
A 30-year-old female patient without chronic disease presented with dyspnea and chest pain of 1-year duration. Physical examination, laboratory tests, and electrocardiography were normal. Transthoracic echocardiography revealed a 25 × 23 mm spherical hypoechogenic aneurysmal structure located intramyocardially in the interventricular septum (IVS) with a small septal structure (Figure 1 A, yellow arrow). Color Doppler demonstrated flow towards this structure via two tracts (7 mm and 12 mm) from the lateral wall.
Figure 1
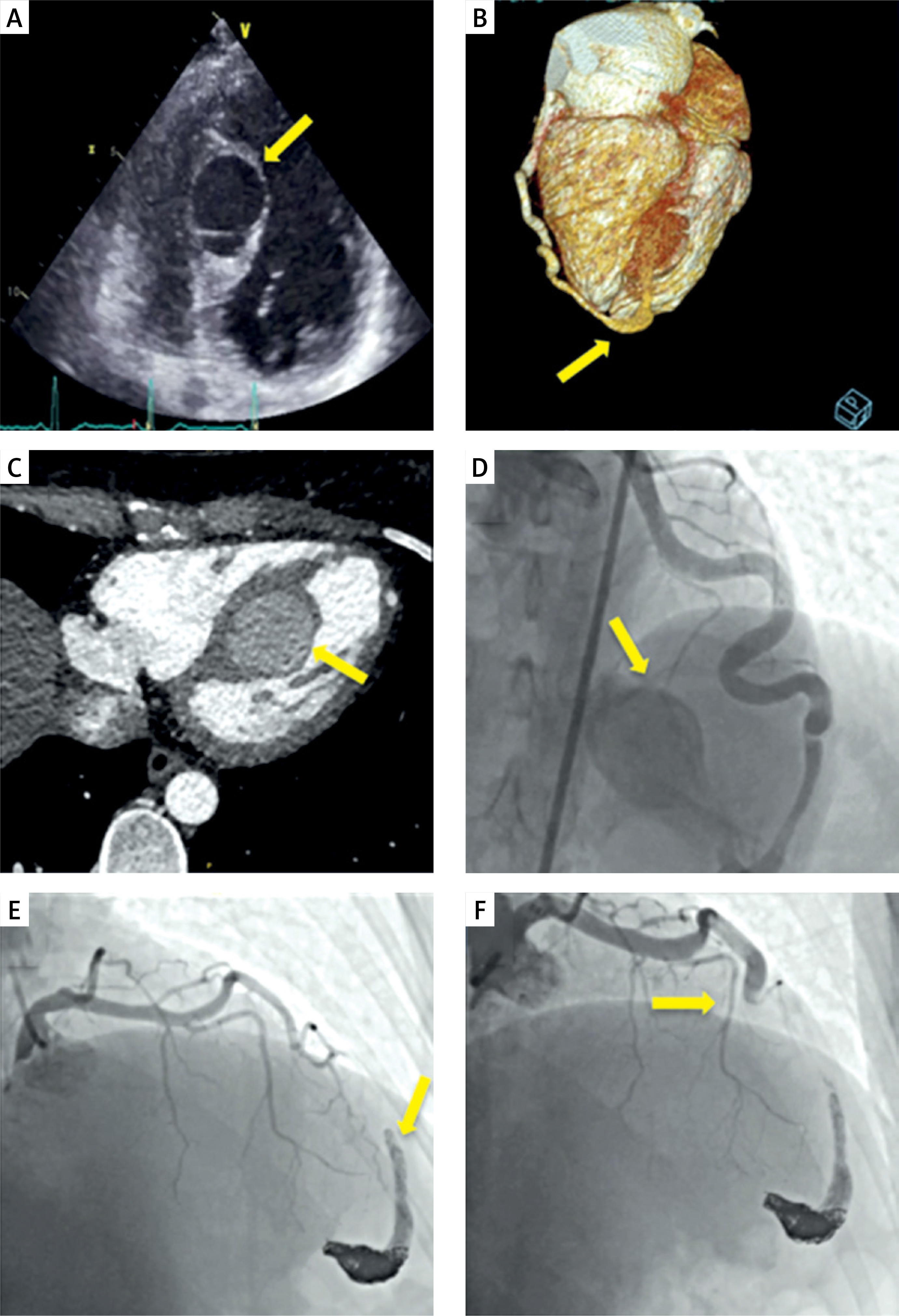
A – A 25 × 23 mm spherical hypoechogenic aneurysmatic structure (yellow arrow) in the interventricular septum. B – 3-D cardiac computed tomography angiography showing the spatial relationship of the aneurysm (yellow arrow). C – A 27 × 37 mm aneurysm (yellow arrow) at the midventricular level of the interventricular septum. D – Coronary angiography (LAO caudal view) showing the dilated and ectatic diagonal artery with abnormal flow into the interventricular septal aneurysm (yellow arrow). E – Coronary angiography (RAO cranial view) demonstrating the thin left anterior descending artery with reduced flow (yellow arrow). F – Post-intervention coronary angiography showing complete occlusion of the fistula (yellow arrow)
Initially, a hydatid cyst was considered in the differential diagnosis due to the septate appearance and history of animal contact. Cardiac computed tomography angiography (CCTA) revealed a 27 × 37 mm aneurysm at the midventricular level, visible in both 3D reconstruction (Figure 1 B, yellow arrow) and axial view (Figure 1 C, yellow arrow). Abdominal computed tomography (CT) and serological tests excluded a hydatid cyst.
While CCTA suggested that the left anterior descending artery (LAD) was feeding the aneurysm, coronary angiography revealed that the diagonal artery was actually dilated and ectatic, draining into the IVS aneurysm (Figure 1 D, yellow arrow). The LAD appeared thin, with reduced flow secondary to the coronary steal phenomenon (Figure 1 E, yellow arrow), explaining the patient’s symptoms.
Percutaneous closure was performed using an 8F guide catheter to cannulate the left main coronary artery. A microcatheter (Cerenovus, Prowler Select Plus, Johnson & Johnson, USA) was navigated into the aneurysm through the ectatic diagonal artery. A 6 × 9 mm Balt balloon (Balt, Eclipse, France) was inflated at the aneurysm neck. Multiple coils (9 × 30 cm, 8 × 30 cm, 6 × 20 cm, and 3.5 × 9 cm Helix, Concerto, Medtronic, USA) were deployed proximal to the balloon. Initial coil embolization resulted in minimal residual filling of the aneurysm. Complete occlusion was achieved using Onyx (34L, Medtronic, USA) and Magic Glue (Balt, Montmorency, France), resulting in immediate restoration of LAD flow. The patient was prescribed dual antiplatelet therapy with acetylsalicylic acid and clopidogrel for 3 months, with a plan to transition to single antiplatelet agent during follow-up.
At 2-month follow-up, the patient was asymptomatic. Transthoracic echocardiography demonstrated significant regression of the aneurysmatic structure in the IVS. Control angiography confirmed complete fistula closure with significantly improved LAD flow (Figure 1 F, yellow arrow). The patient was planned to be evaluated with TTE at 6 and 12 months and with CCTA at 12 and 36 months.
Coronary arterial fistulas are rare congenital or acquired coronary artery abnormalities in which blood is shunted to other vascular beds or cardiac chambers, bypassing the myocardial vascular network [1]. Interventricular septal aneurysms, if left untreated, can lead to serious complications including heart failure due to volume overload, myocardial ischemia from coronary steal phenomenon, aneurysm rupture with potential tamponade, infective endocarditis, and arrhythmias [2]. Given the progressive course and poor prognosis of these lesions, early diagnosis and surgical intervention are imperative for optimal outcomes. Several treatment options exist for coronary artery fistulas, including surgical ligation, coil embolization, vascular plug deployment, and covered stent implantation. Coil embolization is effective for small to medium-sized fistulas but may be complicated by coil migration or incomplete occlusion in larger vessels. Vascular plugs provide more controlled deployment but require adequate landing zones. Covered stents preserve native coronary flow but are limited by vessel tortuosity and risk of stent thrombosis. For our patient, we selected a hybrid approach using both coils and liquid embolic agents due to the complex anatomy, large size of the aneurysm, and need to preserve native coronary flow. This approach provided the advantage of initial framework creation with coils, followed by complete occlusion with liquid agents [3]. Rosic et al. recently described a case of a giant left main coronary artery to right atrium fistula where surgical intervention was required rather than percutaneous closure due to the significant diameter of the fistula and its anatomical relationship with the left main coronary artery, which was successfully treated surgically. These rare variants of coronary fistulas present therapeutic challenges that often necessitate various closure techniques and, when required, surgical treatment approaches to achieve optimal outcomes [4].
This case represents an exceptionally rare variant of coronary arteriovenous malformation with aneurysmal dilatation within the interventricular septum fed by a diagonal branch. To our knowledge, this anatomical variant has not been previously documented in the literature. The successful management through a hybrid transcatheter approach using both coils and liquid embolic agents demonstrates the feasibility of minimally invasive treatment for such complex lesions. This report contributes valuable insights to the evolving body of evidence regarding optimal therapeutic strategies for unusual coronary fistulas with aneurysm formation.







