent. Higher education was significantly linked to better knowledge, and both greater knowledge and more active practice correlated with more positive attitudes. Despite their professional background, notable gaps remained in awareness and application of healthy menopausal practices. Strengthening workplace-based education and support programs is essential to enhance awareness, promote self-care, and improve the quality of counselling and care for women during the menopausal transition.
Beyond the Vietnamese context, the results contribute to the growing international evidence on menopause among healthcare professionals, especially in low- and middle-income settings where formal training may be limited. Strengthening menopause-related education for healthcare workers may therefore represent a practical and globally relevant strategy for improving women’s health services across diverse cultural and healthcare environments.








