
Introduction
Biliary complications are the leading causes of morbidity and mortality after liver transplant (LT). Endoscopic retrograde cholangiopancreatography (ERCP) is widely accepted as a preferred treatment when compared to percutaneous or surgical techniques largely because of lower peri-procedural morbidity and mortality. There have been studies demonstrating the outcomes and complications of ERCP in the normal population; however, these have not been studied comprehensively in LT patients. Previous research has shown that ERCP in LT patients has led to similar complications as in the general population [1]. However, data are lacking in terms of identifying temporal trends and specific predictors associated with poor outcomes. While procedure-related factors may be involved in these complications, patient-associated factors (such as age, sex, race, co-morbidities, etc.) also play a pertinent role. Hence, it is vital to understand the role of these components as it will enable us to better understand how they influence the outcomes of ERCP in this patient population. The primary aim of our study is to analyze the national utilization trend and outcomes of ERCP in LT patients. The secondary aim is to determine the predictors associated with poor discharge disposition.
Liver transplantation has emerged as a lifesaving procedure in patients with acute liver failure and end stage liver disease. Since 2012, the number of liver transplants performed annually in the United States has increased each year, reaching a record number of 8906 in 2020 [2]. Notwithstanding the prodigious advances in surgical techniques and immunosuppressive therapy, postoperative morbidity and mortality remain high, with the leading cause being biliary complications, affecting 25% of recipients. The current survival rates at 1 and 5 years are 85-90% and 70-75%, respectively [3]. Endoscopic retrograde cholangiopancreatography plays a major role in the management of these complications as it helps in confirmation of the diagnosis as well as treatment while precluding percutaneous or surgical interventions [4]. Indications for ERCP in LT patients include dilation and stent placement of anastomotic or non-anastomotic strictures, evaluating post-operative biliary leakage, management of papillary stenosis and removal of bile duct stones [4]. Despite the many diagnostic and therapeutic advantages of ERCP, it is not devoid of complications. Some of the complications arising after ERCP include acute pancreatitis, bleeding, perforation, and infection. These complications can adversely impact the outcome of the procedure in terms of lengthening hospital stay, increasing the cost of in-patient care and, last but not least, increasing the risk of morbidity and mortality [5].
Material and methods
Data source
We extracted our study cohort from the Nationwide Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality (AHRQ) [6]. The NIS is one of the largest all-payer publicly available databases on inpatient discharges from U.S. hospitals maintained by the AHRQ. The NIS approximates a 20% stratified sample of discharges from U.S. community hospitals, excluding rehabilitation and long-term acute care hospitals, and contains more than 7 million hospitalizations annually [6]. With the established weights in NIS, these data could be weighted to represent the standardized U.S. population and obtain national estimates with high accuracy [7].
Study population and design
We queried the 2007-2017 NIS database using International Classification of Diseases, 9th revision, Clinical Modification and International Classification of Diseases, 10th revision, Clinical Modification (ICD-9/10-CM) diagnose codes for LT status. These codes have been used by previously published articles from administrative databases such as the NIS. We also identified ERCP by ICD-9/10-CM procedural codes. We extracted demographics, hospital-level characteristics (geographical region, size, and teaching status) and patient-level characteristics as supplied as part of the NIS [8]. We estimated comorbidities using Elixhauser comorbidity software and mortality risk using the validated All Patient Refined Diagnosis Related Groups (APR-DRGs) mortality score, which are also supplied by HCUP tools and software [9, 10]. Specific concurrent medical conditions, procedures of interest and post-ERCP complications were identified by ICD-9/10-CM diagnosis and procedure codes.
Statistical analysis
To establish the trend, we calculated the proportion of hospitalizations among LT patients who underwent ERCP for each year and used the Cochrane-Armitage trend test for analysis. Descriptive statistics were performed to present the baseline details in sociodemographic, comorbidities and hospital level characteristics of LT patients who underwent ERCP. We also estimated post-ERCP outcomes of interest and predictors of discharge to facilities. We utilized SAS 9.3 (SAS Institute, Cary, NC, USA) for all analyses and included designated weight values to produce nationally representative estimates [7]. For regression models, we used survey procedures to account for the inherent survey design of the NIS to produce more robust estimates [11]. We considered a two-tailed p-value < 0.05 as statistically significant.
Results
Trend of endoscopic retrograde cholangio-pancreatography among liver transplant patients
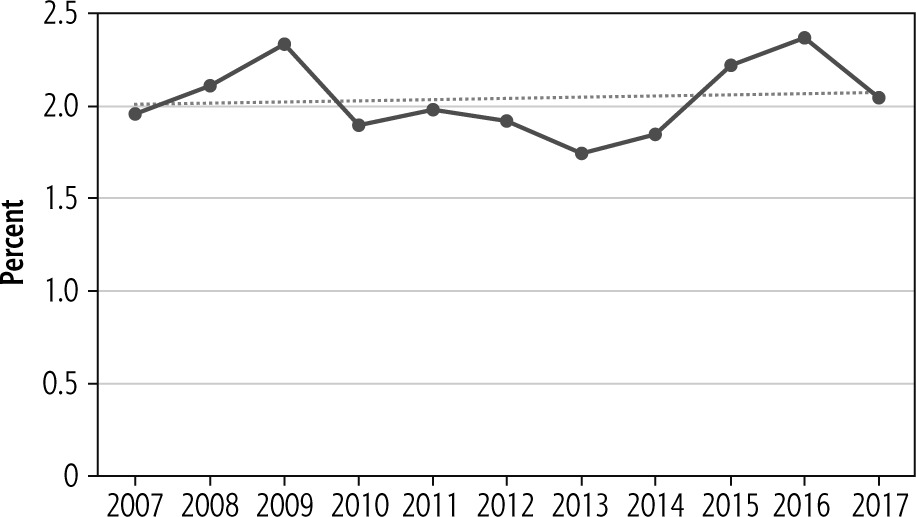
Between 2007 and 2017, 372,814 hospitalizations occurred in LT patients in the U.S., out of which ERCP was performed among 7,632 patients. We observed a steady rise in ERCP utilization from 1.96% (n = 477) in 2007 to 2.05% (n = 845) in 2017 (p < 0.001) (Fig. 1).
Baseline characteristics of liver transplant patients undergoing endoscopic retrograde cholangiopancreatography
The majority of hospitalized LT patients who underwent ERCP from 2007 to 2017 were between the ages of 50 to 64 years (n = 4388, 57.5%) with the mean age of 55.8 ±0.3. More males than females underwent the procedure (n = 5002, 65.5% vs. n = 2630, 34.5%) and White race represented the largest ethnic group (n = 4592, 60.2%). Among these patients, renal failure, hypertension and diabetes mellitus were the most common comorbidities identified. 53.7% (n = 4096) of patients were insured under Medicare and Medicaid while 3.8% (n = 288) of patients were uninsured. The majority of the patients came from the southern region (n = 2431, 32%) and a greater number of the patients were in the middle-income household group (n = 2016, 26.4%). Emergency or urgent admissions accounted for 79.7% (n = 6077) of total hospital admissions while 94.6% (n = 7221) occurred in the teaching hospitals. Other baseline characteristics are outlined in Table 1.
Table 1
Baseline characteristics of liver transplant patients undergoing endoscopic retrograde cholangiopancreatography
† This represents a quartile classification of the estimated median household income of residents in the patient’s zip code. These values are derived from zip code-demographic data obtained from Claritas. The quartiles are identified by values of 1 to 4, indicating the poorest to wealthiest populations. Because these estimates are updated annually, the value ranges vary by year.
Outcomes of endoscopic retrograde cholangiopancreatography among liver transplant patients
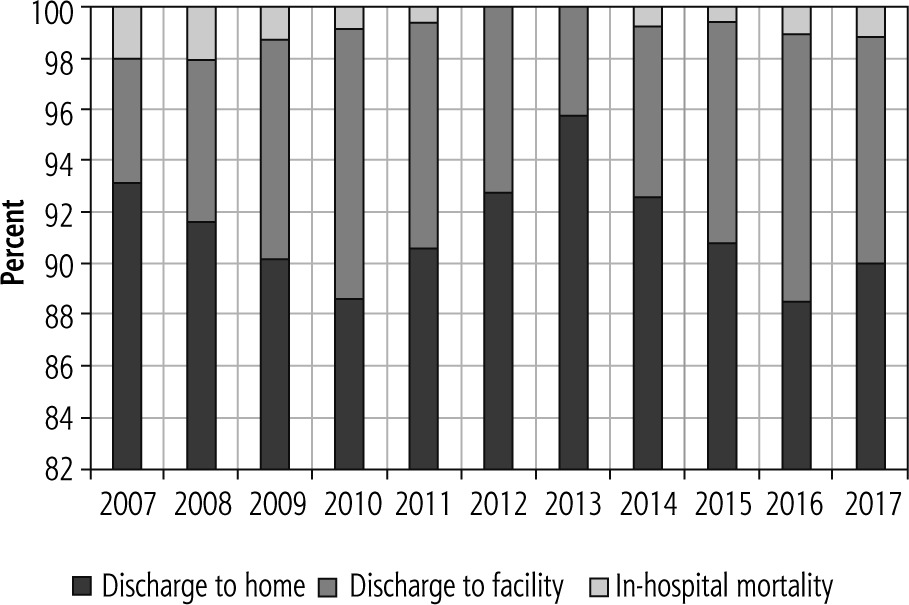
The overall unadjusted in-hospital mortality for patients undergoing ERCP was 1% (n = 73), whereas 8% (n = 607) of the study population was discharged to facilities, with the overall mean length of stay being 7 ±0.3 days. Among the peri-procedural complications, septicemia accounted for 18.3% (n = 1399) followed by post-ERCP pancreatitis 8.8% (n = 674). Other observed complications are outlined in Table 2. In the trend analysis for post-ERCP discharge disposition, no significant changes were seen over the period 2007-2017 (Fig. 2).
Table 2
Outcomes of liver transplant patients undergoing endoscopic retrograde cholangiopancreatography (ERCP)
Predictors of poor discharge disposition among liver transplant patients undergoing endoscopic retrograde cholangiopancreatography
From our analysis, several predictors were associated with increased odds of discharge to facilities in LT patients who underwent ERCP after adjusting for patient demographics, hospital level characteristics and comorbidities. These predictors include concurrent conditions such as septicemia (OR = 3.08, 95% CI: 2.05-4.64, p < 0.001), neurological disease (OR = 2.40, 95% CI: 1.09-5.29, p < 0.0297), renal failure (OR = 1.73, 95% CI: 1.13-2.64, p < 0.0109) and weight loss (OR = 5.25, 95% CI: 3.11-8.86, p < 0.0001).
Discussion
Over the past decade, we have found that ERCP utilization has been increasing among LT patients, which is in accordance with a similar nationwide study by Solanki et al. [12]. A similar trend was observed in a study of decompensated cirrhosis patients [13]. A study of all patient populations from 1988 to 2002 noted a similar dramatic increase in ERCP utilization as well [14]. The national rise in the utilization of ERCP, especially in LT patients, may be attributed to a myriad of factors ranging from increased available expertise to improvement in procedural techniques and peri-procedural care [14]. An extra year of advanced training in ERCP for Gastroenterology fellows may have contributed to the promising ERCP success rate and utilization [15]. In addition, ERCP was found to be more cost effective compared to endoscopic ultrasound (EUS) and magnetic resonance cholangiopancreatography (MRCP) [16]. Easier accessibility, better procedural techniques and cost effectiveness were all plausible reasons for our finding.
Racial disparity has become an important topic in medical research recently. The White population usually has higher medical literacy, easier access to medical care and better socioeconomic status than the Black or Hispanic population. Not surprisingly, we found that Whites were more likely to undergo ERCP compared to Black and Hispanic populations. The disparities in access to LT, post-LT survival and prevalence of chronic liver disease could have contributed to our findings [17-19]. Moreover, Black patients experienced a 21% increased mortality rate (95% CI: 1.12-1.31) after liver transplant compared to White patients [19]. The result was supported by a study from the 2002-2012 United Network for Organ Sharing registry (UNOS) [20]. We can therefore safely infer that Whites are more likely to experience post-LT complications requiring ERCP since they have an overall better survival rate after LT compared to others. Poor medical literacy, low socioeconomic status, and lack of access to medical care are other possible explanations for our finding. However, identifying those factors is beyond the scope of this study. Overall, racial disparities present unique challenges to healthcare professionals involved in the care of patients with chronic liver disease before and after liver transplantation.
Our study did reveal regional variation in ERCP procedures among LT patients. ERCP was more commonly performed in the Southern region compared to the Northeastern region. Although this has not been studied in LT patients, the regional variation in ERCP did exist in pancreatic cancer patients. According to a retrospective study by Tavakkoli et al., pancreatic cancer patients in the Southeast and the West were more likely to receive ERCP compared to those in the Northeast [21]. The racial dynamics in these regions and their peculiar challenges could account for the observed disparity, although other possible reasons need to be considered.
Performing ERCP in LT patients is a complex procedure that requires skills that cannot be met in non-teaching centers. This is suggested by our result which showed that over 94% of ERCP procedures in LT patients were performed at academic teaching centers. The success rate at the university medical center is also higher than that of other facilities, which can reach up to 96.1% [22]. This points to the fact that academic teaching centers have the best outcomes due to the expertise and logistical resources they have at their disposal to handle the complicated ERCP after LT.
The in-hospital mortality rate of ERCP in LT patients was comparable to the general population and considered low. It did not change over the study period. The most common periprocedural complications were septicemia and pancreatitis. Our study is in agreement with two previous studies from Denmark and Spain. Both mentioned that cholangitis and pancreatitis were the two most common complications after ERCP in LT patients [1, 23]. It is notable that our study cannot differentiate between operator, procedure, and patient-related factors while interpreting our results. Although those factors could affect individual center outcomes, the overall impact on the national data should be minimal. Most importantly, adequate selection of patients, novel techniques, and skilled operators in addition to prompt identification and management of comorbidities are the key factors to prevent periprocedural complications.
Discharge to facilities can impose a significant burden on our healthcare system and cause poor quality of life. Several factors influenced the hospital discharge disposition of LT patients who had ERCP. One of the predictors was septicemia. High risk of bacteremia associated with biliary instrumentation and the immunosuppressed condition of LT patients could be contributing factors. The biliary drainage procedure alone is considered as an independent risk factor for post-ERCP bacteremia [24]. Our studied group represented hospitalized patients; therefore the overall infection rate may be higher than previously stated. Although the current guidelines recommend routine prophylactic antibiotics, the infection rate may not change according to a study of elective ERCP in post-LT patients [25].
Another predictor of poor discharge disposition was renal failure. It is well known that end stage renal disease (ESRD) is associated with a higher rate of post-ERCP pancreatitis, ERCP-related bleeding and hospital mortality compared to those without it [26]. A similar association in the studied subjects was reported by Balderramo et al. [1]. Post-ERCP pancreatitis could be related to increased papillary edema from fluid overload resulting in difficult biliary cannulation. On the other hand, platelet dysfunction in the setting of a uremic environment could cause a clotting defect and increase ERCP-related bleeding. Poor hospital outcomes translate to longer stay and hence a higher rate of discharge to facilities. By minimizing aforementioned predictors, one could improve hospital outcomes of the studied patient groups.
Our study has several limitations. Like other nationwide studies, we used ICD codes to capture our population of interest. Diagnostic codes cannot differentiate between pre- and post-procedural complications, which should be borne in mind when interpreting our results. However, similar methods have been used in previously validated studies, and hence the impact should be minimal. Our primary aim was to describe the national trend of ERCP utilization and outcomes in LT patients. Therefore, no comparison was made with the general population. Owing to the retrospective nature, residual cofounders which were not mentioned above could have affected our results as well. Although our study cohort is large enough to represent the whole U.S. population and ideal for epidemiological studies, the indication for ERCP procedures and possible explanation for our findings could not be identified. Specific interventions can be designed in the future based on our findings in order to improve ERCP outcomes in LT patients.
In conclusion, we noted that the utilization of ERCP has been steadily increasing over the past decade among LT patients. Septicemia followed by post-ERCP pancreatitis were the most common periprocedural complications. Patients with septicemia, renal failure, neurological disease, and weight loss were associated with poor discharge dispositions. Future research is needed to explore ways to improve outcomes in these high-risk patient subgroups.





