
Hydatidosis caused by the larval stage of Echinococcus granulosus is the most frequently encountered type of hydatid disease in humans [1, 2]. Due to the close association that exists among sheep and dogs and humans, it is endemic to many parts of the world, particularly the Mediterranean countries including Turkey, the Middle East, South America, Africa, New Zealand, the Russian Federation, Central Asia, and Australia [2, 3]. Of all the body organs, lungs are second only to liver in terms of the disease involvement in adults and, due to their compressible nature and the presence of negative pressure, are the most common site of involvement in children [1, 4]. The most frequently involved organ is the liver (65%) because most of the embryos are trapped within it. Other involved sites are the lungs (25%), and less frequently, the spleen, kidneys, heart, bone, and central nervous system [5]. Structurally, the hydatid cyst of the lung has three layers: pericyst, ectocyst, and endocyst [2, 6]. Multiple protoscolices develop on the inner surface of the germinal layer, differentiate into secondary cysts when cyst ruptures, and form free floating daughter cysts within the mother cyst. Clinically, a small hydatid cyst in the lung often causes no symptoms and they usually remain asymptomatic, while a large one may cause compressive symptoms such as chest pain, coughing, dyspnea, and hemoptysis as well as allergic reactions including anaphylaxis [7]. Importantly, a ruptured pulmonary hydatid cyst into the neighboring or remote cavity spontaneously or iatrogenically is called as “complicated cyst” and it is associated with higher postoperative morbidity and mortality [8]. Interestingly, pulmonary cysts do not calcify, and daughter cyst formation is rare, unlike hydatid cysts located in other surrounding structures such as the pleural cavity, mediastinum and pericardium [2]. The local complications of pulmonary hydatidosis can be classified as rupture (perforation), secondary infection, reactions of the adjacent tissue, and complications associated with space occupation. Rupture, with a reported incidence of 49%, is the most frequent complication of pulmonary hydatid disease [2, 4, 6, 9]. Rupture into the pleural cavity may occur if a live scolex seeds into the pleural cavity as a result of rupture of an intrapulmonary cyst [7]. Pleural manifestations may develop as a complication of pulmonary hydatid disease, which do not involve a parasitic infestation [10, 11]. The rupture of a hydatid cyst into the pleura can cause a wide range of clinical and radiological symptoms, such as pneumothorax, hydropneumothorax, empyema, abscess formation, pleural thickening, and tension pneumothorax, to develop in the pleural area. The diagnosis is sometimes very difficult and even confused with malignancies. Perforated hydatid cysts emerge as a distinct entity that should especially be considered in differential diagnoses. Opening of the hydatid cyst to the pleura can be spontaneous and can be traumatic or iatrogenic [8, 11]. Due to the perforation of the pulmonary hydatid cyst into the pleura, symptoms such as chest pain, coughing, cyanosis, fever, and shortness of breath develop. As a result of the rupture of the cyst, the cyst contents pour into the pleura, and the ruptured germinative membrane collapses. Therefore, signs of compression occur in the latent lung parenchyma.
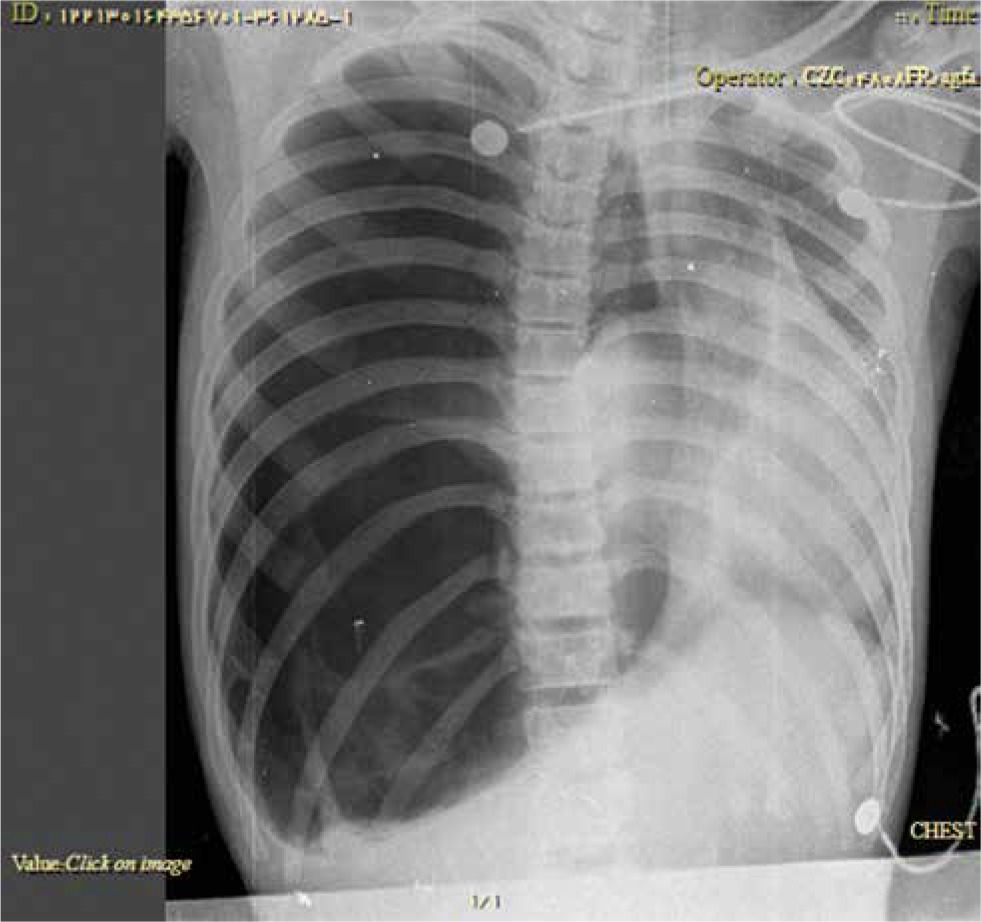
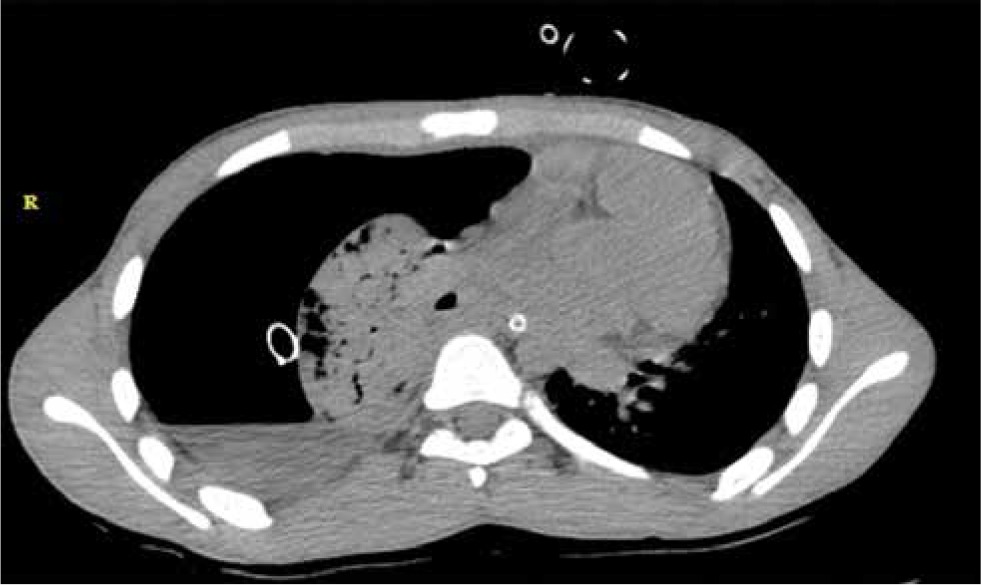
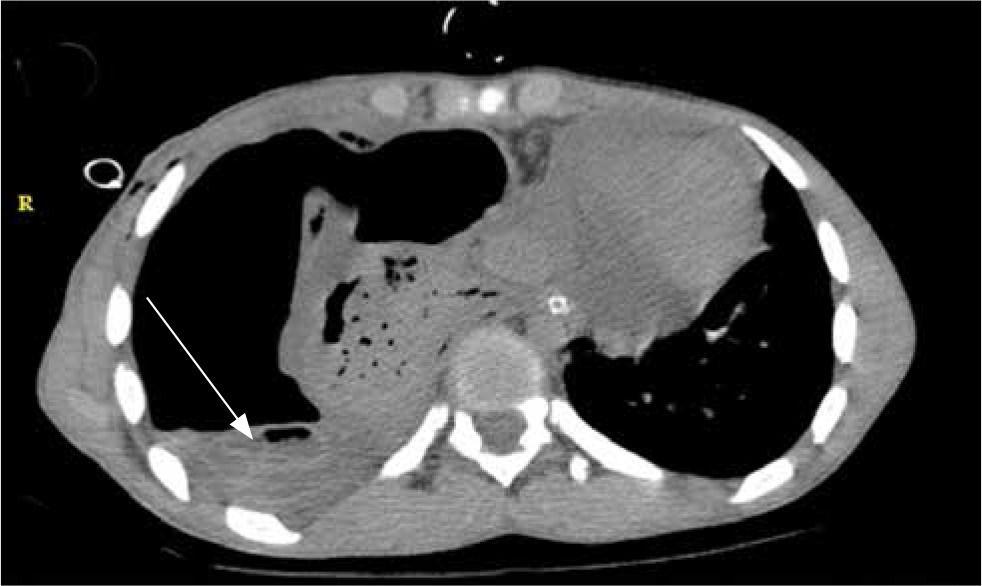
A 16-year-old male patient presented to our emergency department with sudden onset of breathlessness. He was alert and found to be tachypnoeic (respiratory rate 40/minute) with an oxygen saturation of 82% while breathing oxygen through a facemask was at 15 l/minute. His pulse rate was 130/minute and blood pressure 90/70 mm Hg. Suddenly he progressed to cardiopulmonary arrest and so instantly became intubated and cardiopulmonary resuscitation (CPR) began. Fortunately he responded to CPR successfully. After that a portable CXR was taken. The CXR showed tension pneumothorax in the right side with complete collapse of the right lung (Figure 1). So the patient underwent tube thoracostomy with a 32F chest tube at bedside in the emergency department (Figure 2). A lot of air came out of the chest tube. The patient was admitted to the intensive care unit (ICU) and his saturation improved to above 90% and he remained hemodynamically stable. A spiral chest computed tomography (CT) scan was performed, which confirmed right side pneumothorax, right lung collapse (Figure 3) and the crumpled endocyst membranes floating freely on the top of remaining cyst fluid (Figure 4, water lily sign). The chest tube was lying outside the cyst cavity. The decision was made to perform surgery. After the general anesthesia and one-lung ventilation, and left lateral position, our patient underwent right posterolateral thoracotomy. Severe empyema was in the thoracic cavity and the lung was completely collapsed. The germinative layer of the hydatid cyst was obvious in the thoracic cavity that was removed. The hydatid cyst cavity was in the right lower lobe. There was a thick peel on the lung surface and pleura. The peel was completely removed (decortication). The hydatid cyst site in right lower lobe (RLL) was removed with wedge resection. Then the lung parenchyma was repaired with 3-0 absorbable suture. After placement of two chest tubes, the thoracic wall was repaired. Postoperatively, he was extubated. In the following postoperative days, the right lung was fully expanded. He was receiving albendazole 600 mg/day as well. He was discharged from hospital after removal of chest tubes and was doing well on follow-up later.

Pulmonary hydatid cysts and their complications have been recognized since the time of Hippocrates [11]. A pulmonary hydatid cyst does not produce symptoms unless it reaches a large size to show signs of lung compression or becomes complicated. When a pulmonary hydatid cyst becomes complicated, it can result in serious clinical outcomes. Cysts that open to the pleura or bronchia and then become infected develop a number of pleural and parenchymal complications, a condition known as a complicated cyst. Complicated cysts are difficult to diagnose. In perforated cysts, the clinical situation varies depending on the characteristics of the perforation and whether the cyst ruptures into the pleura or the bronchia. Three different types of cyst ruptures have been described: contained, communicating, and direct. Contained ruptures related to degeneration, trauma, or response to therapy occur when the endocyst ruptures, but the pericyst remains intact [6]. Communicating rupture occurs when the contents of the cyst escape via biliary or bronchial radicles that are incorporated in the pericyst [6]. Direct rupture occurs when both the pericyst and endocyst rupture, allowing free spillage of hydatid material into the pleural cavity, hollow viscera, thoracic wall, and so on. Direct rupture is more frequent in lesions located in the periphery of the lung, where there may be less protection for the cyst due to a deficient pericyst and little host tissue to offer support [2]. In communicating and direct ruptures, the cyst empties and may become smaller and less spherical [2]. In contrast to perforation into a bronchus, rupture of a hydatid cyst into the pleura usually causes simple or tension pneumothorax, pleural effusion, or empyema, and symptoms such as chest pain, coughing, cyanosis, fever, and shortness of breath develop. Severe clinical manifestations, such as tension pneumothorax, can sometimes occur as a result of a bronchopleural fistula. Cernay identified tension pneumothorax in 5 out of 336 patients in a case series (1.3%) [12]. Bakir et al. reported a case series consisting of 5 cases of tension pneumothorax [13]. Chacko et al. reported tension pneumothorax in a 35-year-old man with lung hydatid cyst [14]. Our patient was a 16-year-old male who presented with cardiac arrest due to tension pneumothorax associated with lung hydatid cyst. Hydatid cyst is a continuously growing parasite. Its expansion is usually limited by the tissue and organ of the host, though this characteristic in the lung parenchyma is minimal and poor as compared with that of other organs. Pulmonary echinococcal cysts may reach a huge size during growth, the eroding blood vessel often giving rise to hemoptysis. The bronchial passages could be eroded as well and air escapes around or into the cyst, which accounts for the various radiological features in this disease. The eroded bronchus does not function as a fistula to start with, due to the pressure of the tense cyst against the fistula opening. Progressive enlargement will lead to its rupture either into the bronchial tree or into the pleura. Intrapleural rupture more frequently presents as pneumo- or hydropneumothorax. The pneumothorax may be tension in type, as in the above cases, where it is quite easy to visualize the tension or the valvular mechanism. The collapsed or crumpled wall of a ruptured cyst simply acts as a curtain or check valve, admitting air into the pleura during inspiration, then falling back and closing the opening or outlet during expiration, and thus allowing air to enter but not to escape from the pleural cavity. A positive pressure will continuously build up inside the pleural cavity which will ultimately shift the mediastinal structures to the opposite side, interfering with the hemodynamics of the respiratory and cardiovascular systems. These changes are responsible for the clinical picture usually seen in tension pneumothorax, which may be fatal if the tension is not relieved. A sudden rise in the intrapulmonary pressure is the usual precipitating factor in rupture of the cyst: the cause could be a trivial one, such as coughing or sneezing, though sometimes it may follow an increase in intraabdominal pressure as in pregnancy or ascites. Rupture may occur spontaneously without any predisposing factor [14]. Ruptured hydatid cyst should be considered in patients who present with sudden onset of respiratory distress and hypoxia in geographical areas where the disease may be prevalent.
In endemic area for hydatid disease, correct understanding of physicians about hydatid disease, its pathophysiology and complications can help them to diagnose and manage the patients better.









