
Acute myocardial infarction (MI) occurs due to restricted blood flow through the coronary arteries, resulting in ischaemia and subsequent myocardial necrosis. Currently, MI is classified, based on the presence or absence of ST-segment elevation in the electrocardiogram and dynamic changes in cardiac markers, into ST-segment elevation MI (STEMI) and non-ST-segment elevation MI (NSTEMI) [1]. However, the current classification does not take into account the occlusion status of the coronary artery, which should determine the treatment algorithm. Here, we present a patient with an occlusive, but not ST-elevation, MI.
A 69-year-old woman was admitted to the cardiac intensive care unit (CICU) with dyspnoea and chest pain. Sixteen days earlier she underwent an urgent endovascular aneurysm repair with stentgraft implantation due to dissecting aortic aneurysm. An electrocardiogram revealed diffuse ST-segment depressions in 9 leads and ST-segment elevation in aVR (Figure 1). About 1.5 h after admission to the cardiac intensive care unit (CICU), the patient suffered a sudden cardiac arrest due to ventricular fibrillation. Cardiopulmonary resuscitation (CPR) was initiated, and the patient was transferred to the catheterization laboratory. Coronary angiography showed chronic total occlusion of the right coronary artery and circumflex artery, critical left main (LM) coronary artery stenosis, and acute occlusion of the left anterior descending (LAD) artery. Percutaneous coronary intervention (PCI) of the LM and LAD was performed, resulting in the return of flow through LAD and spontaneous circulation. However, the patient experienced recurrent episodes of cardiac arrest due to pulseless electrical activity, and eventually, given the lack of therapeutic options and unfavourable prognosis, CPR was stopped.
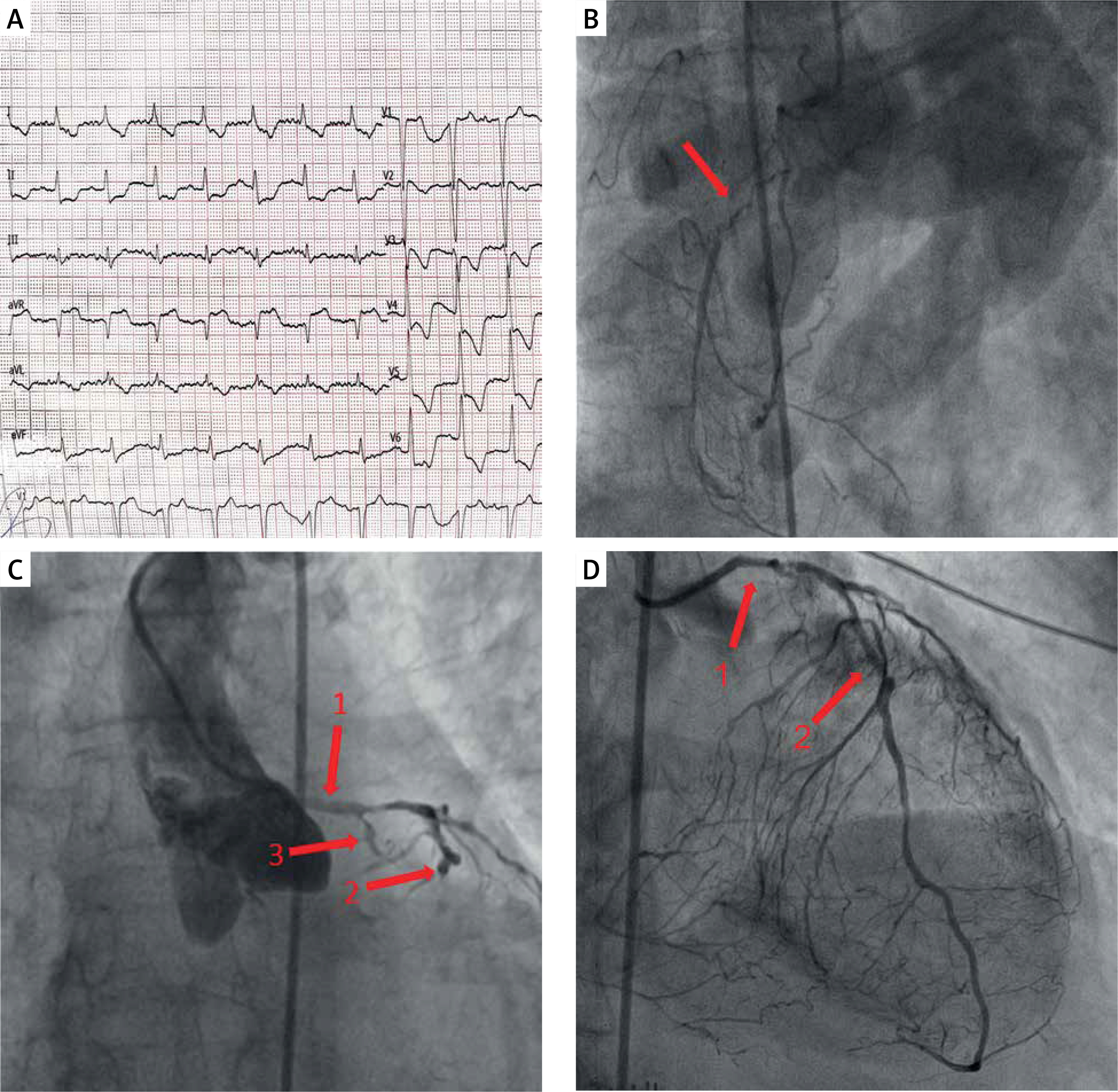
Figure 1
A – Electrocardiogram revealing diffuse ST-segment depressions with ST-segment elevation in aVR lead. B – Coronary angiography showing chronic occlusion of the right coronary artery (arrow) with partial recanalization; right anterior oblique (RAO) anterior-posterior view. C – Coronary angiography showing significant stenosis of the left main coronary artery (1), acute occlusion of the left anterior descending artery (2) and chronic occlusion of the circumflex artery (3); left anterior oblique caudal view. D – Restoration of flow through left anterior descending artery (2) after percutaneous coronary intervention; RAO cranial view
The STEMI vs. NSTEMI paradigm was developed in response to the introduction of reperfusion therapy, which was a breakthrough in the treatment of acute coronary syndromes (ACS). The aim of this paradigm was to identify patients who would benefit from un emergency PCI. However, 25% of patients with NSTEMI have acute coronary artery occlusion and require an emergency PCI despite no ST-segment elevation. Patients with occlusive culprit lesions have 67% higher 6-month mortality rate, compared to patients with non-occlusive lesions, despite the same treatment [1]. Thus, division of ACS into STEMI and NSTEMI has limitations because it does not take into account the occlusion status of the coronary artery. Therefore, a modification of the current ACS classification system based on the occlusion of the coronary artery has been proposed. The occlusive MI (OMI) is defined as STEMI and all STEMI equivalents introduced by American College of Cardiology [2], which warrant an emergency PCI and aggressive postprocedural dual antiplatelet therapy (DAPT) with a potent P2Y12 receptor antagonist. The latter is especially important given the still widespread use of clopidogrel in post-MI patients, which is contradictory to the current recommendations [3]. In the case of our patient, the ECG picture typical for LM stenosis should have been a rationale for emergency coronary angiography and PCI, instead of CICU admission. The recently presented “Occlusive vs. non-occlusive myocardial infarction (OMI versus non-OMI)” paradigm facilitates the dissemination of knowledge among physicians of all specialties about conditions and ECG findings that require an emergent PCI. Subsequently, it helps to optimize therapeutic decisions regarding interventional treatment and postprocedural DAPT [3, 4].







