
Streptococcus gallolyticus (SG) is a known cause of infective endocarditis (IE), particularly linked to colorectal cancer, prompting a thorough investigation of underlying gastrointestinal malignancies in cases of bacteraemia [1]. IE affecting the aortic valve can extend to the mitral valve, causing a secondary ‘kissing lesion’, which may lead to a rare but serious condition: the formation of a mitral valve aneurysm (MVA) [2]. This can result in severe complications such as perforation, mitral regurgitation, pulmonary oedema, and systemic embolization [3]. This report presents a case of SG endocarditis affecting both the aortic and mitral valves, with an atypical subacute presentation, differing from the usual acute onset of this severe condition.
A 62-year-old man arrived at the emergency department with a 3-week history of rigours, headaches, anorexia, bilateral flank tenderness, and significant weight loss. He had recently travelled to Australia from Kazakhstan, where he resides. His medical history included hypertension, former smoker, consumed alcohol infrequently, and had no history of recreational drug use.
On examination, the patient was afebrile, haemodynamically stable with a blood pressure of 112/51 mm Hg and a heart rate of 70 bpm. Initial investigations revealed normocytic anaemia, elevated white blood cell count, and raised inflammatory markers. Blood cultures identified SG, and subsequent cultures on days 1 and 2 confirmed ongoing bacteraemia, which resolved by day 4.
A computed tomography (CT) scan revealed a rectal mass suspicious for neoplasm, unilateral sacroiliitis, and a right kidney lesion concerning for malignancy (Figure 1). A flexible sigmoidoscopy performed on day 6 of admission demonstrated a 45 mm polyp, with histopathology confirming a tubulovillous adenoma with low-grade dysplasia. A transthoracic echocardiogram (TTE) revealed a large echogenic mass attached to the aortic valve, causing severe eccentric regurgitation and reverse flow in the descending aorta (Figures 2 A, B). Furthermore, a saccular image with an attached vegetation and turbulent flow was noted on the anterior mitral leaflet (AML), indicating perforation (Figures 2 C, D).
Figure 1
A – Contrast-enhanced computed tomography (CT) of the pelvis demonstrating an intraluminal soft tissue density within the rectum, accompanied by surrounding mucosal thickening, fat stranding, and intrapelvic free fluid, raising suspicion for a rectal neoplasm. B – Contrast-enhanced CT of the abdomen showing identified bilateral renal lesions, with the largest located in the right superior pole, measuring 25 mm in diameter
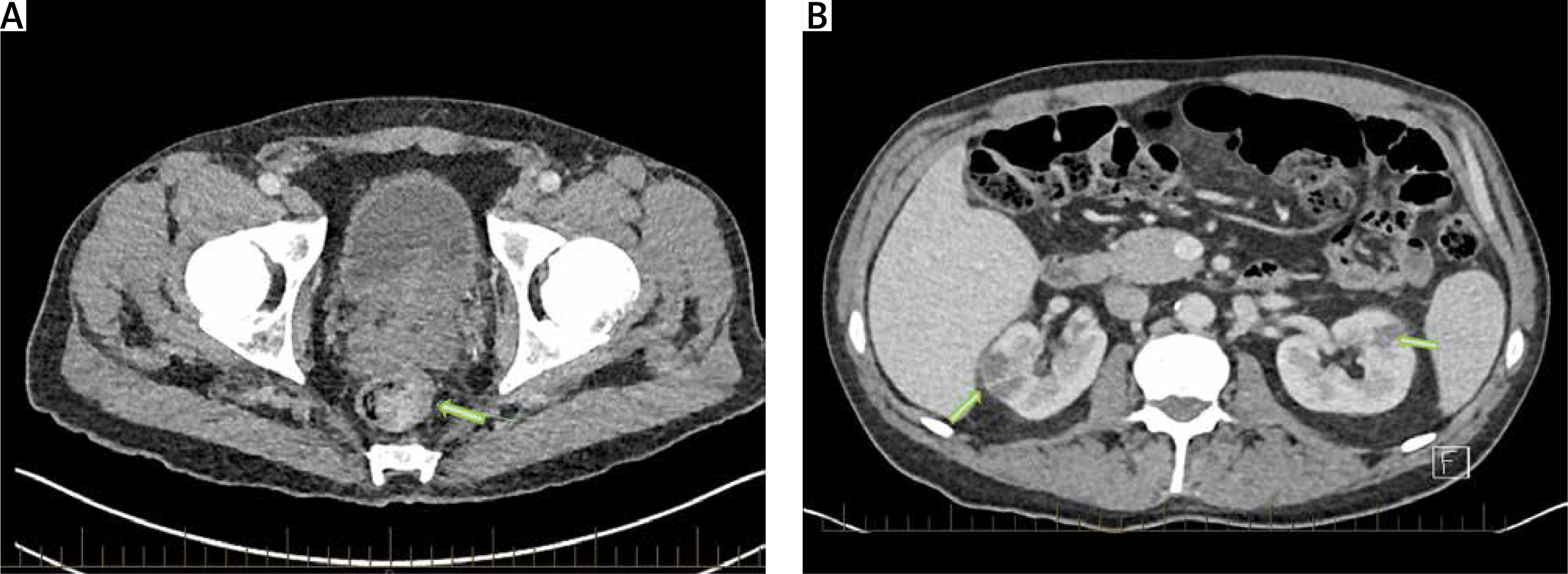
Figure 2
A – 2D TTE PLAX view demonstrating vegetations on the aortic and mitral valves (arrows). B – Pulse-wave Doppler showing holodiastolic flow reversal in the descending aorta (arrow). C – 2D TTE zoomed PLAX view showing a vegetation on the anterior mitral valve with a small saccular appearance, suggestive of an aneurysm. D – 2D TTE with colour Doppler in systole demonstrating flow through the mitral valve. E – TOE long-axis aortic view without (left) and with (right) colour Doppler, showing a vegetation (arrow) and severe regurgitation in the aortic valve. F – TOE long-axis view focused on the mitral valve demonstrating an aneurysm in A2 (green arrow) and the associated vegetation (yellow arrow) in the left panel, and TOE long-axis view with colour Doppler confirming the perforation (red arrow). G – 3D Cardiac TrueVue image (left atrial view) demonstrating a perforation in A2 with a vegetation attached to the aneurysm. H – CT chest on admission showing the aneurysm in the anterior mitral valve (red arrow)


A transoesophageal echocardiogram (TOE) confirmed native valve endocarditis, revealing multiple echogenic masses on the aortic valve, the largest measuring 1 cm. Severe aortic regurgitation was present (Figure 2 E, along with a ‘kissing lesion’ on the AML (Figure 2 F), which exhibited a windsock aneurysm with perforation (Figures 2 G, H). Additionally, a 0.63 cm × 0.5 cm echogenic mass was identified on the AML, closely associated with the aneurysm. A multidisciplinary team recommended aortic and mitral valve replacement following 4 weeks of intravenous benzylpenicillin therapy.
Surgical findings included infectious destruction of the left and right coronary commissures, but no aortic root involvement or abscess. A perforation near the AML annular line with a ‘windsock’ appearance in the A2 segment, measuring approximately 0.5–1 cm, was identified. Although valve replacement was selected in this case due to extensive tissue destruction, mitral valve repair with closure of the leaflet defect using a pericardial patch may be considered in cases where inflammation is limited and the perforation site is suitable for repair. Ultimately, both the aortic and mitral valves were replaced with bioprosthetic prostheses, and the patient completed an additional two weeks of intravenous antibiotic therapy
MVAs are rare, occurring in 0.2–0.29% of IE cases. These saccular protrusions of the mitral valve collapse in diastole and expand in systole, most frequently affecting the AML. Perforation is the most concerning complication, leading to severe mitral regurgitation [4, 5]. TOE is more sensitive than TTE for diagnosing MVA, and 3D-TOE provides superior differentiation from other pathologies, such as abscesses or vegetations [6].
The exact mechanism of infection transmission remains uncertain; it may result from the direct extension of infection from the aortic valve to the mitral valve via vegetations striking the anterior mitral leaflet (‘kissing lesion’), or alternatively, from simultaneous seeding of both valves through bloodstream infection. While Staphylococcus aureus, especially methicillin-resistant strains, is known for rapid tissue destruction and abscess formation, this case suggests that MVA formation may be more common in less aggressive infections such as SG, which can follow a more indolent course [7].
Conservative management of MVA is an option when there is no significant mitral regurgitation, but surgical intervention is necessary in cases of rupture, enlargement, or haemodynamic compromise.
This case underscores the importance of recognizing MVA as a rare but serious complication of IE, particularly when infection extends from the aortic valve. Despite significant valve destruction, the subacute presentation highlights the need for early detection and timely intervention to prevent catastrophic outcomes.









