








Introduction
Ureteral calculi are one of the common health care problems that affect the daily life of patients [1]. Generally speaking, spontaneous passage of a ureteral stone is largely dependent on its size and location. Large proximal ureteral stones larger than 10 mm in diameter are less likely to pass spontaneously [2]. Then large proximal ureteral stones will adhere to the ureteral wall, which may cause hydronephrosis, secondary infection, ureteral polyps, and ureteral stricture [3]. Nowadays, available treatment modalities include extracorporeal shock wave lithotripsy (ESWL), ureteroscopic lithotripsy (URSL), percutaneous nephrolithotripsy (PCNL), laparoscopic ureterolithotomy (LU), and open surgery [4, 5]. However, among the various treatments for proximal ureteral stones, the optimal choice remains controversial.
ESWL is the first line treatment option for proximal ureteral stones. However, ESWL has a lower stone-free rate for large proximal ureteral stones [6]. The efficacy of URSL in the treatment of proximal ureteral stones remains controversial due to the risk of stone migration [7]. Flexible URSL, which has a high surgical success rate, has gained popularity in recent years, but this procedure requires special devices that may not be available [3]. PCNL has been reported to be the standard procedure for the treatment of kidney and proximal ureteral stones with a high stone burden, but it is associated with a high complication rate [8]. LU is increasingly used to treat large proximal ureteral stones, which has a great probability of complete stone clearance in a single attempt [9, 10].
Therefore, PCNL and LU are the most effective treatments for proximal ureteral stones, which are considered as options for failure of ESWL and URSL [11]. However, the pros and cons of the two procedures remain controversial.
Aim
The objective of this meta-analysis was to investigate the efficacy and safety of PCNL and LU in the treatment of proximal ureteral stones.
Material and methods
Search strategy
A systematic search of PubMed, Ovid and Scopus was performed to identify studies comparing LU versus PCNL for proximal ureteral stones published up to May 2022. The search strategy was “(ureteral stone OR ureteral calculi) and (laparoscopic ureterolithotomy OR percutaneous nephrolithotomy OR PCNL OR antegrade ureterorenoscopy)”. Two authors independently screened all citations to identify eligible studies.
Inclusion criteria and exclusion criteria
The included studies met the following requirements: (1) original studies comparing LU versus PCNL for proximal ureteral stones, (2) publications written in English language, (3) adult patients only.
Studies were excluded in the case of: (1) a lack of primary data (i.e. reviews, commentaries, conference abstracts), (2) insufficient data to calculate or extrapolate for the results of LU vs PCNL, (3) children patients. Discrepancy was resolved in consultation with the third reviewer.
Data extraction
Two authors independently extracted the data using a predefined data extraction form. Any discrepancy was resolved in consultation with the third researcher. The data extraction form contains the following information: baseline demographics (age, gender, stone side and stone size), surgical outcomes (operative time, length of hospital stay, initial and final stone-free rate), and complication outcomes (complications, Clavien-Dindo score ≥ 3 complications, transfusion rate, auxiliary procedures and ureteral stenosis).
Quality assessment
Two authors independently evaluated the quality of included studies according to the Oxford Centre for Evidence-based Medicine. Discrepancy was resolved in consultation with the third researcher.
Statistical analysis
A meta-analysis was conducted according to the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUORUM) guidelines [12]. Cochrane Collaboration’s Review Manager (RevMan) 5.4 software (Cochrane Collaboration, Oxford, UK) was used to analyze statistical differences. The weighted mean difference (WMD) was used for continuous variables. The odds ratio (OR) was calculated for dichotomous data. For studies presenting continuous data as means and ranges, a validated mathematical model was used to convert median (range) to mean (standard deviation) [13]. A fixed-effects model was used if no significant heterogeneity was identified; otherwise, a random-effects model was used. Statistical heterogeneity was assessed by the χ2-based Q test and I2 test. A p-value < 0.05 was considered statistically significant. Funnel plots were examined to evaluate publication bias.
Results
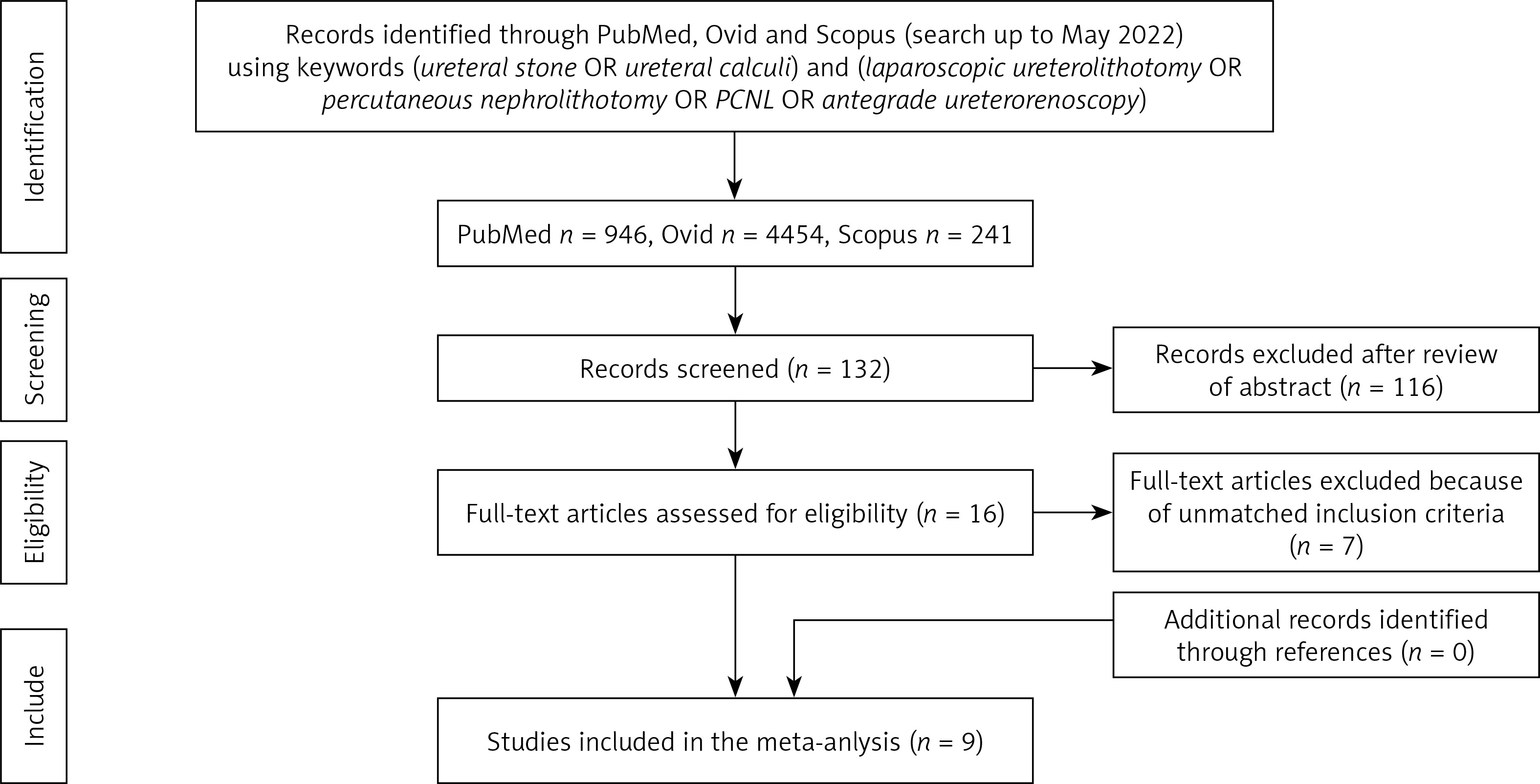
Nine studies including 933 patients (LU 465; PCNL 468) were included in this meta-analysis (Figure 1) [14–22]. The basic characteristics and quality assessment of the included studies are summarized in Table I.
Table I
Basic characteristics of included studies
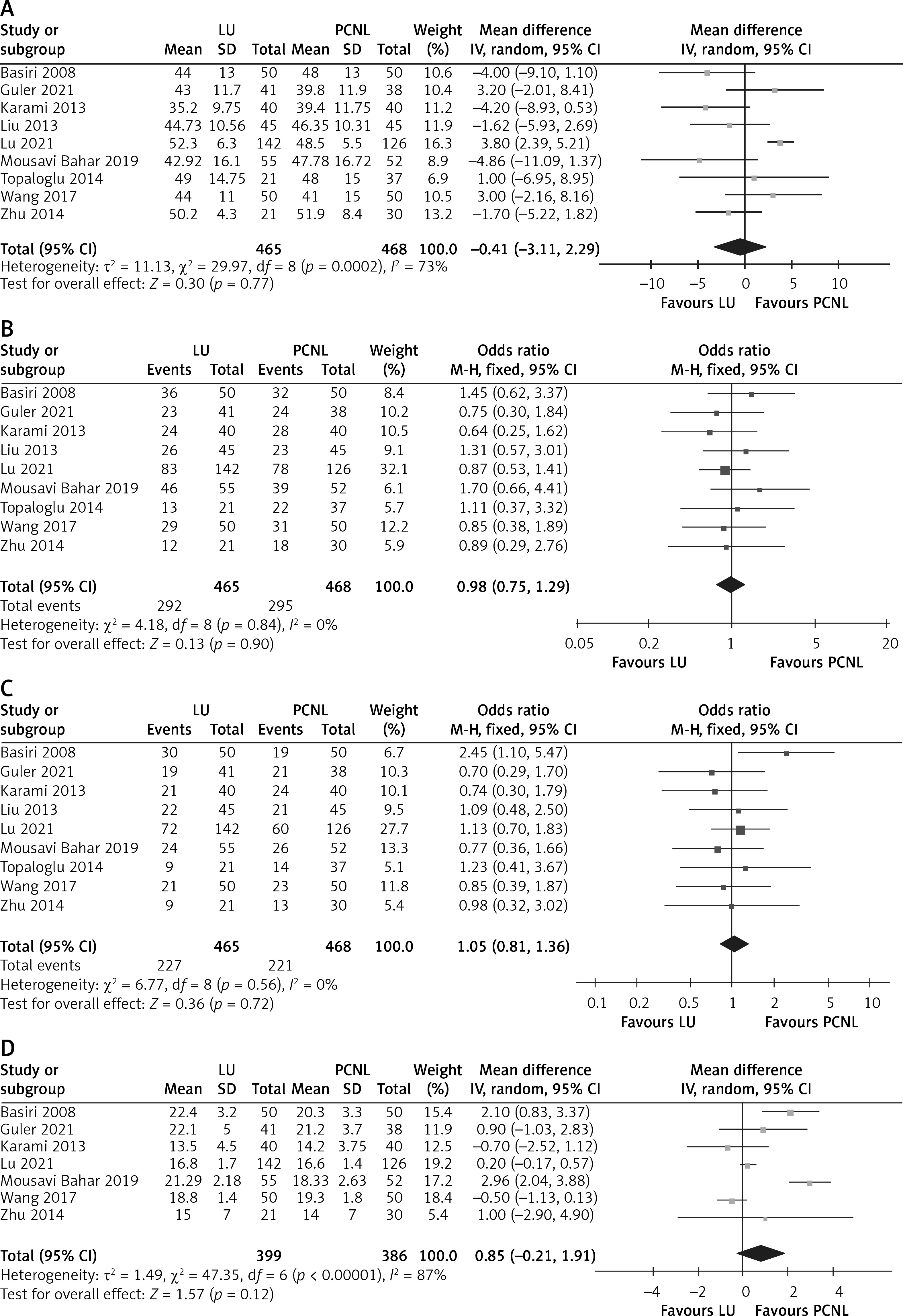
Our meta-analysis showed no significant differences in age (WMD = –0.41 years, 95% CI: –3.11 to 2.29; p = 0.77), male patients (OR = 0.98, 95% CI: 0.75 to 1.29; p = 0.90), stone side (OR = 1.05, 95% CI: 0.81 to 1.36; p = 0.72), and stone size (WMD = 0.85 mm, 95% CI: –0.21 to 1.91; p = 0.12) between LU and PCNL (Figure 2).
Figure 2
Forest plots of demographic characteristics of LU vs. PCNL for proximal ureteral stone: A – age [years], B – gender (male), C – stone side (right), D – stone size [mm]
Our data showed that LU was associated with a significantly longer operative time (WMD = 35.08 min, 95% CI: 16.29, 53.86; p = 0.0003) and a significantly higher initial stone-free rate (OR = 3.26, 95% CI: 1.45–7.31; p = 0.004). However, there was no significant difference between LU and PCNL in terms of length of hospital stay (WMD = 0.32 d, 95% CI: –0.57, 1.21; p = 0.48) or final stone-free rate (OR = 2.08, 95% CI; 0.94–4.61; p = 0.07) (Figure 3).
Figure 3
Forest plots of surgical outcomes of LU vs. PCNL for proximal ureteral stone: A – operative time [min], B – length of hospital stay [day], C – initial stone-free rate, D – final stone-free rate

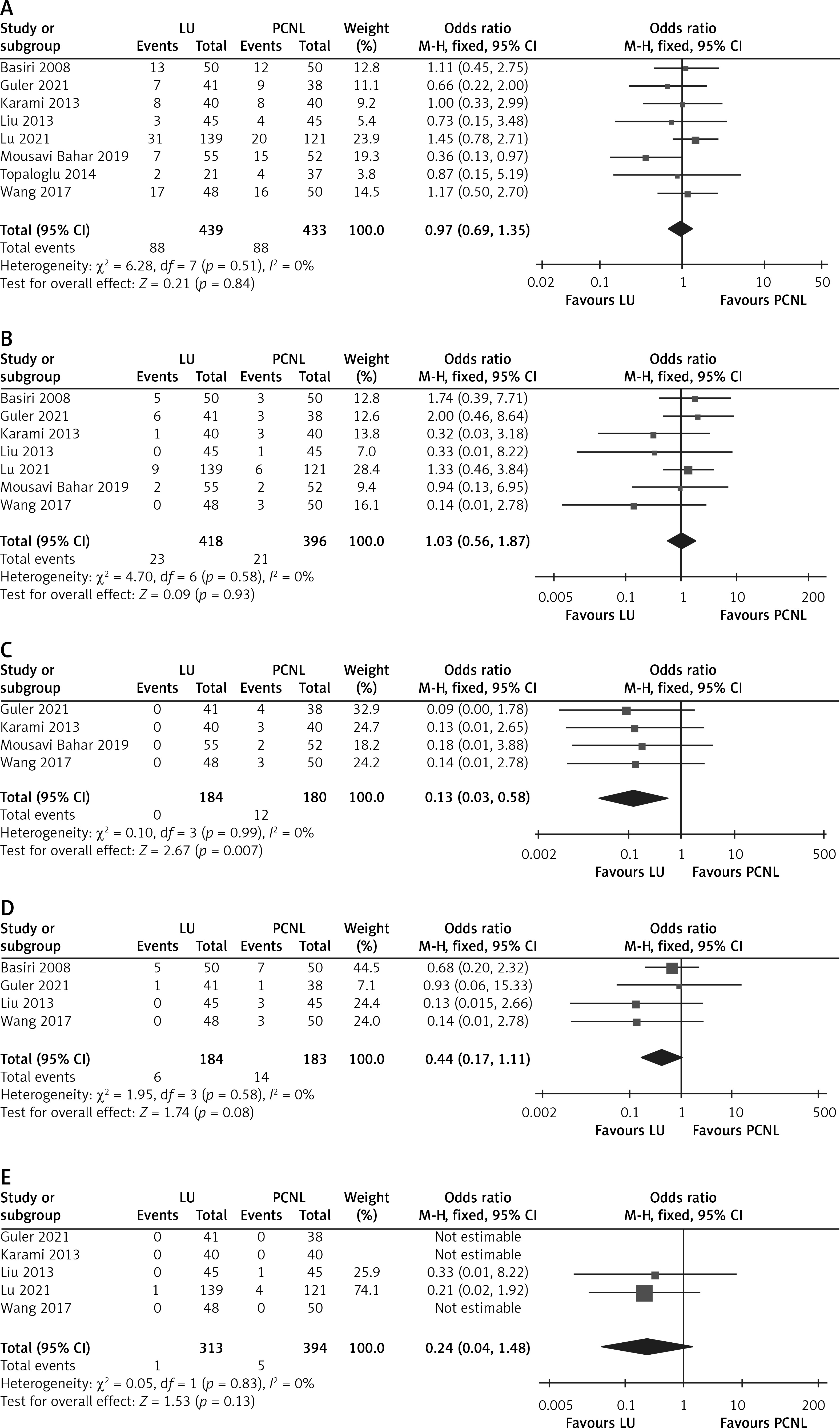
Our pooled data on postoperative complications showed that LU was associated with a significantly lower transfusion rate than PCNL (OR = 0.13, 95% CI: 0.03–0.58; p = 0.007). All the following results comparing LU with PCNL including complications (OR = 0.97, 95% CI: 0.69–1.35; p = 0.84), Clavien Dindo score ≥ 3 complications (OR = 1.03, 95% CI: 0.56–1.87; p = 0.93), auxiliary procedures (OR = 0.44, 95% CI: 0.17–1.11; p = 0.08), and ureteral stenosis (OR = 0.24, 95% CI: 0.04–1.48; p = 0.13) had no significant difference (Figure 4).
Figure 4
Forest plots of complications of LU vs. PCNL for proximal ureteral stone: A – complications, B – ClavienDindo score ≥ 3 complications, C – transfusion rate, D – auxiliary procedures, E – ureteral stenosis
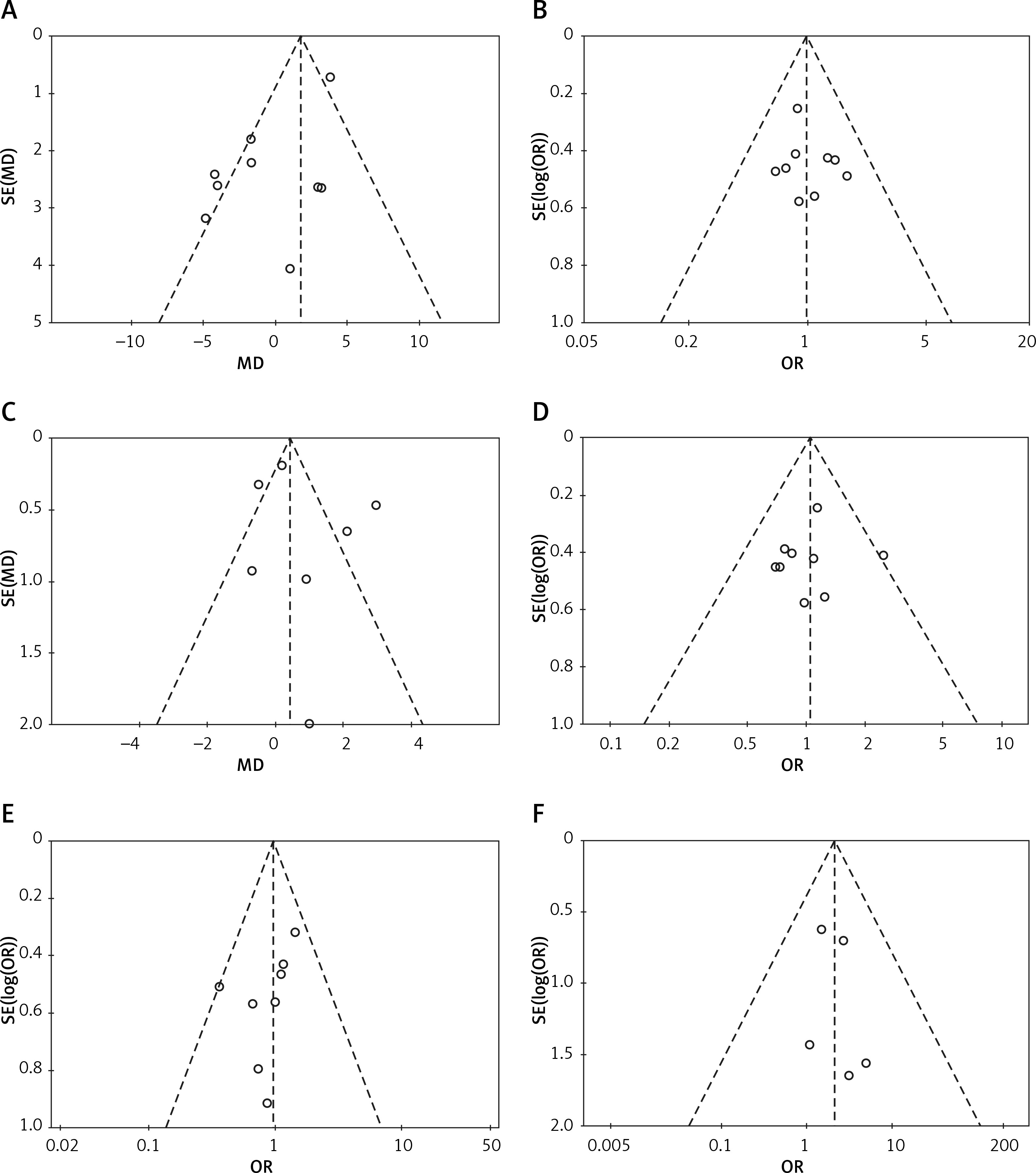
Publication bias of the included studies was assessed by funnel plots, and no palpable publication bias was noted (Figure 5).
Discussion
There are several methods available for the management of proximal ureteral stones, such as ESWL, URSL, PCNL and LU [23, 24]. The choice for proximal ureteral stones depends primarily on the stone size, hydronephrosis, infection status, cost and instruments available [25]. For proximal ureteral stones less than 10 mm, the European Association of Urology Guidelines recommend ESWL or URSL as the first line choice [26].
For proximal ureteral stones larger than 10 mm, anterograde or retrograde URSL may be preferred, and PCNL or LU is recommended for selected cases [6]. However, proximal ureteral stones may migrate upward to the kidney when treated with URSL. It is reported that both PCNL and LU are more effective than URSL or ESWL [21, 24]. However, the efficacy and safety of PCNL and LU in the treatment of proximal ureteral stones have not been fully investigated.
Nine studies reported similarities in age, gender, stone side and stone size, reflecting minor selection bias in this study. Our pooled results showed a longer operative time with LU, reflecting the complexity of LU. However, the length of hospital stay was similar in the two groups. The average length of hospital stay was 4 to 5 days, reflecting the great trauma of the two procedures. The most important surgical outcome is stone-free rate. The initial stone-free rate reflects the immediate effect of surgery. Our pooled analysis showed that the initial stone-free rate was significantly higher in LU. This result indicated that LU has high efficiency for large proximal ureteral stones, requiring less assisted or spontaneous stone passage. However, the final stone-free rate was not significantly different between the two groups. Only four studies reported the initial stone-free rate, while seven studies reported the final stone-free rate. The finial stone-free rate is an indicator that clinicians and patients are more concerned about. Our pooled results indicated that LU and PCNL can achieve the same final stone-free rate, but LU has an advantage in the initial stone-free rate. This is consistent with the results reported by Wang et al. [24].
Complications are one of the key factors limiting the application of surgery. Most studies reported complications. Our pooled analysis showed that the overall complications and the severe complications (Clavien-Dindo score ≥ 3) were comparable between LU and PCNL, revealing similar safety profiles. However, four studies reported the transfusion rate, which was significantly lower in LU than in PCNL. This is consistent with recent reports [27, 28]. The reason could be that LU may avoid percutaneous renal access injuries during PCNL [29]. Therefore, LU is a more complex procedure and PCNL is a more dangerous procedure.
Four studies reported auxiliary procedures, with no significant difference between the two groups. Considering the similar final stone-free rate and higher initial stone-free rate in LU, PCNL was more likely to have small residual stones. However, this does not affect PCNL as a high stone-free rate treatment for large proximal ureteral stones. Five studies reported ureteral stenosis, while only two studies reported postoperative ureteral stenosis. The pooled results of our study showed no significant difference between the two groups. We believe that this is closely related to the condition of stones, such as ureteral polyps, impacted stone, chronic inflammation, etc., because neither group has thermal damage.
Our study had some inherent limitations. First, half of the studies were retrospective, which limited the quality of the results. Second, the small sample size is also a limitation for the quality of this study. Third, some studies reported impacted ureteral stones, while others did not. Fourth, we did not compare the differences between transperitoneal and retroperitoneal approaches for LU. However, similar results are reported for the two approaches [30]. Fifth, the follow-up time is too short to assess the long-term effects of LU and PCNL. Last, the costs of LU and PCNL were not available from the literature.
More large randomized controlled trails are needed to evaluate the efficacy and safety of LU and PCNL in the treatment of large proximal ureteral stones.
Conclusions
This meta-analysis suggests that LU is a more complex procedure and PCNL is a more dangerous procedure. Although LU was associated with longer operative time, the incidence of blood transfusion was lower. LU may provide a safe and feasible option for large proximal ureteral stones with a higher initial stone-free rate and lower transfusion rate compared with PCNL. More randomized controlled studies are needed to confirm these results.