
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most common type of chronic liver disease in the world, and its incidence is currently increasing. The prevalence of NAFLD is 23.7% and 27.4% in Europe and Asia, respectively [1]. The prevalence is predicted to increase to 15-56% [2]. NAFLD includes non-alcoholic fatty liver and non-alcoholic steatohepatitis (NASH). The pathogenesis of NAFLD involves steatosis, inflammation and fibrosis, and the degree of fibrosis determines the patients’ long-term prognosis. A recent systematic review reported that progression of fibrosis in patients with NAFLD increases all-cause mortality and liver-related mortality [3]. Monitoring the fibrosis staging and development is important to predict the long-term prognosis of patients with NAFLD, and therefore the suppression of hepatic fibrosis should be the primary consideration in the treatment of patients with NAFLD.
Pemafibrate, a novel selective peroxisome proliferator-activated receptor α (PPAR-α) modulator, was made available in Japan in 2018. Pemafibrate has the potential to prevent cirrhosis and liver failure by inhibiting persistent hepatic inflammation and fibrosis due to NAFLD/NASH. We previously reported an improvement of hepatic markers of inflammation and fibrosis in both short-term and long-term studies [4, 5]. In routine clinical practice, we sometimes encounter patients with NAFLD who are refractory to pemafibrate therapy. There are no reports regarding predictors of improvement with pemafibrate therapy in patients with NAFLD, although in some studies correlation analyses were performed [4-7]. Identification of predictors for susceptibility to pemafibrate therapy is important to determine optimal treatment strategies such as dose escalation and/or the use of additional medications. The aim of this study is to identify predictors for improvement of hepatic inflammation and fibrosis after pemafibrate therapy in patients with NAFLD.
Material and methods
Study population
This dual-center retrospective study included patients with NAFLD with dyslipidemia who started treatment with pemafibrate between June 2019 and November 2021 at the Saiseikai Utsunomiya Hospital and the Shinozaki Medical Clinic. Inclusion criteria were: 1) fatty liver diagnosed by abdominal ultrasound, 2) dyslipidemia treated with pemafibrate, 3) sustained alanine aminotransferase (ALT) elevation > 30 U/l for more than three months before starting pemafibrate therapy, 4) negative hepatitis B surface antigen or anti-hepatitis C antibody, 5) normal serum immunoglobulin-G level, 6) alcohol consumption < 30 g/day in males and < 20 g/day in females [4, 5]. Exclusion criteria were: 1) severe chronic kidney disease (estimated glomerular filtration rate < 30 ml/min/1.73 m2), 2) history of previous pemafibrate use, 3) cessation of pemafibrate therapy within six months or 4) patients with diabetes mellitus. This retrospective observational study was approved by the Institutional Review Board of both centers.
Predictors of response of hepatic inflammation and fibrosis
Improvement of hepatic inflammation was evaluated by reduction of ALT level, which is a representative validated marker associated with progression of NAFLD toward hepatic fibrosis [8, 9]. The definition of response of inflammation was 50% or more decrease of ALT levels at six months compared to baseline. Improvement of hepatic fibrosis was assessed by reduction of Mac-2 binding protein glycosylation isomer (M2BPGi) reflecting the grade of hepatic fibrosis [10]. The definition of response of fibrosis was 20% or more reduction in M2BPGi levels at six months compared to the baseline.
Statistical analysis
Changes in parameters after six months of pemafibrate therapy were assessed with the Wilcoxon rank sum test. Cut-off values were determined by receiver operating characteristic curve except for the cut-off value of body mass index (BMI), which was determined by the definition of lean NAFLD (BMI < 25) [11]. To evaluate predictors of response, univariate and multivariate logistic regression analysis were used. To perform multivariate analysis, factors were selected based on clinical significance. Data for lean and non-lean NAFLD were compared using the Mann-Whitney U test. Differences were considered significant when p < 0.05. StatFlex 7.0 software (Artech Co., Ltd., Osaka, Japan) was used.
Results
Baseline characteristics and changes in parameters
One hundred two patients fulfilled the inclusion criteria, and 31 patients were excluded for the following reasons: lost to follow-up (n = 23) and diabetes (n = 8). Consequently, the remaining 71 patients were analyzed (Table 1). All patients were treated with pemafibrate 0.1 mg twice daily without dose escalations. Approximately half of the patients had been treated with a statin before starting pemafibrate, and pemafibrate was given in addition. There was no combination treatment with vitamin E or ursodeoxycholic acid. No adverse events were observed. During six months of pemafibrate therapy, significant improvements were observed in aspartate aminotransferase (AST), ALT, γ-glutamyl transpeptidase (γ-GTP), platelet count, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, total bilirubin, serum albumin, albumin-bilirubin score and M2BPGi (Table 2).
Table 1
Patient baseline characteristics
Table 2
Changes in clinical parameters after six months of pemafibrate therapy
[i] SD – standard error, AST – aspartate aminotransferase, ALT – alanine aminotransferase, γ-GTP – γ-glutamyl transpeptidase, GFR – glomerular filtration rate, LDL – low-density lipoprotein, HDL – high-density lipoprotein, ALBI – albumin-bilirubin, M2BPGi – Mac-2 binding protein glucosylation isomer
Predictors of improvement of hepatic inflammation
Changes in serum ALT levels, a serum marker for hepatic inflammation, were evaluated (Table 3). A greater than 50% decrease in serum ALT levels was found in 35% (25/71) of patients. In univariate analysis, lean NAFLD (BMI < 25) was identified as a significant positive predictor of response to treatment. Subsequent multivariate analysis confirmed this result.
Table 3
Predictors for reduction of serum alanine aminotransferase (ALT) level after pemafibrate therapy
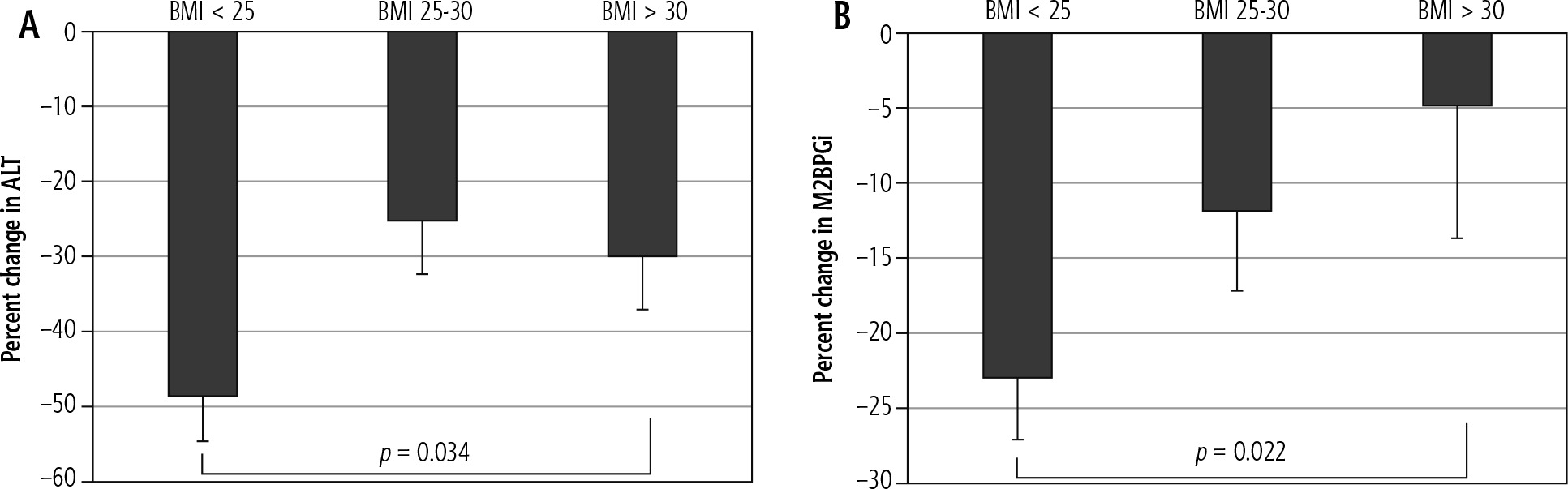
Next, patients were categorized into three groups based on BMI (lean < 25, overweight 25-30 and obese > 30) (Fig. 1A). Compared with baseline levels, all groups showed a significant reduction in serum ALT levels after six months of pemafibrate therapy (lean p < 0.001, overweight p < 0.001 and obese p = 0.001). The reduction of serum ALT in the lean NAFLD group was significantly greater than in the obese NAFLD group (p = 0.034), consistent with a greater improvement in hepatic inflammation.
Fig. 1
Reductions in serum markers after six months of pemafibrate therapy according to body mass index (BMI): A) alanine aminotransferase (ALT), B) Mac-2 binding protein glycosylation isomer (M2BPGi). Bar: standard error. All differences among groups were evaluated, but only statistically significant results are shown
Predictors of improvement of hepatic fibrosis
Changes in serum M2BPGi levels, a marker of hepatic fibrosis, were assessed after treatment (Table 4). A greater than 20% reduction in serum M2BPGi levels was found in 51% (36/71) of patients. In univariate analysis, lean NAFLD (BMI < 25) and age > 50 years were identified as significant positive predictors of response to treatment. Subsequent multivariate analysis confirmed this result.
Table 4
Predictors for reduction of serum Mac-2 binding protein glucosylation isomer (M2BPGi) level after pemafibrate therapy
We compared three groups based on BMI (lean BMI < 25, overweight BMI 25-30 and obese BMI > 30) (Fig. 1B). Pemafibrate therapy for six months significantly reduced serum M2BPGi levels in all groups compared to baseline (lean p < 0.001, overweight p = 0.001 and obese p = 0.046). The reduction of serum M2BPGi in the lean NAFLD group was significantly greater than in the obese NAFLD group (p = 0.022), consistent with a greater improvement in hepatic fibrosis.
Discussion
This retrospective observational study shows that pemafibrate therapy for six months improved both markers of hepatic inflammation and fibrosis regardless of BMI. Notably, treatment was more effective in patients with lean NAFLD (BMI < 25) compared with obese NAFLD (BMI > 30). The baseline ALT or M2BPGilevels were not significant predictors of response, and concurrent use of statins did not influence these responses. Age > 50 years was also a positive predictor of improvement of hepatic fibrosis. This is the first report to identify predictors of response to pemafibrate therapy in patients with NAFLD.
Lean NAFLD is more prevalent in Asia (19%) than in the United States (7%) [11]. The prevalence of NAFLD in Japan is 25.5%, and lean NAFLD comprises 20.7% of these patients [12]. Patients with lean NAFLD have a long-term prognosis similar to those with obese NAFLD despite an increased risk of severe liver disease [13]. The presence of lean NAFLD is significantly associated with a higher risk of incident cardiovascular disease compared to lean individuals without NAFLD [14]. Therefore, long-term control of hepatic inflammation and fibrosis in patients with lean NAFLD is important, as it is in those with obese NAFLD. The results of the present study show that patients with lean NAFLD have a greater response to pemafibrate therapy compared to those with obese NAFLD. Pemafibrate concentration and/or body distribution may be better in lean patients than in obese patients. Older patients are also more responsive to pemafibrate therapy. Adherence to pemafibrate may be better in older patients than in younger ones. Genetic predispositions such as variants in patatin-like phospholipase domain containing 3 (PNPLA3), sarcopenia and/or visceral adiposity may affect the response to pemafibrate therapy [12]. Visceral adiposity and insulin resistance have a central role in the development and progression of lean NAFLD compared with obese NAFLD. Pioglitazone, a PPAR-γ agonist, mainly decreases visceral adiposity rather than peripheral adiposity and improves insulin resistance [15]. Actually, a pan-PPAR agonist showed favorable results with histologic improvement in NASH, but an increase in weight was also observed [16]. For lean NAFLD, additional use of pioglitazone may enhance the improvement observed with pemafibrate.
Recent animal studies from Japan reported the effect of pemafibrate on intrahepatic triglyceride levels and lipid droplet formation [17, 18]. Pemafibrate administration alone prevents NASH development without reducing hepatic triglyceride content [18]. Pemafibrate monotherapy reduces the ballooning score and increases lipid droplet numbers [17]. In short, pemafibrate diminishes the size of lipid droplets but does not decrease the total amount of triglycerides in the liver. These results are compatible with a recent phase II trial evaluating the effect of pemafibrate on NAFLD steatosis and fibrosis [19]. The trial did not show a significant difference in steatosis evaluated by magnetic resonance imaging-estimated proton density fat fraction (MRI-PDFF) but there was a significant difference compared to placebo in fibrosis as evaluated by magnetic resonance elastography (MRE). Taken together, these results suggest that pemafibrate significantly increases small lipid droplet numbers by diminishing large droplets. Decreased lipid droplet size and hepatocyte ballooning due to pemafibrate may reduce compression of hepatic sinusoids, leading to improvement of hypoxia and activation of hepatic stellate cells [20]. The persistent improvement of hepatic ballooning and inflammation might result in amelioration of hepatic fibrosis evaluated by MRE without changing the total liver fat content as evaluated by MRI-PDFF in the phase II trial [19]. Therefore, the optimal primary endpoint of a future trial may be the percentage change in MRE-based liver stiffness or liver-biopsy-based fibrosis scoring.
In the present study, obese patients (BMI > 30) were comparatively refractory to pemafibrate therapy. Additional strategies should be considered for these patients. First, double-dose pemafibrate (0.2 mg twice daily) is a viable option for obese patients to elevate the blood concentration. Second, concurrent sodiumglucose cotransporter-2 (SGLT2) inhibitors may be recommended [21]. In the NASH mouse model, combination therapy with pemafibrate and an SGLT2 inhibitor improves both hepatic steatosis and fibrosis, resulting in prolonged survival and suppression of hepatocellular carcinoma development [17]. Therefore, the synergistic effects of pemafibrate and an SGLT2 inhibitor may be useful for obese patients with NAFLD even if the patient does not have diabetes mellitus. A new randomized controlled trial (ClinicalTrials.gov Identifier: NCT05327127) is being undertaken by Kowa Research Institute to evaluate the effects of pemafibrate and/or an SGLT2 inhibitor on NASH.
Decreased levels of AST, ALT, γ-GTP, LDL cholesterol, triglyceride and total bilirubin were observed in this study, and these changes are consistent with the results of a phase II trial investigating the effect of pemafibrate on NAFLD [19]. An elevated platelet count and decreased M2BPGi levels are also consistent with the results of the phase II trial [19]. Therefore, the results of the present study are considered to be reproducible.
The present study has acknowledged limitations. First, this is a retrospective observational study. Second, the combined use of statin, ezetimibe, and an angiotensin II receptor blocker may influence the improvement of NAFLD, but these medications had been started more than six months before starting treatment with pemafibrate [21]. Third, no histological evaluations were performed before or after the treatment. The major advantage of this study is that patients with diabetes mellitus and those who take anti-diabetic medications were excluded. The development and clinical course of NAFLD are largely influenced by concurrent diabetes mellitus, and anti-diabetes medications such as an SGLT2 inhibitor, glucagon-like pepitide-1 and pioglitazone could improve NAFLD [21].
Conclusions
Pemafibrate therapy improves markers of hepatic inflammation and fibrosis regardless of BMI. Patients with lean NAFLD (BMI < 25) have a greater response to pemafibrate therapy than patients with obese NAFLD (BMI > 30). For patients with obese NAFLD, doubledose pemafibrate and/or combined treatment with an SGLT2 inhibitor should be considered. A randomized controlled trial focusing on improvement of hepatic fibrosis is necessary to clarify the effect of pemafibrate on NAFLD/NASH.





