
Minimally invasive direct coronary artery bypass (MIDCAB) is a method of surgical revascularization in which the left internal mammary artery (LIMA) is harvested to graft the left anterior descending artery (LAD) through a small incision on the chest wall (Figure 1 A). The procedure is performed without cardioplegia induced cardiac arrest and allows the burden of open-chest surgery to be avoided. Previous studies have shown excellent early and long-term results for MIDCAB performed either as a single procedure for an isolated LAD lesion [1] or as a step in hybrid revascularization with percutaneous coronary intervention to other significantly stenosed arteries [2]. Nevertheless, the data for the use of MIDCAB as a method of choice for re-do cardiac surgery are sparse.
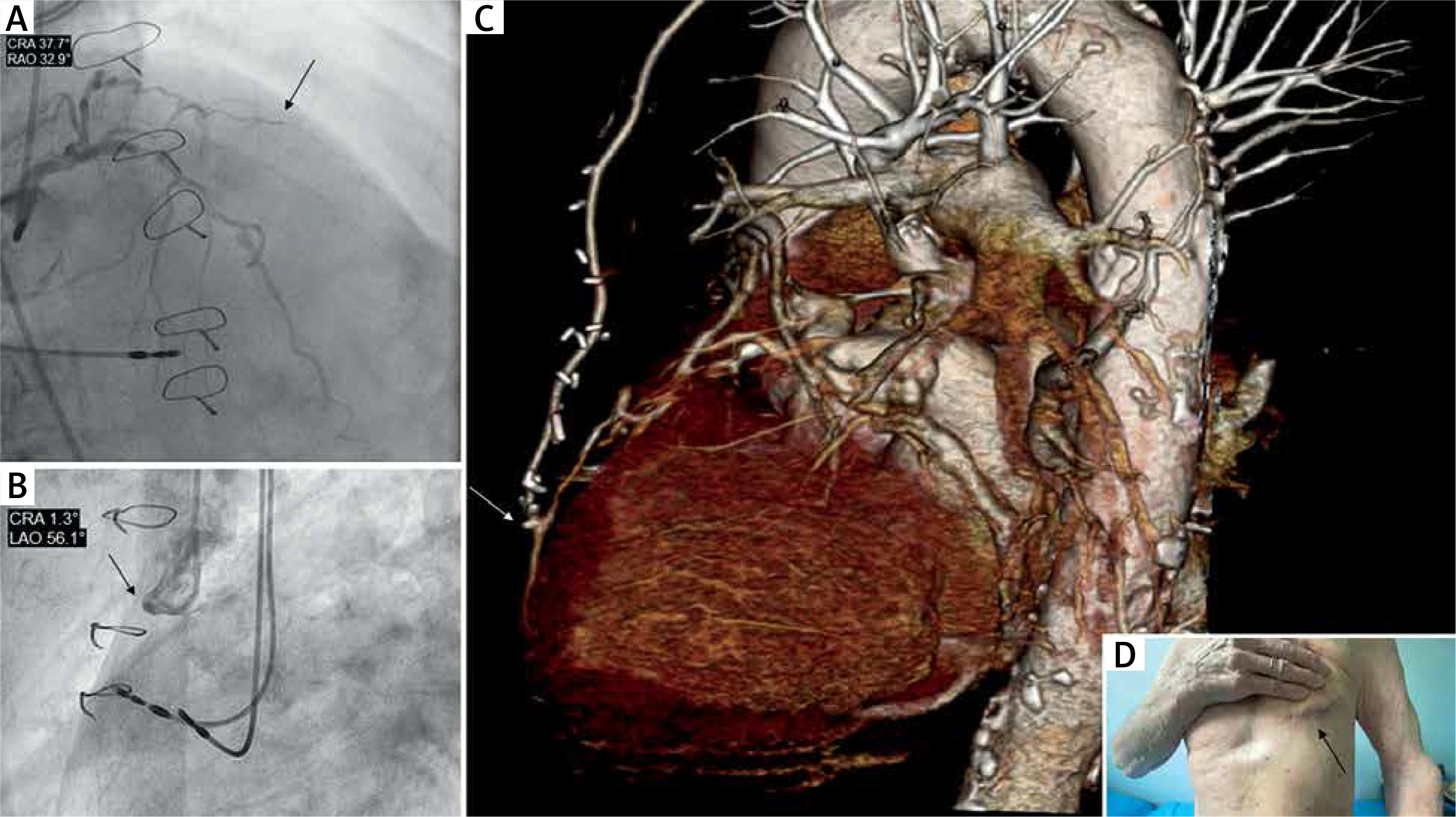
Figure 1
A – On coronary angiography CTO LAD, B – on coronary angiography occluded venous graft to LAD, C – on postoperative computed tomography patent LIMA graft to LAD, D – incision site 11 days after surgery
We report a case of a frail 86-year-old man, with concomitant diabetes on insulin, asthma, heart failure, peripheral artery disease with previous carotid stenting, and impaired renal function, who underwent a successful re-do MIDCAB in April 2021 after previous coronary artery bypass grafting (CABG) for multivessel coronary artery disease in 1996. The initial surgery was performed via median sternotomy and venous grafts were implanted in the LAD, diagonal (Dg) and marginal (Mg) arteries.
The patient was admitted to hospital due to exacerbation of angina (CCS III) and a recent decrease in left ventricle ejection fraction (LVEF 35%). Urgently performed coronary angiography showed chronic total occlusion (CTO) of the LAD with an occluded graft to the LAD, 70% stenosis in the circumflex artery with a patent venous graft to the Mg branch, and CTO in the proximal right coronary artery. In spite of a very high perioperative risk (EuroSCORE II 28.5%, STS risk of mortality 19.3%), due to coronary lesion anatomy, the patient’s poor biological condition, and multiple comorbidities, an urgent re-do MIDCAB was recommended as the safest option by the Heart Team.
Through a left antero-lateral minithoracotomy the LIMA was skeletonized and implanted distally to the previous anastomosis (Figure 1 F). Postoperatively, the patient required reoperation through the same incision to evacuate the hematoma from the left pleural cavity and received empiric antimicrobial therapy for pneumonia. However, the patient remained free from major adverse cardiac and cerebrovascular events throughout the hospitalization, and no renal or wound complications were reported. The patient was discharged for cardiac rehabilitation at postoperative day 11 with improvement in left ventricle function (LVEF 50%). The follow-up appointment was performed 30 days after the surgery. The patient remains asymptomatic and the quality of life improved within the observation period.
To date, only two studies have presented the utility of MIDCAB as a re-do CABG in a total of 20 patients [3, 4]; however, this report is the first to describe the successful implementation of this method in a very high-risk patient.







