
Introduction
Primary hyperparathyroidism (PHP) is a common endocrine disease, caused by long-term autonomous and inappropriate excessive production of parathyroid hormone (PTH), by one or more hyperfunctioning parathyroid glands, with the main metabolic consequence of hypercalcemia. It is related in 10–20% of cases to hyperplasia of glands, in 1% to a parathyroid carcinoma and in 80% of cases to a parathyroid adenoma [1]. In 15–20% of cases, the latter is ectopic, due to an aberrant embryological migration [2]. The most frequent ectopic locations of parathyroid glands are intra-thyroid, para-tracheal and retroesophageal. The mediastinal site is less frequent and accounts for 10–15% of ectopic parathyroid adenomas [3]. A mediastinal parathyroid gland is defined as a parathyroid lying completely below the level of the clavicle.
Aim
Our study reports the management of 21 cases of mediastinal parathyroid adenoma (MPA). The objectives of this study were to determine the clinical manifestation of MPA, to analyze the imaging methods performed, and finally to describe the therapeutic approach for our patients.
Material and methods
This is a descriptive and retrospective study, based on documented cases of MPA, during the period from January 2010 to December 2019 at the Thoracic Surgery Department of the Mohammed V Military Training Hospital in Rabat. The patients included in our study had pathological confirmation of MPA after surgery.
Results
Patients ranged in age from 20 to 69 years, with a mean age of 45 years. There was no gender predominance. The medical history was dominated by arterial hypertension in 23.8% (n = 5/21), renal lithiasis in 14.28% (n = 3/21), thyroidectomy in 9.5% (n = 2/21), diabetes in 14.2% (n = 3/21), cardiac disease in 9.5% (n = 2/21), and end-stage renal disease in 4.2% (n = 1/21); it is also noted that 6 patients did not have any notable history. The frequently reported manifestations were mainly osteoarticular with bone pain in 52.3% (n = 11/21), multiple fractures in 28.5% (n = 6/21) and osteoporosis in 14.2% (n = 3/21). Preoperative parathyroid hormone (PTH) and blood calcium values of our patients revealed significantly elevated PTH and hypercalcemia with a mean of 541 pg/ml and 133.1 mg/l, respectively.
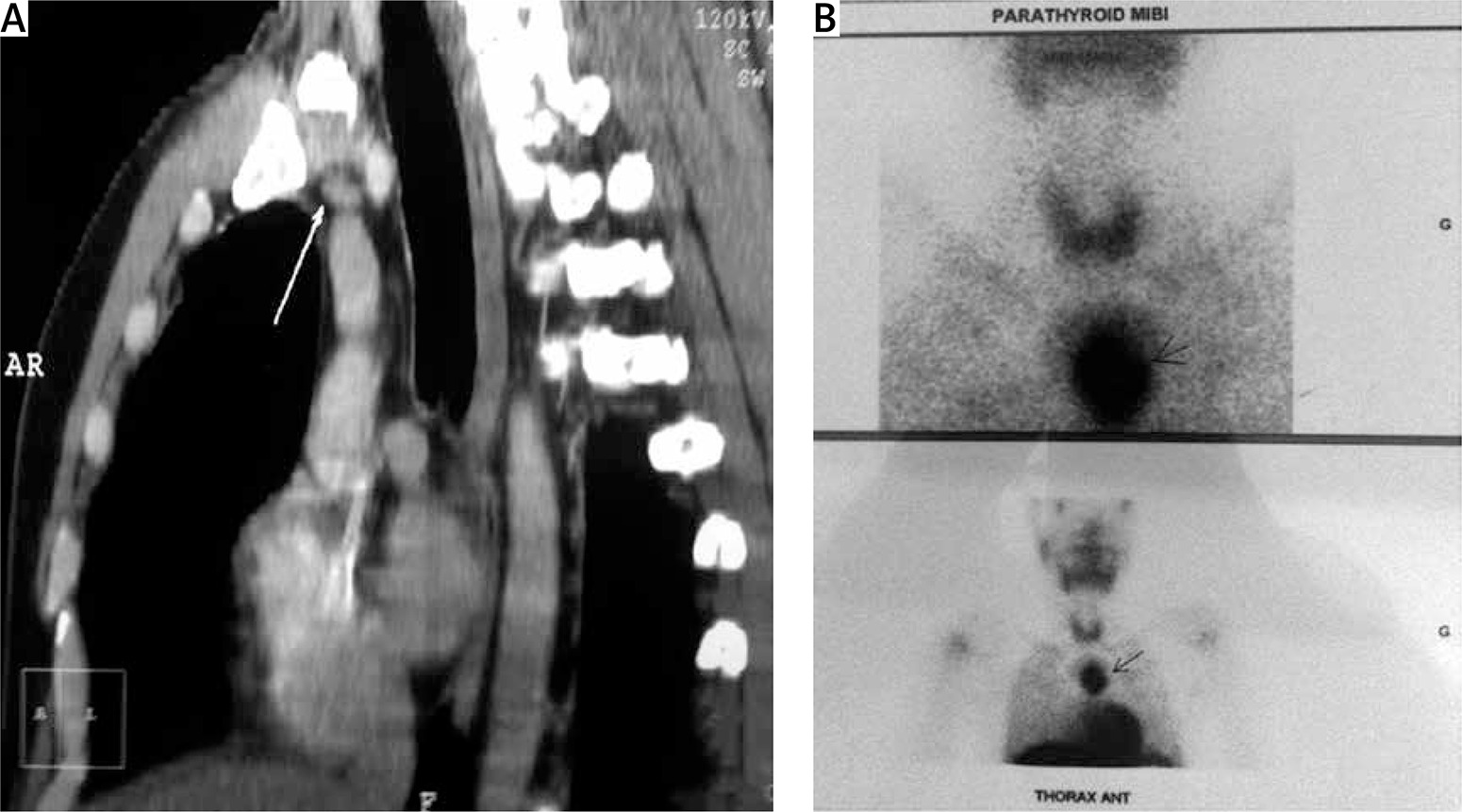
Imaging examinations were first cervical ultrasound in 28.5% (n = 6/21) giving a presumptive diagnosis of MPA, but in addition it allowed the diagnosis of 2 cases of multiheteronodular goiter; MIBI (99mTc-labeled methoxyisobutyl isonitrile) scintigraphy was used in 47.6% (n = 10/21) and cervico-thoracic CT scan was used in 100% (n = 21), both offering a positive diagnosis of MPA in 100% (Figure 1).
Figure 1
A – Sagittal view of thoracic CT scan shows an upper mediastinal mass neighboring a vascular structure. B – A 99mTc-MIBI scintigraphy reveals ectopic parathyroid adenoma in the superior mediastinum
Six of our patients presented with postoperative hypocalcemia treated with intravenous calcium and then per os intake.
Surgical technique
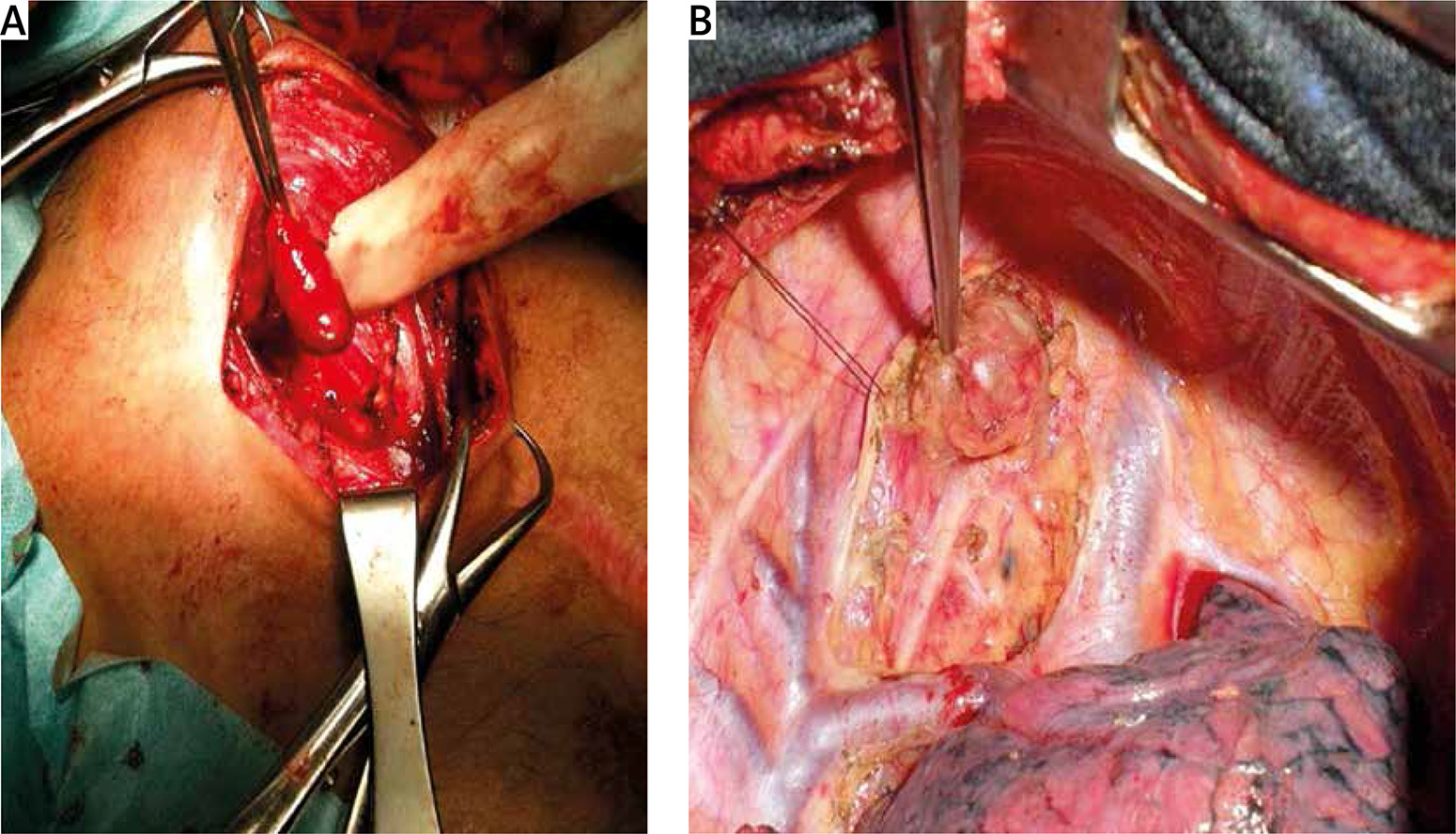
Adenoma resection was performed in all cases, associated in two cases with subtotal thyroidectomy. The surgical approach was (Figure 2) a cervicotomy in 19% of cases (n = 4/21), a cervico-manubriotomy in 47.6% (n = 10/21), subtotal cervico-sternotomy in 9.5% (n = 2/21), manubriotomy in 9.5% (n = 2/21), sternotomy in 9.5% (n = 2/21), thoracotomy in 4.7% (n = 1/21).
Figure 2
A – Peroperative view of pathological parathyroid adenoma resected via cervicotomy. B – Preoperative view of thoracotomy showing a superior inter-tracheoesophageal parathyroid adenoma
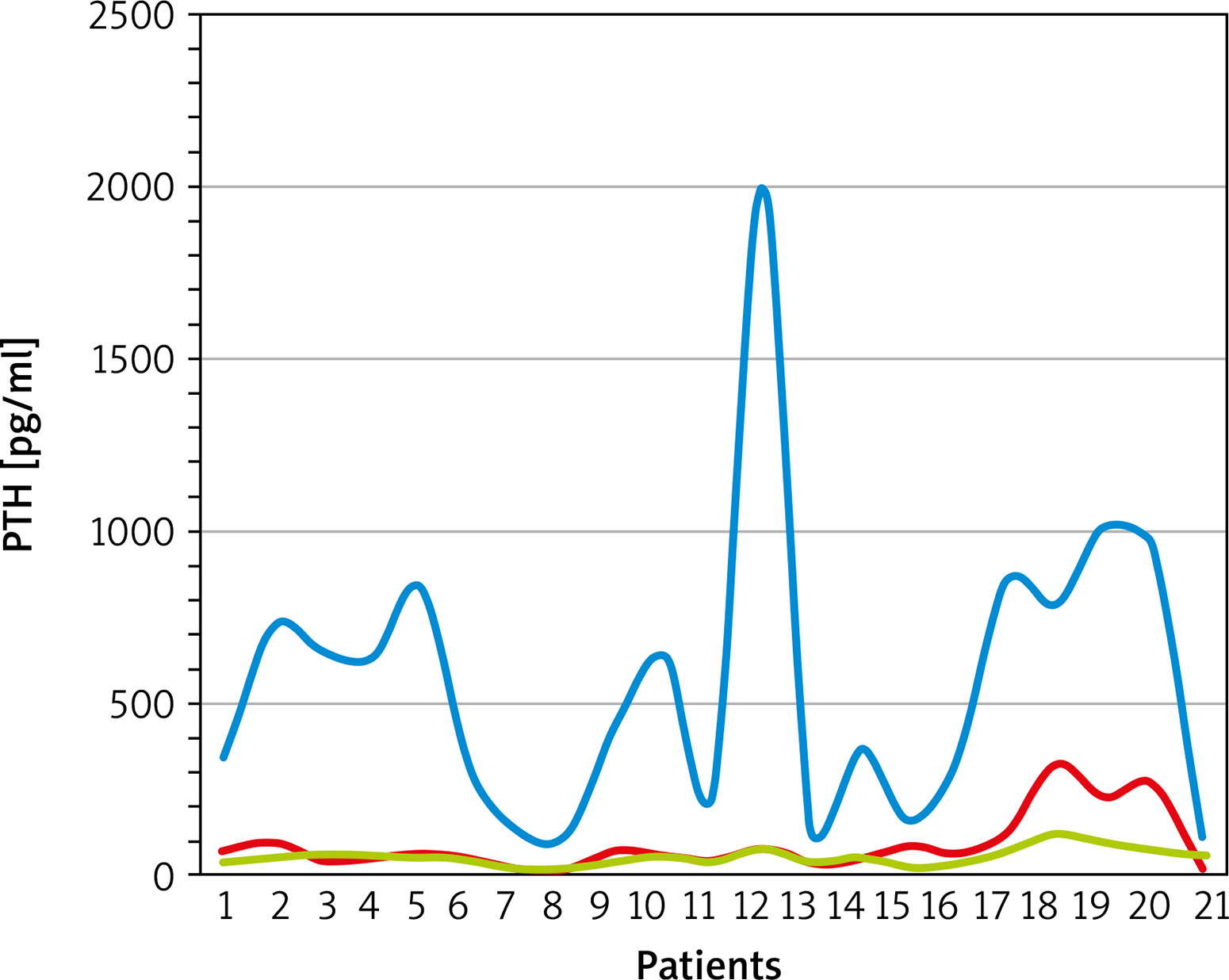
Whatever the surgical approach, per-operative PTH dosage was done 15 minutes after removal of the pathological gland in the homolateral internal jugular vein. Post-operatively PTH dosage was at H4 and H24. In one patient the PTH level was still high after resection of MPA to become lower after one hour of the post-operative course. We noted a significant drop in value compared to the initial value (Figure 3), with an average value of 47 ng/l for post-operative dosage at H24. Six of our patients presented severe hypocalcemia post-operatively that was treated with intravenous calcium then per os intake. About 72% of patients (n = 15) were discharged on the third day, but 6 of them left the hospital 7 days after surgery because of persistent hypocalcemia and hungry bone syndrome, a severe but rare form of postoperative hypocalcemia. The one-month, 3-month, 1-year and 2-year follow-up was uneventful.
Discussion
Mediastinal parathyroid adenomas are rare without gender predominance, as evidenced by our study in agreement with other studies [4]. The classic presentation of parathyroid adenoma is that of hyperparathyroidism associated with psychiatric symptoms, kidney, bone and gastrointestinal stones [4]. However, this complete constellation of symptoms is rarely observed today due to frequent assessments of patients’ blood chemistry.
On physical examination, the majority of cervical parathyroid adenomas did not have a palpable mass in the neck. The small size of these adenomas is one of the reasons why a clinician may suspect another disease before looking at the laboratory results. It is the hypercalcemia with concomitant high levels of PTH that confirms the diagnosis of primary hyperparathyroidism. But other biological data should be collected, such as phosphorus levels, vitamin D and others.
Accurate preoperative identification of hyperfunctional parathyroid glands is imperative for satisfactory results, but not all imaging modalities should be used to diagnose this condition. In our study, preoperative diagnosis was obtained by MIBI-Tc99m scintigraphy, cervico-thoracic CT and cervical ultrasound. The latter is limited by the operator’s experience and inability to explore the mediastinum. Moreover, in patients who have never undergone cervicotomy, its sensitivity to detect parathyroid adenoma reaches 80%, but after a first cervical surgery (as was the case in two of our patients) or associated thyroid disease (goiter) sensitivity is reduced to only 30% [5].
MIBI scintigraphy is based on the difference in clearance of the Tc99m-MIBI tracer in the thyroid and parathyroid glands. After injection, the tracer is captured early and intensely on both glands, the elimination of the thyroid is faster while the fixation of the parathyroid persists over time. Therefore, MIBI scintigraphy is considered positive because of the existence of a focus of hyperfixation at an early stage, the intensity of which persists or even increases with time. We also noted that some authors have shown that the sensitivity of MIBI scintigraphy improves when the weight of the gland is greater than 600 mg [6], allowing cervical and mediastinal exploration in search of parathyroid pathology.
Despite the fact that MRI provides good contrast for soft tissue study, cervicothoracic CT with contrast has been used to accurately localize ectopic parathyroid adenoma, with an estimated sensitivity of 75% [7]. Recently, fluorocholine (FCH) PET/CT offers a good tool in parathyroid gland exploration. Behera and Damle explained the increasing role of FCH PET/CT over MIBI scintigraphy because of the better spatial resolution and the detection of smaller adenomas [8]. Regarding location, upper parathyroid gland ectopias are less frequent (1%), and can be found in the retropharyngeal spaces, compared with lower parathyroid gland ectopias that can be found throughout the large descending area with the thymus, from the hyoid bone at the top to the pericardium at the bottom, from the prevertebral plane at the back to the plane of the infrahyoid muscle and sternum at the front [9].
Mediastinal ectopic parathyroid adenomas are a recognized cause of persistent hyperparathyroidism, and hypercalcemia in approximately 0.8% of iterative parathyroidectomies.
There is no curative medical treatment; the treatment of choice is surgery to resect the pathological glands. This removal surgery can become delicate depending on site and surrounding structures. In addition, there are questions about the benefits of surgery in asymptomatic patients; in response, the Fourth International guidelines for the management of asymptomatic adenomas have published indications for surgery in asymptomatic patients [10]. Once the indication is established, several types of surgical procedures can be used depending on multiple factors. In our setting, conventional surgery for the management of MPA is still widely used, but recently new approaches are being developed to minimize interventions and reduce complications and repeated surgery. Elsewhere it includes minimally invasive parathyroidectomy, which includes directed parathyroidectomy, endoscopic parathyroidectomy (endoscopic, video-assisted and robotic total parathyroidectomy) and isotope-guided parathyroidectomy. Most of these surgical approaches are recommended for solitary lesions. However, while preoperative imaging may be negative in approximately 30% of cases [7], the risk in some settings of encountering multi-glandular lesions may necessitate exploration by conventional surgery. A large proportion of mediastinal parathyroid adenomas can be successfully removed through a cervical approach. However, if this approach is not possible, a total or partial sternotomy is required and is associated with increased postoperative pain, prolonged hospital stay and complications in up to 21% of patients.
When a tracer is not used for surgery (radio-guided parathyroidectomy), intraoperative location of the parathyroid gland requires the surgeon’s experience to discriminate a normal parathyroid gland and a pathological, hypervascularized, darker parathyroid gland [10–15], both orthotopic or ectopic. Once the pathological parathyroid gland has been identified, it is extracted with great care; it is necessary to completely remove an intact gland by slowly grasping its capsule until the vascular pedicle is identified and then ligated [16, 17].
Once excision has been performed, regardless of the approach, the intraoperative PTH dosage and its kinetics are essential to ensure complete excision of the pathological parathyroid gland. Postoperatively, large MPAs may be associated with a higher incidence of postoperative hypocalcemia [18–21] due to hungry bone syndrome (six in our study). Patients with small MPAs were less likely to develop postoperative hypocalcemia.
Conclusions
Parathyroid adenoma can occur in a mediastinal ectopic situation. It therefore represents a particular challenge at both the diagnostic and therapeutic levels. The management is based on imaging assessment, which is an essential step, since it determines the precise location and number of hyper-functioning parathyroid glands, providing exact cervico-mediastinal mapping, which will allow the surgeon to perform a targeted “surgical strike”, by adapted ways.









