
A 70-year-old female with a 6-month history of surgical aortic valve replacement (SAVR) with a 19-mm Bicarbon Slimline metallic prosthesis (LivaNova PLC, Saluggia, Italy) presented with crushing chest pain. A positive troponin test combined with electrocardiographic evidence of diffuse ST depression in leads II, aVf, V3-V6 (Figure 1) and ST elevation in aVr suggested a diagnosis of non-ST elevation myocardial infarction necessitating evaluation in the cardiac catheterization laboratory in anticipation of international normalized ratio (INR) drop below 1.8 (~2.8 at admission).
Figure 1
A – Angiographic assessment prior to the aortic valve replacement indicated absence of the disease in the left coronary system. B – The Bicarbon Slimline LivaNova metallic prosthesis. C – Ostial left main sub-total occlusion. D – Patent saphenous vein graft to the distal right coronary artery. E – Proximal optimization technique following stent deployment to optimize apposition/positioning in the proximal left main segment. F – Final angiographic result obtained
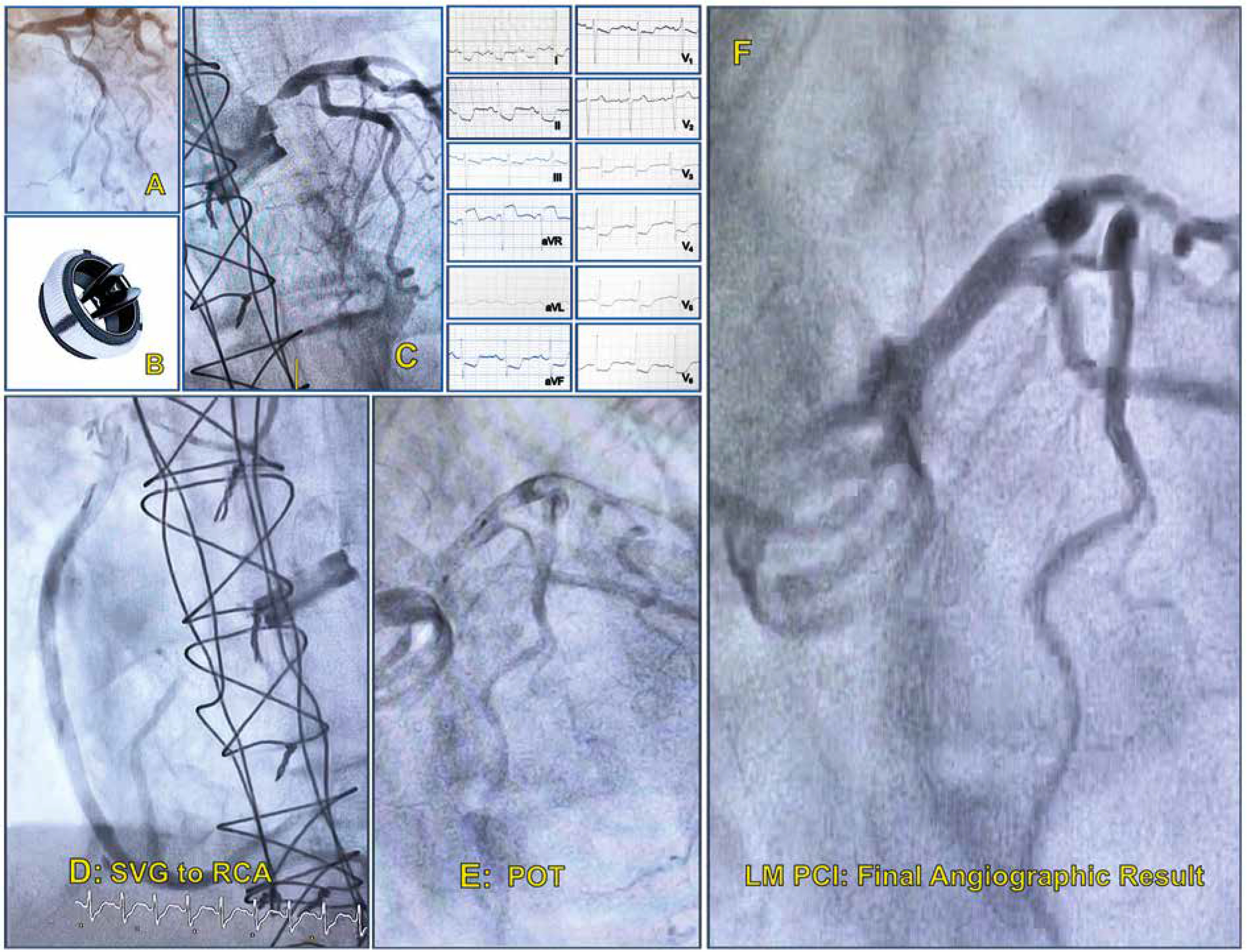
The aforementioned plan was aborted as the patient experienced cardiac arrest shortly after admission and was urgently transferred to the catheterization laboratory following successful resuscitation and intubation. Angiographic evaluation through the right trans-radial access demonstrated ostial left main (LM) sub-total occlusion (Figure 1 C) and patent saphenous vein graft to the distal right coronary artery (RCA) (Figure 1 D). Interestingly, angiographic evaluation performed prior to AVR indicated absence of the disease in the left coronary system and 60% mid-RCA disease that was revascularized with a vein graft (Figure 1 A).
LM engagement was managed with a JL 4.0 6F guide catheter and the ostial lesion was crossed with a BMW guidewire (Abbott Vascular, Santa Clara, USA). Predilatations were performed with 3.0 × 15 mm compliant balloon and a Xience Pro 3.5 × 15 mm (Abbott Vascular, Santa Clara, USA) drug-eluting stent was deployed. Following successful stent deployment, proximal optimization (Figure 1 E) was performed with a 4.0 × 15 mm non-compliant balloon at high atmospheres delivering an excellent angiographic result (Figure 1 F).
The etiology of LM critical stenosis following SAVR involves 1) accelerated fibrous tissue growth secondary to turbulent flow induced by the aortic prosthesis [1] and 2) exaggerated tissue response subsequent to micro-injuries induced by catheters during cardioplegia administration [2]. Pathology studies have indicated the absence of tunica adventitia in the ostium of LM resulting in higher elastic recoil (abundance of smooth muscle cells and elastic tissue compared to the trilaminar anatomy of the main and the distal part) when catheter-induced micro-injuries occur [3].
It is noteworthy that in the present case, only cardioplegia CUSTODIOL® HTK Solution was given retrogradely. This fact cannot explain the mechanism of the left main stem lesion. It should be noted, of course, that the 60% RCA lesion became 100% after 6 months of treatment with antiplatelet and anticoagulant medication. This fact cannot explain the mechanism of stem damage.
The treatment following LM critical stenosis is either reoperation with coronary artery bypass grafting associated with increased mortality rate in the range of 25% or percutaneous coronary intervention (PCI). LM PCI is a challenging operation performed by experienced high-volume operators with at least 15 LM PCIs per year for at least 3 consecutive years delivering excellent results [4]. Our patient was treated successfully with PCI and was extubated 4 days later without any neurologic deficit. The patient was discharged 10 days after admission with proper medication.
In conclusion, ostial coronary critical stenosis should be anticipated in patients who develop ischemic cardiac events 3–6 months after SAVR. Careful manipulation of cardioplegia catheters and aortic root minimize the risk of fibrous tissue generation in this anatomic area. PCI is considered the treatment of choice when operators have significant volumes in such cases.









