
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most common chronic liver disease worldwide and one of the leading causes of cirrhosis, hepatocellular carcinoma and liver transplantation in developed countries, as well as an important cardiovascular risk factor. It affects about 30% of the adult population and about 10% of the paediatric population. These figures may be underestimated due to the long-standing asymptomatic or sparse course of the disease, the lack of nationwide screening for MASLD in patients with risk factors for its development and the low awareness of both patients and physicians themselves. According to projections, this number could double by 2030 due to the growing obesity epidemic and the associated development of other weight-dependent metabolic complications, such as insulin resistance, pre-diabetic state, type 2 diabetes, lipid disorders or hypertension, which are the main causes of the development of MASLD [1–4].
Lack of prophylaxis and late diagnosis of MASLD lead to hepatic complications – increased hepatic steatosis, steatohepatitis, progression of hepatic fibrosis, development of cirrhosis or hepatocellular carcinoma – and extrahepatic complications, mainly cardiovascular: arteriosclerosis, ischaemic heart disease (myocardial infarction or stroke) (Table 1). Cardiovascular disease, not hepatic complications, is the main cause of death in patients with MASLD [1, 2].
Table 1
Hepatic and extrahepatic complications of MASLD
Hence, it is not uncommon for the disease to be diagnosed relatively late, after a cardiovascular incident or at the stage of advanced liver fibrosis or cirrhosis.
Imaging methods are used in the diagnosis of hepatic steatosis. Ultrasound has been applied most frequently because of its availability, low cost of performance and relatively high sensitivity and specificity. However, ultrasound detects steatosis only when 20-30% of hepatocytes are involved, and therefore relatively late. According to the recommendations of American scientific societies, patients with risk factors for the development of MASLD – obesity, diabetes, hypertension or dyslipidaemia – should undergo liver elastography with the FibroScan method in order to detect steatosis at an early stage – when steatosis affects 5% of hepatocytes. FibroScan can also be used to assess the severity of steatosis related to the Brunt scale or liver fibrosis related to the METAVIR scale in patients diagnosed with MASLD and to assess the risk of developing metabolic dysfunction-associated steatohepatitis (MASH) or other liver complications using specific scales: FAST, Agile 3 and Agile 4. Computed tomography (CT) or magnetic resonance imaging (MRI) is also used to assess hepatic steatosis; however, due to their availability and cost, they are not routinely used for diagnosis. Liver biopsy, although the gold standard, is currently used rarely for the diagnosis of MASLD. It is mainly reserved for doubtful cases, overlap syndromes or the diagnosis of MASLD or cirrhosis [1, 5].
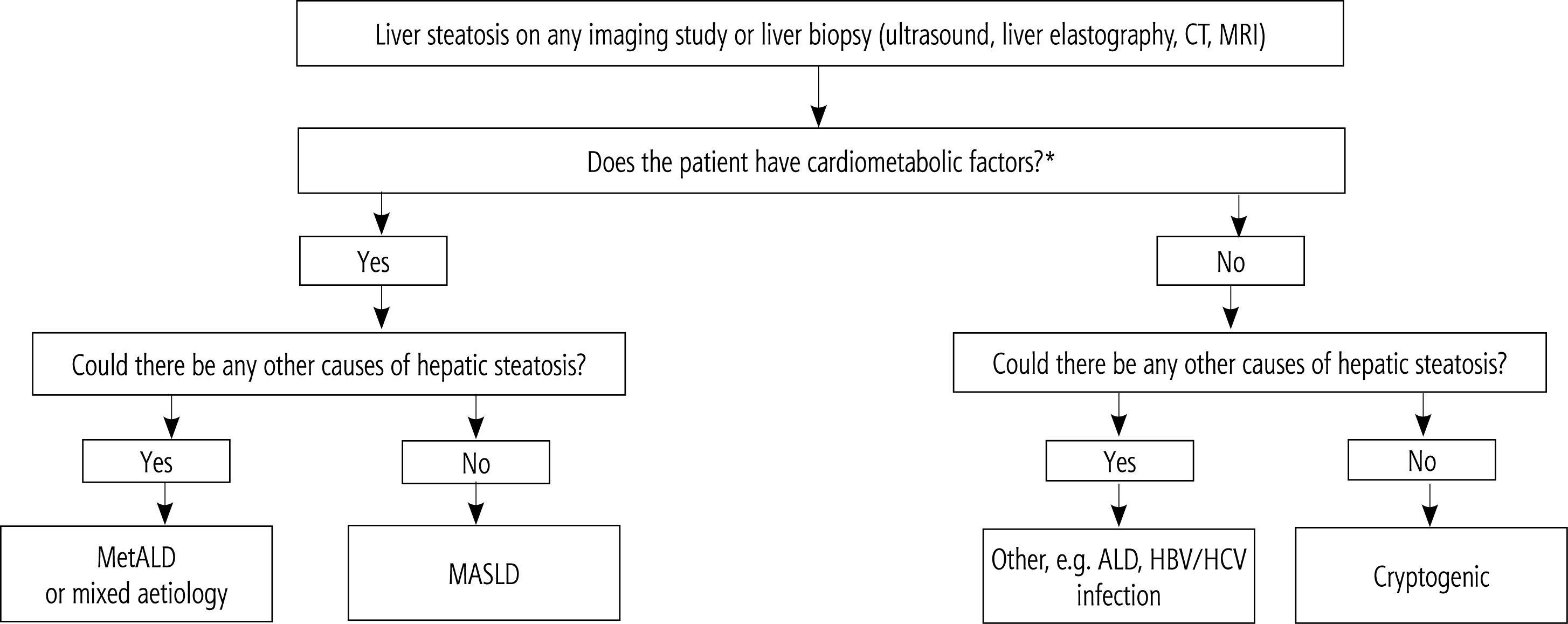
The diagnosis of hepatic steatosis in MASLD also requires the exclusion of other potential causes of hepatic steatosis such as alcohol consumption, drugs, viral hepatitis and others (Figs. 1, 2).
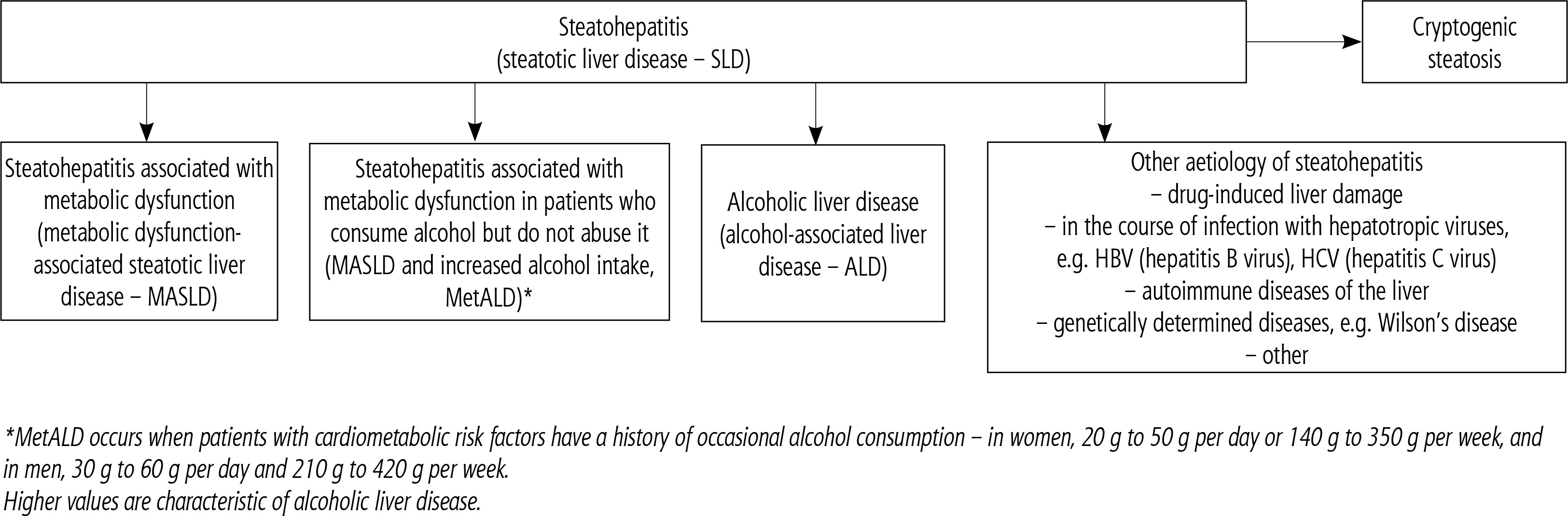
Fig. 2
Algorithm for management of patients with hepatic steatosis
*Cardiometabolic factors considered in patients with suspected MASLD:
– BMI ≥ 25 kg/m2 or waist circumference ≥ 94 cm in men and ≥ 80 cm in women (or above normal depending on ethnicity),
– blood pressure ≥ 130/85 mm Hg or treatment of hypertension,
– serum triglyceride concentration ≥ 1.7 mmol/l (150 mg/dl) or treatment of hypertriglyceridaemia,
– serum HDL (high-density lipoprotein) cholesterol concentration ≤ 1.0 mmol/l (< 40 mg/dl) in men and ≤ 1.3 mmol/l (< 50 mg/dl) in women or treatment of hypercholesterolaemia,
– fasting glucose ≥ 5.6 mmol/l (100 mg/l) or 2 h after a glucose load ≥ 7.8 mmol/l (140 mg/dl) or HbA1c ≥ 5.7% (39 mmol/mol) or type 2 diabetes or treatment of type 2 diabetes.
Despite medical advances, there is still no effective pharmacological treatment strictly reserved for the treatment of hepatic steatosis, steatohepatitis or progressive liver fibrosis in the course of MASLD.
There are currently 3 main pillars in the therapeutic management of patients with MASLD:
– Pillar I is the treatment of obesity-related disease, with a target weight reduction of 10% of baseline weight within 6 months [1]. It has been shown that sustained weight reduction can reduce or reverse hepatic steatosis depending on its severity and reduce the initial stages of liver fibrosis. Based on an analysis of 4 randomised trials, a weight reduction of at least 3% results in a reduction in steatosis in 35-100% of patients depending on the severity, a reduction in weight of at least 5% reduces the severity of ballooning degeneration/inflammation in 41-100% of patients, a further weight reduction of at least 7% reduces the severity of MASH in 64-90% of patients, while a weight reduction of at least 10% results in regression of fibrosis (F1-F2) in 49% of patients;
– Pillar II is the elimination of cardiometabolic risk factors – the main cause of premature mortality in patients with MASLD – i.e. appropriate treatment of diabetes, lipid disorders and hypertension;
– Pillar III, on the other hand, is the use in patients with diagnosed and confirmed steatohepatitis of drugs that have demonstrated in clinical trials the ability to reduce MASH and/or regress liver fibrosis – pioglitazone, vitamin E, glucagon-like peptide-1 (GLP-1) or GLP-1/gastric inhibitory polypeptide (GIP) analogues, etc. [1, 6–8].
Potential pharmacological options in MASLD
Although, at this point in time, no drug has gained U.S. Food and Drug Administration (FDA) approval specifically for the treatment of hepatic steatosis, given the diseases that are the underlying causes of this condition (including components of the metabolic syndrome – insulin resistance-related: obesity, carbohydrate and lipid metabolism disorders, blood pressure) and its complications (fibrosis, cirrhosis), a variety of pharmacotherapy pathways are used in clinical practice [9–11].
GLP-1 analogues are a broad group of incretin mimetic drugs finding recognition in the modern treatment of type 2 diabetes, obesity and their comorbidities (diabesity). GLP-1 analogues increase post-meal insulin secretion, inhibit glucagon secretion, reduce excess hepatic glucose secretion, decrease lipogenesis, delay gastric emptying, exhibit anti-inflammatory effects and act on the hunger and satiety centres located in the hypothalamus [12, 13]. In 2014, it was reported that in patients with diabetes, exenatide had a beneficial effect on reversing hepatic steatosis (the comparator for exenatide in this case was insulin) [14]. In the same year, Bi et al. also found a benefit from exenatide in this respect, although here a difference between aGLP1 and pioglitazone or insulin was not proven at the same time [15]. Two years later, another representative of aGLP1, liraglutide, was found in the LEAN study to be effective in reducing both steatosis and liver fibrosis [16], which was also confirmed by subsequent studies from other scientific groups [17–19] (although not all – for example, Smits et al., in a 12-week study comparing the use of liraglutide and sitagliptin in patients with type 2 diabetes, found that neither drug showed a significant difference in intrahepatic fat accumulation relative to the placebo group [20]). The D-LIFT study evaluating the efficacy of dulaglutide showed that the drug reduced intrahepatic fat volume by approximately 26.4% with 24 weeks of use, but had no statistically or clinically significant effect on reducing perihepatic fat volume or the fibrotic process [21]. Semaglutide (which is the only GLP-1 analogue available in both oral form and subcutaneous injection) in a study by Gad et al. showed beneficial effects on both the reduction of steatosis and liver fibrosis (assessed after 6 and 12 months of drug use), with semaglutide used in weekly subcutaneous injections performing best in both analyses [22] – this was de facto confirmation of previous reports of the efficacy of this drug in the treatment of MASLD, while also noting the clinically relevant articulation of differences between different forms of delivery of the same active substance. With all the above information in mind, the use of GLP1 analogues should be considered as one of the first-line treatments for liver steatosis associated with metabolic disorders [23, 24].
A somewhat distinct group of drugs is that of the dual GLP-1 and GIP receptor agonists. Glucose-dependent insulinotropic peptide (GIP) is another incretin mimetic hormone that, when secreted by the small intestine, increases insulin sensitivity and, similar to GLP-1, has a beneficial effect on fat metabolism [24]. At the moment, the only GLP-1 and GIP dual agonist preparation approved worldwide is tirzepatide, for which the 2022 SURPASS-3 MRI study demonstrated high efficacy at doses of 10 and 15 mg in reducing intrahepatic fat. Given the short time of availability of the drug, further results of studies on the observation of long-term or long-distance complications should be patiently awaited [25, 26]. Other dual agonists – cotadutide, survodutide and efinopegdutide targeting GLP-1 and glucagon receptors – also demonstrated a favourable impact on hepatic fat content and noninvasive fibrosis scores in clinical trials involving MASLD patients. Nonetheless, caution is warranted before making definitive conclusions, given the ongoing status of these trials [27–29].
Another drug, this time a triple agonist (for GIP, GLP-1 and the receptor for glucagon), is retatrutide, currently only available in clinical trials. Although it will be some time before the drug is on the full market, in the promising trial results to date, all doses of retatrutide produced a significant reduction in liver fat compared to placebo [30, 31].
Another group of drugs with incretin-mimetic effects are the dipeptidyl peptidase 4 (DPP4) inhibitors. These are weak hypoglycaemic drugs, mainly used in the initial stages of type 2 diabetes treatment, showing a neutral or minimally positive effect on weight reduction. Data on their real effect in the treatment of hepatic steatosis are limited. Vildagliptin has been proven to have a marginally significant beneficial effect on intrahepatic lipid accumulation, but this is not sufficient to recommend the use of gliptins in the treatment of MASLD (although, on the other hand, international bodies agree that their use in the treatment of patients with type 2 diabetes and concomitant fatty liver disease is safe in principle) [32].
Metformin is an antidiabetic drug, a biguanide derivative whose primary mechanism of action is to increase the sensitivity of peripheral tissues to insulin. Chronic therapy (lasting a minimum of 2.8 years) results in an average weight reduction of 2.5%, so ostensibly metformin could be a beneficial drug in the treatment of hepatic steatosis. However, this is not the case – the use of metformin has not been confirmed in sufficiently high-quality studies to date to be associated with beneficial changes in hepatic lipid architecture [33, 34].
Sodium-glucose cotransporter-2 (SGLT-2) inhibitors are drugs designed to increase renal resorption of glucose. They are used in the treatment of type 2 diabetes, but at the same time, due to their considerable proven cardioprotective benefits, these drugs have also found favour with cardiologists and nephrologists, who have begun to use them in the treatment of chronic heart failure and chronic renal failure [35]. Glucosuria results in weight loss, averaging 1.8 kg after 12 weeks of treatment in patients with pre-existing hyperglycaemia. In 2018, Kuchay et al., as part of the E-LIFT study, found that empagliflozin used in patients with type 2 diabetes at a dose of 10 mg daily for 20 weeks was associated with a 5% reduction in liver fatness [36]. In the same year, another group found that dapagliflozin used in a similar group of patients reduced the CAP parameter on liver elastography by approximately 10%, while having no statistically significant effect on liver fibrosis (except in the most stressed group, with measurements exceeding 8 kPa) [37]. A pooled analysis of randomized controlled trials of various SGLT-2 inhibitors by Mantovani et al. showed that iSGLT-2 (with particular emphasis on empagliflozin and dapagliflozin) significantly reduce intrahepatic lipid accumulation [31]. The results so far seem promising, but further, more extensive studies targeting the efficacy of treatment of hepatosteatosis sensu stricto should be patiently awaited.
A special place in the EASL-EASD-EASO (European Association for the Study of the Liver, European Association for the Study of Diabetes, European Association for the Study of Obesity), AASLD (American Association for the Study of Liver Diseases) and APASL (Asian Pacific Association for the Study of the Liver) guidelines for the management of MASLD is occupied by pioglitazone, which is a selective peroxisome proliferator-activated receptor γ (PPARγ) agonist leading to an increase in tissue sensitivity to insulin and therefore a reduction in insulin resistance in adipose tissue, skeletal muscle and liver cells, with a concomitant reduction in free fatty acids and blood glucose [1]. According to the available studies, six-month treatment with pioglitazone effectively reduces hepatic steatosis and inflammation in patients with pre-diabetes and type 2 diabetes [15, 38, 39]. Cusi et al.’s group demonstrated that long-term (18-month) treatment also has a beneficial effect on fibrosis. A subsequent meta-analysis by Lian and Fu confirmed a beneficial effect on hepatic steatosis but not on fibrosis [38, 39]. Despite the above, due to the side effects of pioglitazone, such as hypoglycaemia, increased risk of osteoporotic fractures, weight gain, possible onset or exacerbation of heart failure, and risk of bladder cancer, this therapy is questionable and not widely used.
Fibrates, which are also PPAR agonists, show beneficial effects on the dyslipidaemia accompanying MASLD. The benefits include both a reduction in biochemical activity and a positive effect on histology (in terms of ballooning degeneration). Short treatment with bezafibrate (2-8 weeks) in combination with diet and increased physical activity reduced fine steatosis. Short 4-week treatment with gemfibrozil for MASH led to a reduction in aspartate aminotransferase (AST) and γ-glutamyltranspeptidase (GGTP) activity, while no benefit was demonstrated with 1 year of clofibrate therapy [40].
Orlistat is a long-acting inhibitor of gastric and pancreatic lipase, designed to reduce the absorption of triglycerides from the gastrointestinal tract by approximately 30%. It is thus used in the treatment of obesity, where it causes a reduction in body weight of approximately 5-10%. The results of studies to date on the reversal of hepatic steatosis are inconsistent. On the one hand, we have results confirming such a positive consequence of the use of the drug; on the other hand, we also have the results of a study in which patients on a diet with vitamin E and randomised to orlistat or placebo did not show that orlistat led to a histopathologically confirmed reduction in hepatic steatosis (which would suggest that it was vitamin E, not orlistat, that was the key element in the treatment of steatosis) [41–44]. Interestingly, vitamin E can be found in official guidelines for the management of metabolic dysfunction–associated fatty liver disease (MAFLD), and this is due to its antioxidant properties. A study by Xu et al. found that high doses of vitamin E (800 mg/d) can lead to normalisation of biochemical activity, as well as a reduction in steatosis and inflammation and even ballooning degeneration in patients without diabetes, although without improvement in fibrosis [45]. With regard to orlistat, however, a meta-analysis was published in 2024, which proved that this drug effectively and independently reduces peri-umbilical localised fat [46]. The main problem with the use of orlistat is its side effects – bloating, abdominal pain, fatty diarrhoea, skin lesions, impaired absorption of fat-soluble vitamins (A, D, E, K) requiring the implementation of adequate supplementation. Due to the potential impact of vitamin E on the incidence of prostate cancer in men > 50 years of age and on the risk of stroke, it is currently rarely used. Vitamin E is not recommended in patients with diabetes or cirrhosis [47, 48].
An important component of the metabolic syndrome, also linked to MASLD, is dyslipidaemia. Statins, i.e. 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase inhibitors, are well-studied preparations with a well-established role in the treatment of dyslipidaemia. Nevertheless, it should be noted that, worldwide, treatment with these preparations is suboptimal; the results of the Khoo et al. study indicated that 59% of patients who do not take statins should take them, and 74% of patients taking statin therapy use them in a way that prevents them from achieving their therapeutic goal. A 2023 multivariate study by Ayad et al. showed that statin therapy significantly reduces intrahepatic fat concentrations (the risk of developing non-alcoholic fatty liver disease [NAFLD] with such therapy decreases by up to 31%) – an association was also identified between the use of simvastatin and lovastatin and the inhibition of genes acting on the expression of sterol regulatory element-binding protein 1 (SREBP-1) and patatin-like phospholipase domain-containing protein 3 (PNPLA-3), which may be one of the main factors contributing to this efficacy of therapy [49, 50]. Statins, in particular, have beneficial effects on the liver in MASLD through their pleiotropic effects such as antioxidant, antiproliferative, anti-inflammatory, immunomodulatory, normalising endothelial function. The beneficial effects of statins on the liver, proven in numerous studies clinical trials, include: reduction in the severity of inflammatory changes, reduction in fibrosis and steatosis, reduction in portal pressure, reduction in disease progression in patients with cirrhosis, reduction in the risk of hepatocellular carcinoma in patients with cirrhosis, and increased survival [1, 51]. Ezetimibe, which selectively inhibits cholesterol absorption in the small intestinal stroma, when added to statin therapy, produces an even greater improvement in the reduction of peri-hepatic fatness, according to the results of the ESSENTIAL trial (although, at the same time, this drug has no effect on liver fibrosis). According to the current Polish guidelines for the clinical management of patients with MASLD (coinciding with those of other scientific societies), hypolipemic therapy is recommended as for the general population [52, 53].
Ursodeoxycholic acid (UDCA) is a natural, hydrophilic bile acid that inhibits intestinal absorption of cholesterol, reducing its secretion into bile (leading to a 40-60% reduction in bile cholesterol concentration) while showing pluripotent effects on the liver associated with cytoprotection and immunomodulation. To date, this drug has not been included in treatment recommendations for MASLD, despite showing beneficial effects on hepatic steatosis and gut microbiota in an animal model. However, the results in humans were different: a randomised study by Dufour et al. showed a beneficial effect of UDCA on hepatic steatosis, but only in combination with vitamin E; several years later, high doses of ursodeoxycholic acid (23-28 g/kg/day) failed to achieve histopathologically recordable improvements in patients [54–56].
An interesting fact worth including in this review is that, since disruption of the microbiota is identified as one of the potential causes of the development of hepatic steatosis, it is likely that the use of probiotics will have a beneficial effect on treatment. Intestinal dysbiosis can influence the development and progression of MASLD through a number of metabolic, immunological and inflammatory mechanisms. It can cause increased intestinal permeability (so-called leaky gut syndrome). Dysbiosis leads to damage of the intestinal barrier, which facilitates the passage of bacterial toxins (e.g. lipopolysaccharides – LPS) into the bloodstream, activating the immune system and causing chronic inflammation and oxidative stress in the liver [57]. LPS activates Toll-like receptors (TLR4) in hepatocytes and Kupffer cells, exacerbating steatosis and inflammation. Dysbiosis can increase endogenous ethanol production by bacteria, which has a toxic effect on the liver. Also, excess secondary bile acids can affect lipid metabolism and cause insulin resistance. Disruption of the gut microbiome also disrupts the balance between protective short-chain fatty acids (SCFAs) such as butyrate and those that can promote lipogenesis (e.g. acetate, propionate). In turn, excess SCFAs can be a substrate for lipid production in the liver, exacerbating hepatic steatosis. Intestinal dysbiosis also increases calorie absorption from the diet and promotes insulin resistance, leading to excessive fat accumulation in the liver. It affects hormonal pathways, such as GLP-1 and fibroblast growth factor 19 (FGF19), which regulate liver metabolism. Typically, patients with obesity and MASLD show a reduction in microbiota diversity. There is an increase in pro-inflammatory bacteria: overgrowth of Enterobacteriaceae (e.g. Escherichia coli) and an increase in endotoxin-producing bacteria (e.g. Proteobacteria), while there is a decrease in protective bacteria such as Faecalibacterium prausnitzii (with anti-inflammatory effects) and Akkermansia muciniphila, which supports the integrity of the intestinal barrier [58, 59].
An appropriate diet – rich in vegetables, fruit and fermented products such as kefir, yoghurt or pickles – with restriction of simple sugars, saturated fats, alcohol and cigarettes, is beneficial in the treatment of intestinal dysbiosis. Prebiotics, such as dietary fibre (e.g. inulin, oligofructose), support the growth of beneficial bacteria, while postbiotics, such as products of bacterial metabolism (e.g. butyrate), can support the regeneration of the intestinal epithelium. Indeed, according to previous reports, appropriately selected probiotic treatment (and especially in combination with symbiotics) may have beneficial effects in the ancillary treatment of steatosis and liver fibrosis – these would be mainly formulations based on Bifidobacterium longum, Lactobacillus paracasei, Lactobacillus johnsonii, Lactobacillus reuteri and others, which would be expected to reduce insulin resistance, the negative impact of dyslipidaemia and features of systemic inflammation. Experimental studies are also investigating the effect of transfer of the gut microbiota on MASLD [60–62]. Also, some of the drugs used to treat MASLD have a beneficial effect on the composition of the gut microbiota, e.g. UDCA or GLP-1 analogues [59].
New drugs are being developed for treatment of MASLD
Resmetirom was the first FDA-approved medication for the indication of MASH without cirrhosis [63]. Thyroid hormones in the liver promote lipid export and oxidation, along with de novo lipogenesis, while suppressing hepatic gluconeogenesis. These effects are mediated by thyroid hormone receptors (THRs), which directly affect gene expression, particularly in the liver isoform β (also found in cardiac ventricles) [64]. Resmetirom is a highly selective orally active THR-β agonist. The finding of the phase 3 clinical trial MAESTRO-NASH indicated that MASH without deterioration of fibrosis was observed in 25.9% of the 80 mg cohort and 29.9% of the 100 mg cohort, in contrast to 9.7% in the placebo group. Fibrosis improvement without exacerbation of MASH occurred in 24.2% of the 80 mg group and 25.9% of the 100 mg group, in contrast to 14.2% in the placebo cohort. Fibrosis improvement by ≥ 2 stages occurred in 8.3% of the 80 mg group and 10.1% of the 100 mg group, compared to 2.8% in the placebo group [65, 66]. Vidal-Cevallos et al. determined the number needed to treat (NNT): it ranged from 5 to 6.25 for NASH resolution without fibrosis worsening, 8.5 to 10 for fibrosis improvement by at least one stage without exacerbation of the steatosis activity score, and 13.7 to 18.2 for fibrosis improvement by at least two stages. Additionally, considering that resmetirom was initially developed for dyslipidaemia treatment (and has been shown to significantly lower LDL-C and triglycerides [67]), the authors speculate whether the drug could reduce cardiovascular risk (although this question will remain unanswered until the conclusion of the clinical trials, anticipated to last 52 months) [68]. This is significant, particularly when considering that, in conjunction with data from phases 2 and 3 studies, resmetirom has exhibited a good safety and tolerability profile, with gastrointestinal adverse events such as diarrhoea and nausea being the most frequently reported (while presumed THRα-related effects, including arrhythmias, were not observed). The FDA has approved the treatment for a once-daily oral dosage of 80 mg or 100 mg, dependent on the patient’s weight (less than or greater than 100 kg); a liver biopsy is not required for prescription [11].
Analogues of fibroblast growth factors (FGF) represent another significant category of drugs deemed potentially advantageous in the treatment of MASLD. FGF21 is a stress-responsive hormone with pleiotropic effects (mostly hepatoprotective), synthesized in the liver and adipose tissue. Its concentrations physiologically rise in reaction to stress associated with, for instance, an inadequate macronutrient composition in the diet (insufficient protein content and/or excessive carbohydrate intake, especially fructose, whose metabolism consumes substantial ATP, imposing significant stress on the liver). Mitochondrial dysfunction, commonly associated with components of the metabolic syndrome (obesity, hyperglycaemia, dyslipidaemia, hypertension, which are also part of the MASLD diagnosis), also generates high levels of oxidative and endoplasmic reticulum stress, which subsequently stimulates the expression of FGF21. FGF also affects the function of thyroid hormones in the liver (by enhancing hepatic deiodinase activity and upregulating expression of the THR-β receptor), as well as the secretion of adipokines of adipose tissue and pancreatic hormones: glucagon and insulin [69–71]. Among the many FGF21 analogue drugs studied, promising results in clinical trials have been shown by drugs such as efruxifermin, pegozafermin and efimosfermin-α [69, 72, 73]. Efruxifermin is a long-acting Fc-FGF21 fusion protein under development for MASH and fibrosis. In the HARMONY phase 2b clinical trial involving 128 patients with MASH and fibrosis grades F2-F3, a minimum one-degree improvement in fibrosis (without exacerbation of MASH) was noted in 39% of patients receiving a 28 mg dose and 41% of those receiving a 50 mg dose, compared to 19% in the placebo group. The treatment maintained an acceptable safety and tolerability profile, with the most prevalent side effect being diarrhoea (affecting 40% of patients) and one serious adverse event related to the drug (esophagitis in a participant with a history of gastroesophageal reflux disease) [74]. Pegozafermin is a long-acting glyco-pegylated recombinant FGF21 analogue administered subcutaneously, currently under development for MASH, fibrosis, and the treatment of severe hypertriglyceridemia. In the phase 3b ENLIVEN trial, involving 219 patients with MASH and F2-F3 fibrosis, 22-30% of patients receiving the drug showed at least a one-grade improvement in liver fibrosis, compared to 7% in the placebo group; additionally, resolution of MASH (without worsening of liver fibrosis) occurred in 23-37% of patients, vs. 2% in the placebo group [75]. Efimosfermin-α is a long-acting, engineered variant of FGF21, designed for a prolonged half-life with monthly administration. A phase 2a study involving 84 patients with biopsy-confirmed MASH and grade F2-F3 fibrosis revealed that 45.2% of patients experienced improvement in fibrosis without exacerbation of MASH (compared to 20% in the placebo group); 67.7% of patients showed improvement in MASH without worsening of fibrosis (vs. 29.4% in the control group); the treatment also resulted in significant reductions in intrahepatic fat among patients exhibiting characteristics of obesity, type 2 diabetes or diabesity [73]. Analogues of fibroblast growth factors represent a promising class of pharmaceuticals, although we must also remember the failures of clinical trials of such promising substances as pegbelfermin (BMS-986036), CVX-343 or LY2405319 [69]. We await the outcomes of the next phases of clinical trials.
In the previous section, we discussed pioglitazone, a conventional PPAR agonist with established efficacy with a proven effect on the course of liver structural problems. However, it is worth mentioning newer representatives of this group, studied in the same context: lanifibranor, saroglitazar, and elafibranor. PPAR is a family of nuclear receptor proteins that are classified as ligand-activated transcription factors, typically categorized into three isoforms: α, β/δ, and γ. The PPAR-α activity may decrease as MASLD progresses clinically, leading to a reduction in fatty acid oxidation and the accumulation of hepatic fat [76]. Lanifibranor is a pan-PPAR agonist, evidenced in the six-month NATIVE phase 2b study (involving 247 patients with MASH, with and without type 2 diabetes) to achieve at least a 2-point enhancement in the SAF-A score (the activity component of the Steatosis, Activity, Fibrosis scoring system that includes assessments for ballooning and inflammation) without exacerbating fibrosis in 48-55% of patients (compared to 33% in the control group), resolution of MASH without worsening of fibrosis (39-49% in the treated group vs. 22% in the placebo group), and improvement of fibrosis by at least 1 degree without worsening of MASH (34-48% in the drug group vs. 29% in the control group). Improvements were noted in liver enzyme activity, inflammation biomarkers, and lipid parameters, although it is important to mention that the drug was associated with a higher incidence of weight gain [77]. Saroglitazar is a dual agonist of α and γ PPAR. In a prospective, multicentre, double-blind, placebo-controlled study involving 106 patients with MASLD/MASH, who were overweight or obese and exhibited elevated alanine aminotransferase activity, patients in the saroglitazar group demonstrated a reduction in liver fat content (assessed by MRI), along with improved management of dyslipidaemia and insulin resistance [78]. In an Indian study involving 112 patients with MASLD, administration of 4 mg of saroglitazar for 52 weeks resulted in improvements in hepatosteatosis and fibrosis (evaluated via elastography) as well as improvements in carbohydrate and lipid metabolism parameters, without alterations in body weight; this led to the approval of the drug in India for patients with stage F1-F3 fibrosis [79]. Elafibranor is a dual agonist of PPARα and PPARδ receptors. In the GOLDEN study, a multicentre, double-blind, randomized, placebo-controlled trial involving 183 patients, those receiving a 120 mg dose exhibited a higher resolution rate of MASH (19-20% compared to 9-11%) and a reduction in fibrosis stage; the drug was generally well tolerated, though it resulted in a reversible increase in creatinine concentration (4.31 ±1.19 µmol/l) [80].
Farnesoid X receptor (FXR) agonists represent another intriguing class of pharmaceuticals that have shown potential in MASLD therapy. FXR is a receptor localized in the liver and intestine that regulates the synthesis and enterohepatic circulation of bile acids. The primary function of FXR is to inhibit the conversion of cholesterol into primary bile acids and to prevent the resorption of bile acids in the ileum, which underpins the modulation of the inflammatory process associated with MASH and the fibrosis process [81, 82]. The best studied of FXR analogues so far is obeticholic acid, a synthetic analogue of chenodeoxycholic acid, which has been recently approved for the treatment of primary biliary cirrhosis when ursodeoxycholic acid is insufficient (in 2016). In the phase 3 clinical trial REGENERATE, the percentage of pre-cirrhotic MASH patients (F2-F3) who received obeticholic acid and achieved a histological regression of fibrosis by at least one grade (without exacerbation of steatohepatitis) was 22.4% (compared to 9.6% in the control group) [83]. In another multicentre, double-blind, placebo-controlled, randomized clinical trial, FLINT, the therapy led to significant histological improvement of MASH (2-point or greater improvement in activity score without worsening of fibrosis) in 45% of treated patients vs. 23% in the placebo group [84]. Subsequent to the FDA’s rejection of the New Drug Application, further investigations into MASLD were halted [72]. Moreover, due to insights regarding the adverse risk-benefit ratio and the outcomes of the COBALT study, the FDA rescinded the full approval of obeticholic acid for the treatment of primary biliary cholangitis – the drug is now restricted to patients with primary biliary cholangitis without cirrhosis or with compensated cirrhosis but no evidence of portal hypertension [85, 86]. Other lesser-known FXR agonists include tropifexor (which showed improvements in hepatic fat fraction and body weight reduction after 12 weeks of treatment in the phase 2 clinical trial NCT02855164), and cilofexor (which, in combination with firsocostat and semaglutide, has exhibited favourable effects on liver steatosis, inflammatory activity, and fibrosis). However, further research outcomes are needed [72, 87–89].
Summary
Despite continuous medical advances, we still do not have a typical pharmacotherapy targeting the treatment of steatosis and liver fibrosis in MASLD. Hence, considerable emphasis is now placed on lifestyle medicine aimed at the prevention of lifestyle diseases, particularly targeting the prevention of obesity, diabetes, dyslipidaemia and hypertension, and thus also MASLD. Occasionally, new pathways are proposed for the potential pharmacotherapy of steatohepatitis and its complications. We await the results of furthers studies on FGF21 agonists, ketohexokinase inhibitors, novel THR-α and THR-β agonists, ASK1 (apoptosis signal-regulating kinase 1) inhibitors, FXR agonists, and galectin or caspase inhibitors, among others [90]. Research targeting the modulation of the gut microbiota – through diet, probiotics, prebiotics or faecal microbiota transplantation (FMT) – is now a promising approach for the future treatment and prevention of MASLD progression.
Be that as it may, it is crucial to point out that, according to current EASL-EASD-EASO guidelines, the cornerstone of the management of MASLD is multidisciplinary care, directed at the prevention and treatment of hepatic and non-hepatic complications – reduction of cardiometabolic factors. The basis is non-pharmacological treatment: diet, systematic physical activity and management directed at weight reduction. Pharmacotherapy of MASLD should be reserved for patients with features of hepatic inflammation, especially as co-occurring fibrosis at F2 level or higher. In the case of less severe disease, the guideline authors emphasize that conservative prevention and appropriate treatment of comorbidities – the aforementioned obesity, diabetes, dyslipidaemia and hypertension – is justified [1, 91, 92].





