
Aortic stenosis (AS) with hypoplastic aortic annulus (HAA), recurrence after percutaneous treatment, progression to severe heart failure, and its association with significant valve insufficiency make it complex and require timely aortic valve surgery [1–3]. The Konno-Rastan (K-R) technique consists of enlarging the aortic ring, and provides an aortic annular area compatible with the current hemodynamic requirement of the patient and its subsequent development [4, 5]. It is currently considered the most effective for widening the aortic ring and the left ventricular outflow tract, constituting an enormous surgical challenge for today’s pediatric cardiac surgeon.
An 11-year-old female patient with a history of severe congenital AS and HAA was initially treated with percutaneous valvuloplasty at 3 years and aortic valve repair with commissurotomy at 6 years. She was admitted to the emergency department of our institution due to symptoms of heart failure and respiratory failure.
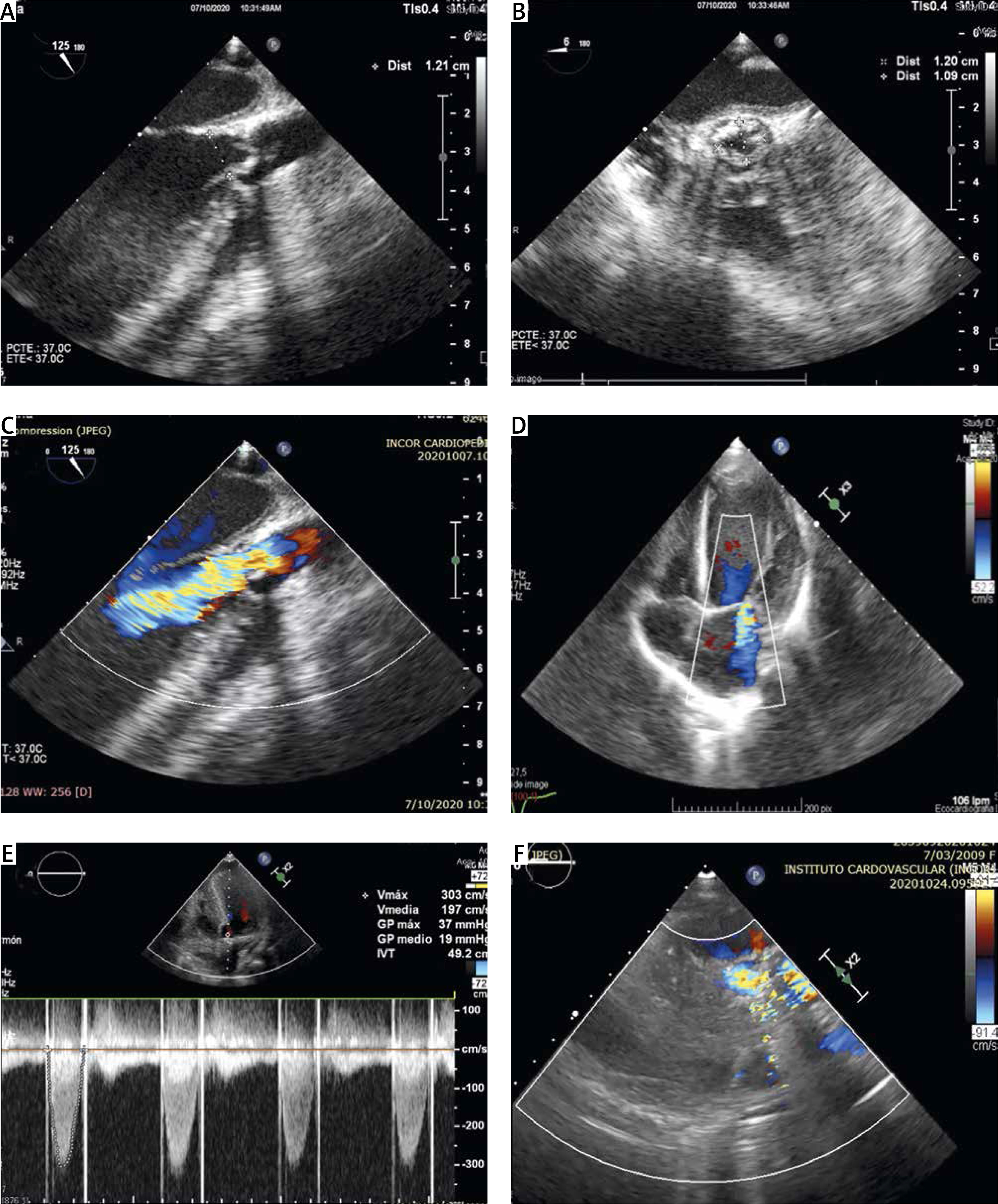
The transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) showed a double severe aortic lesion with a predominance of stenosis and recurrent HAA. The mean valve gradient was 76 mm Hg, with aortic annulus of 12 mm, and an aortic root of 18 mm (Figure 1). Likewise, the mitral valve showed severe functional insufficiency with a mitral annulus of 40 mm due to annular dilation secondary to severe growth of the left ventricle (LV) (end-diastolic diameter, 61 mm, Z-score, +4; LV ejection fraction, LVEF, 28%).
Figure 1
Preoperative and postoperative echocardiographic study. A – TEE long-axis view of the aortic root showing measurement of an HAA. B – TEE short-axis view showing a tricuspid aortic valve with thickened leaflets (*) and decreased opening. C – TEE long-axis view showing severe aortic regurgitation jet. D – Apical 4-chamber TTE view showing severe dilation of the left ventricle and severe mitral regurgitation jet. E – TTE 4-chamber apical view showing continuous wave Doppler of the aortic valve prosthesis. F – TTE parasternal long-axis view showing the adequate opening of the aortic valve prosthesis (arrow)
Due to the clinical status of the patient and the recurrence despite the 2 surgical interventions, the K-R procedure was indicated. The approach was by median re-sternotomy, with extracorporeal circulation (ECC) through central cannulation. A mitral annuloplasty was performed at the level of the posterior leaflet by suturing a band of bovine pericardium using 5-0 polypropylene sutures (Figure 2 A).
Figure 2
Mitral annuloplasty and K-R procedure. A – Posterior mitral annuloplasty with bovine pericardium patch. B – Aortotomy with right ventriculotomy extension. C – Konno incision (arrow). D – Lower part of the internal anchorage of the bovine pericardium patch on the interventricular septum E – Placement of valve sutures in the neoannulus. F – Mechanical aortic valve replacement. G – Reconstruction of the aortic root with the upper part of the inner patch. H – Reconstruction of the LVOT with an external patch
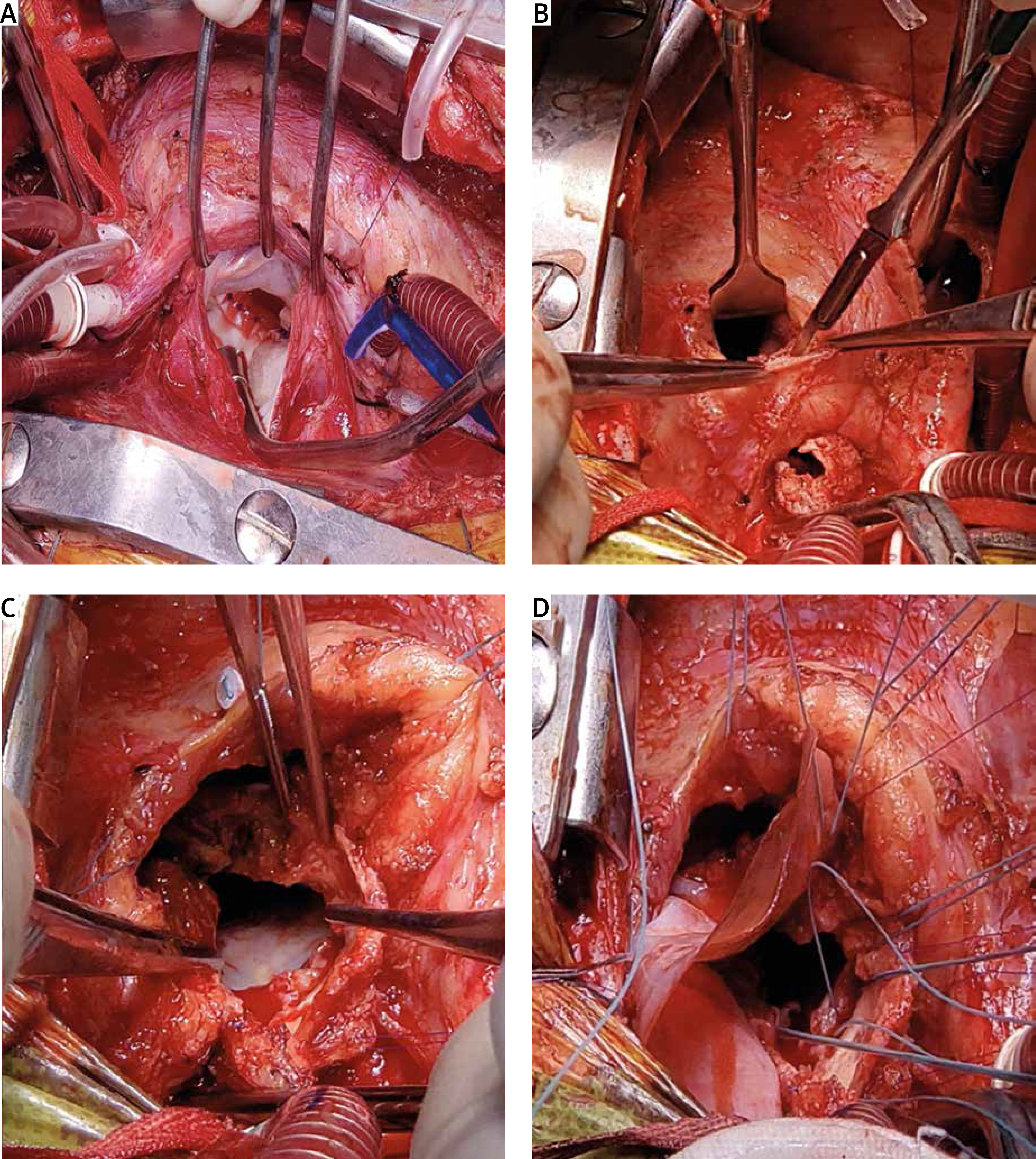
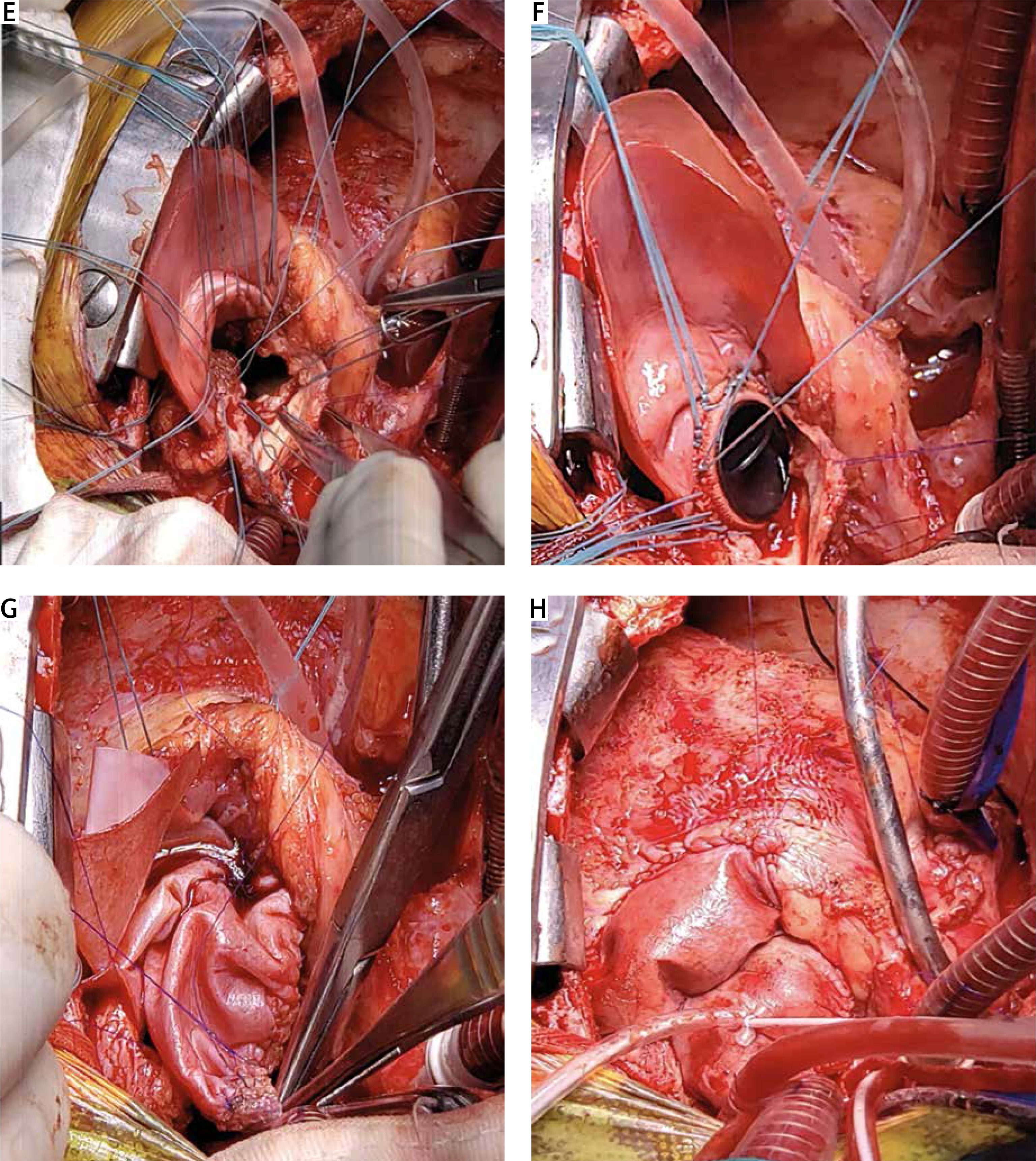
Subsequently, an aortotomy with right infundibular ventriculotomy was performed and then the Konno incision (upper third of the interventricular septum) was performed (Figures 2 B, C). The aortic leaflets were resected and a patch of the bovine pericardium was anchored over the upper edge of the Konno incision towards the aortic wall, achieving enlargement of the LV outflow tract (LVOT) (Figure 2 D). After implantation of a mechanical aortic valve prosthesis (19 mm) over the pericardial patch and the neo-annulus (Figures 2 E, F), reconstruction of the aortic root and LVOT was performed with the upper and lower part of the pericardial patch, respectively (Figures 2 G, H). The surgery proceeded without any complications, and the postoperative TEE did not reveal abnormalities (Figure 1). The postoperative course was short, and the patient was discharged with an indication of regular outpatient control.
A complex recurrent HAA, and AS are conditions constituting a serious surgical problem during valve replacement, due to the need to offer an adequate effective valve area for the patient’s requirement, and that offers a lower rate of restriction during growth [3, 5]. The implantation of an aortic valve prosthesis must offer an effective area greater than 0.85 cm2/m2, and in severe cases of HAA, annular enlargement of more than 50% of its diameter is necessary, to avoid prosthesis-patient disproportion (PPD) [6].
The K-R procedure is an effective and attractive treatment for LVOT enlargement, surgically incising the aortic root, the interventricular septum, and the anterior wall of the LVOT [5]. However, this technique has been associated with various complications such as ventricular dysfunction (18.9%), atrioventricular block (61.4%), and perioperative bleeding (26.3%) [3]. Another therapeutic alternative to consider, especially in young female patients as in our case, is the Ross-Konno procedure, a technique that replaces the aortic root with a pulmonary valve autograft [3].
Following the basic principles of the effective valve area and extrapolating them to our patient (aortic ring, 10 mm), we decided to implant a 19 mm mechanical aortic prosthesis, using the K-R procedure to double the initial annular diameter.
Various case series have shown that the K-R procedure together with aortic valve replacement provides optimal postoperative results with minimal associated mortality rates (< 1%), low mean gradient (< 10 mm Hg), and remission of NYHA IV–III symptoms to I–II [1, 3, 5]. Likewise, the safety of this technique has been highlighted with a survival greater than 85% and without deterioration of ventricular function in a 20-year follow-up (LVEF, 58–62%) [1, 2, 6].
We highlight the importance of reporting the present case due to the unusual use of the K-R technique for pediatric congenital pathologies such as complex AD and associated with HAA, and with greater emphasis on the case due to recurrence and previous surgical intervention, making its treatment a challenge for today’s cardiopediatric surgeon. Likewise, our case description is the first report of its use in a pediatric patient and with complete technical success. The diversity of pediatric congenital pathologies alone or associated requires a series of surgical strategies that seek to structurally correct the condition and that provide cardiohemodynamic conditions compatible with their requirements and that do not generate restrictions in the development of the patient.









