
Marfan syndrome (MFS) is a rare connective tissue disorder caused by fibrillin-1 (FBN1) mutations [1]. It primarily involves cardiovascular, skeletal, and ocular systems, and increases the risk of aortic dissection, particularly during pregnancy due to hemodynamic and hormonal changes [2]. Dissections are more likely in women with an aortic root diameter over 45 mm, and pregnancy is generally discouraged in these cases [3]. If the root measures between 40 mm and 45 mm, clinical judgment based on family history and growth rate of the aorta is advised [4]. In acute type A dissection, valve repair and valve-sparing procedures can yield durable outcomes [5].
A 27-year-old woman at 34 weeks of gestation with MFS and mild mitral regurgitation was transferred after echocardiography suggested aortic dissection. On admission, she was stable. Transthoracic echocardiography (TTE) confirmed aortic dissection with moderate aortic and mitral regurgitation and preserved left ventricular ejection fraction (LVEF) 65%. Computed tomography angiography (CTA) confirmed a Stanford type A dissection from the non-coronary sinus through the ascending aorta and arch, with 44 mm aortic root diameter (Figures 1 A, B). Due to the fetal risk of cardiopulmonary bypass with deep hypothermia and considering the patient’s stable condition and the risk of hemorrhagic shock with combined procedures, a staged approach was chosen: cesarean section followed by delayed cardiac surgery. As our center lacks an obstetrics department, the cesarean section was urgently performed in our operating room in coordination with a gynecological team. General anesthesia was uneventful. The newborn (APGAR 8, 2300 g) was transferred to neonatology. The mother was admitted to the intensive care unit (ICU), remained stable under urapidil to maintain systolic blood pressure (SBP) < 120 mm Hg, and was extubated the following day. Lactation was suppressed. Thromboprophylaxis and daily gynecologic and cardiologic assessments were performed. Ultrasound was used to assess uterine bleeding, and echocardiography to monitor effusion and valvular function.
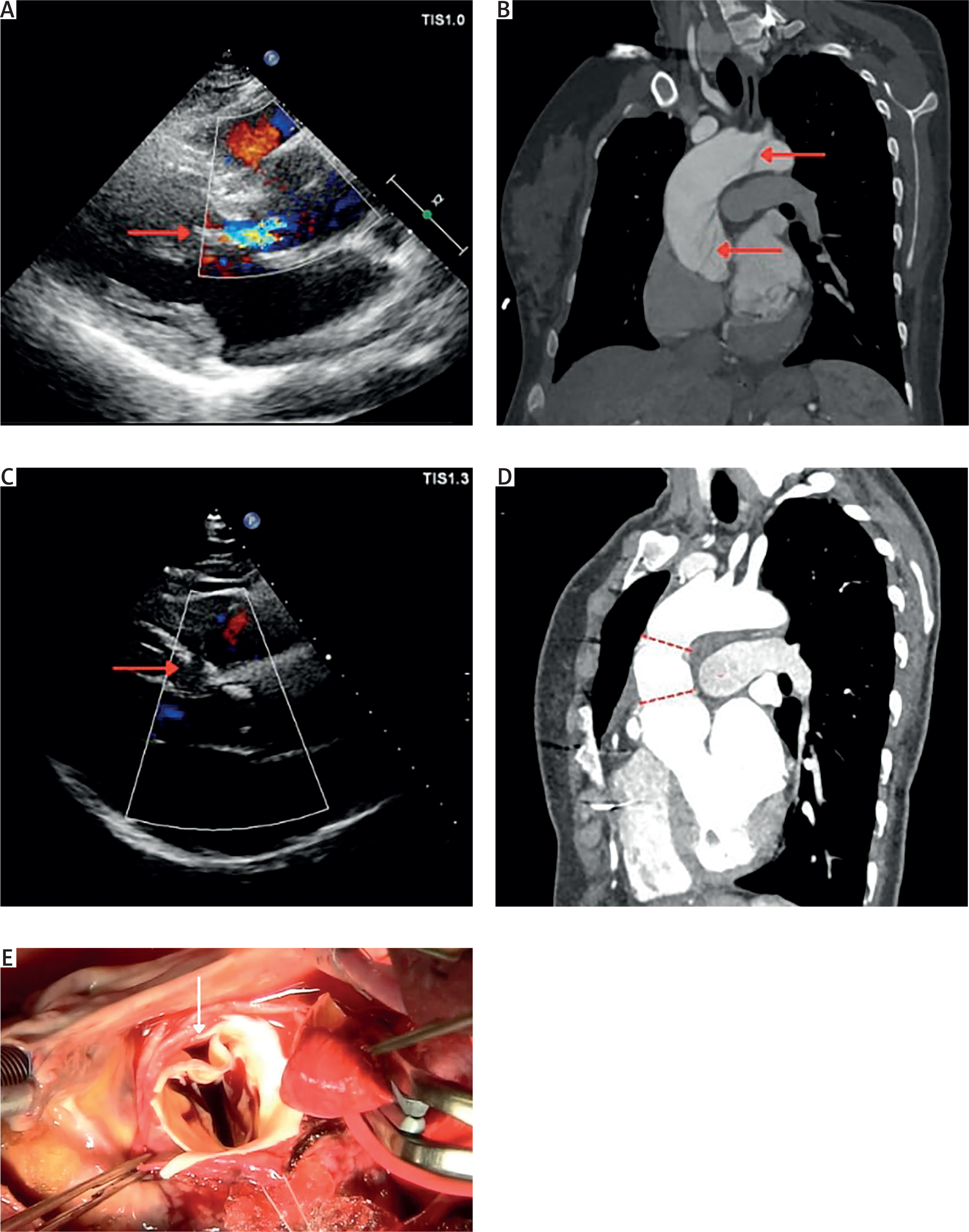
Figure 1
A – Preoperative transthoracic echocardiography. Moderate aortic valve regurgitation is visible (red arrow). B – Preoperative computed tomography angiography. Aortic dissection (red arrows) is visible, originating in the aortic root and extending to the aortic arch. C – Transthoracic echocardiography at 6-month follow-up. No aortic regurgitation is observed (red arrow). D – Postoperative computed tomography angiography at 6-month follow-up. A vascular graft is visible (area between dashed lines). E – Intraoperative photograph of the dissected right–noncoronary commissure of the aortic valve causing moderate aortic regurgitation
On postoperative day 8, the patient underwent uneventful cardiac surgery. Aortic insufficiency resulted from rupture at the non-right and non-left commissures. The aortic arch showed no re-entry on inspection. Aortic root repair with adhesive, commissural reconstruction, and sinotubular junction remodeling was performed, followed by replacement of the ascending aorta with a 30-mm vascular graft (Figure 1 E). A gynecologic team was present to manage potential uterine bleeding. Postoperatively, the patient remained stable on norepinephrine, later transitioned to urapidil. Following transfusion of two blood units, she was mobilized and discharged in good condition.
According to current guidelines, patients with MFS who have undergone aortic repair should receive TTE at discharge, at 6–12 months, and annually thereafter, with CTA or magnetic resonance imaging (MRI) performed annually, or every 2 years if the condition remains stable [5]. At 6 months, echocardiography showed LVEF 55%, competent aortic valve, and persistent moderate mitral regurgitation. CTA confirmed a successful surgical outcome (Figures 1 C, D). The infant is developing normally.
This case highlights the importance of a multidisciplinary approach in managing acute type A dissection in pregnancy. A staged strategy – urgent cesarean followed by delayed surgery – minimized hemorrhagic risk while maintaining maternal and fetal stability, underscoring the value of team-based care.









