
Introduction
Coronary artery bypass grafting (CABG) plays an important role in the revascularization of ischemic heart disease. After CABG, stroke is a rare but devastating complication, and its incidence is 1.6–3% depending on the patient population and individual surgical procedures [1, 2]. The main etiology of intraoperative stroke is embolism, followed by multiple etiologies and strokes because of hypoperfusion [3].
For patients suffering from coronary artery disease (CAD), there have been studies that show the relative correlation between the use of neutrophilia [4] and lymphocytopenia [5] as negative prognostic factors. There is also some research that identifies the correspondence between neutrophil-lymphocyte ratio (NLR) and CAD patients’ severity [6] as well as an adverse event in stable CAD [7]. In the past years, some studies have revealed that the NLR is associated with the prognosis of ischemic stroke (IS) [8].
Platelets play an important role in the pathogenesis of atherosclerosis [9], both in plaque development and in fibrin plug formation caused by unstable plaque rupture [10]. Although lymphocytes, which are a major sub-type of the leukocyte family, also play a role in chronic inflammation, many studies have revealed a relationship between low lymphocyte count and increased cardiovascular disease [11]. It is a new marker of clinical significance in the platelet-lymphocyte ratio (PLR) in coronary artery disease [12]. It was reported in previous studies that the elevation of red blood cell distribution width (RDW) is associated with clinical outcomes of diseases such as cardiovascular disease and stroke [13, 14] and that RDW elevation predicts morbidity and mortality regardless of other factors in coronary artery disease [11, 12]. Previous studies have shown that increased preoperative RDW independently predicts mortality and early complications after CABG [13, 14].
However, as far as we are concerned, the relationship between ischemic stroke and preoperative NLR, PLR, and RDW values after CABG surgery has not been examined yet.
Aim
In the present study, our purpose was to examine the full blood count parameters in the preoperative period, which is very easy to do, and the relations between preoperative NLR, PLR, and RDW values and ischemic stroke after CABG.
Material and methods
Subjects
A total of 1240 patients undergoing CABG between September 2016 and June 2019 were included in the study, which was designed as a retrospective and observational study. Patients were diagnosed with ischemic stroke by evaluating the neurology consultation results and radiological imaging (CT or MRI) findings in the postoperative period. All patients included in the study had carotid artery and vertebral artery imaging performed using either Doppler, BT angiography, or MR angiography methods. Patients with carotid artery occlusion and patients who underwent carotid endarterectomy with CABG were not included in the study. Cerebrovascular perfusion was checked routinely with near-infrared spectroscopy (NIRS). All patients were using acetylsalicylate, other antiaggregants, and/or statins before surgery. Patients who were under the age of 18, who received a blood transfusion within 4 months, heart transplantation, dissection, aneurysm, carotid endarterectomy, valve surgery or other vascular surgery were excluded from the study.
The study data were collected after the Ethics Committee of Retrospective Studies approved the study (number 72300690-79; 12-27.11.2019). Preoperative, intraoperative, and postoperative data of the patients with medical data such as age, gender, presence of comorbidity (hypertension, diabetes, hyperlipidemia, and coronary artery disease), white blood cells (WBC), number of neutrophil cells, lymphocyte cell count, hemoglobin (HB) concentration, RDW, and platelet counts were obtained by scanning the patient files from the hospital electronic database and archives. The full blood count data, taken only one day before the surgery, were used as the preoperative values in our study. Patients who did not meet this criterion were excluded from the study.
Statistical analysis
The Kolmogorov-Smirnov test was used to determine whether the distribution was normal. The continuous variables were compared using Students’ t-test or the Mann-Whitney U-test. The categorical data were compared using the χ2 test. The predictive value of routine hematological parameters was evaluated using receiver operating characteristic (ROC) curve analysis and a forward-conditional logistic regression model. All analyses were performed using SPSS 22.0, and a p-value of 0.05 was defined as statistically significant.
Results
The characteristics of the subjects are given in Table I and hemogram values are given in Table II. A total of 1240 CABG patients were included in the study, 40 of whom had ischemic stroke (IS). In the postoperative period, stroke occurred in 22 patients in the first 24 h, in 13 patients between 24 and 72 h, and in 5 patients after 72 h. The average age was higher, and the HB value and lymphocyte count were lower in patients who underwent IS (p < 0.001); also, there were high NLR, PLR, and RDW ratios (p < 0.001) together with more mechanical ventilator days, days hospitalized, and days in the intensive care unit (p < 0.001). The use of statins and acetylsalicylic acid was higher and statistically significant in patients who had no ischemic stroke after CABG (p < 0.001); and the use of other antiaggregants (e.g. clopidogrel, dipyridamole, ticlopidine) was found to be high in patients with stroke (p = 0.033). Also, the duration of the operation was longer, and reoperation, mortality, the opening of tracheotomy, and postoperative infection rates were higher in patients with postoperative ischemic stroke (p < 0.001).
Table I
Clinical characteristics of subjects (mean ± SD, n (%))
Table II
Hemogram values (mean ± SD)
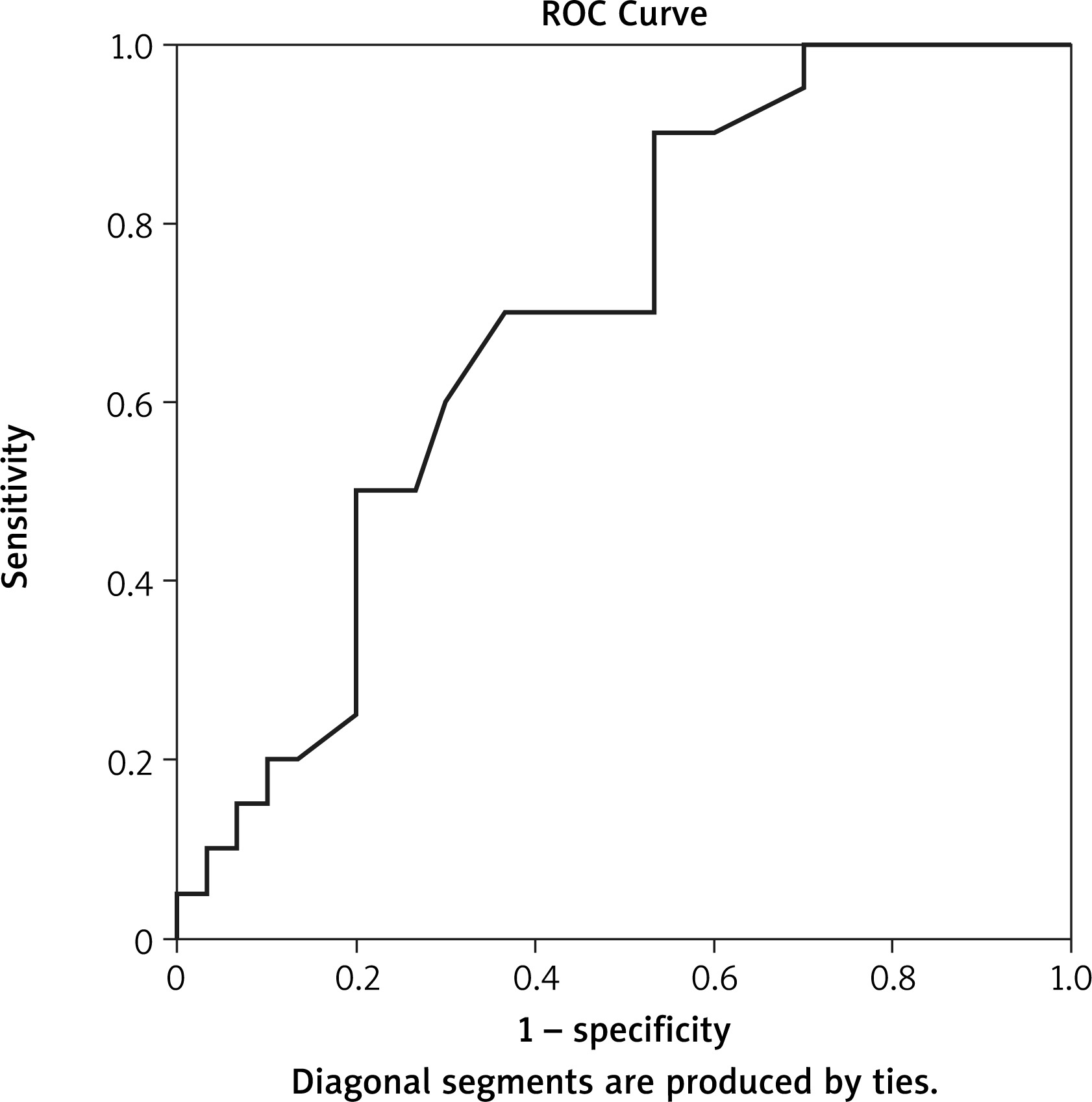
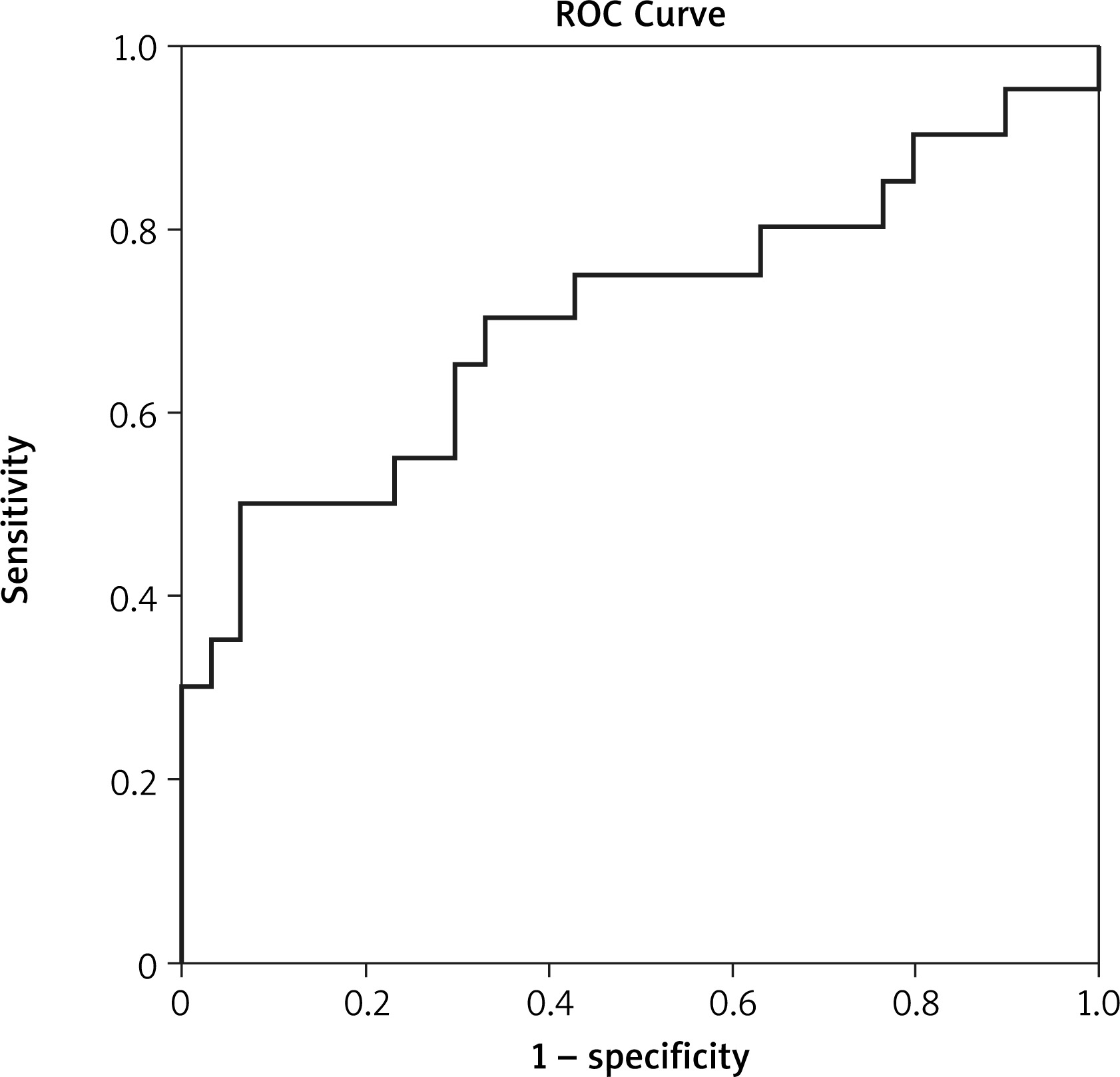
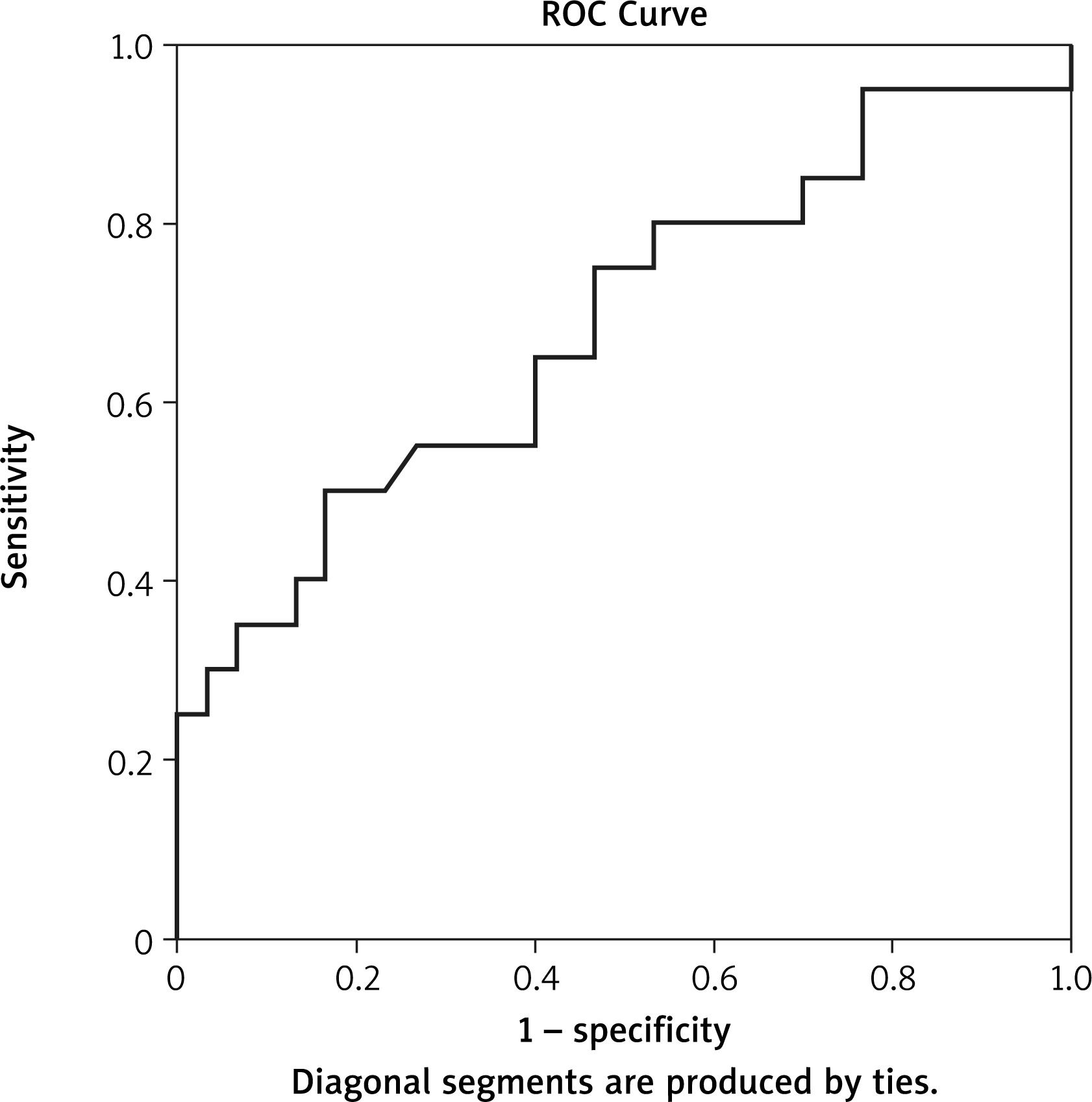
When the two groups are compared in Tables I–III, it can be seen that preoperative risk factors differed in terms of gender, age, HB, RDW, lymphocytes, preoperative neurological disease, acetylsalicylate use, use of other antiaggregants, reoperation, surgery duration, statin use, NLR and PLR values. However, in a multivariable model, only age, RDW, surgery duration, NLR, and PLR were independently associated with postoperative ischemic stroke, with ORs of 1.10 (95% CI: 1.02–1.18), 1.02 (95% CI: 1.01–1.049), 1.62 (95% CI: 1.15–2.35), 2.02 (95% CI: 1.39–2.95), 1.02 (95% CI: 1.00–2.92), respectively. The results were: RDW area under the curve (AUC): 0.696 in Figure 1, PLR AUC: 0.703 in Figure 2, and NLR AUC: 0.684 in Figure 3.
Table III
Multivariate logistic regression
Discussion
In this study, NLR, PLR and RDW elevation was proven to be an independent risk factor in patients with ischemic stroke after CABG. Many previously conducted studies reported that platelets play roles in the pathogenesis of atherosclerosis, lymphocytes are associated with inflammation, and low lymphocyte counts are associated with cardiovascular diseases. Lymphopenia is associated with mortality after ST-segment elevation myocardial infarction [8]. NLR has also been associated with long-term mortality in patients with ST-segment elevation myocardial infarction and acute decompensated heart failure [15, 16].
In this study, we investigated the relations between preoperative NLR, PLR, and RDW values with the emergence of ischemic stroke after CABG, which had never been investigated before, and found that with the appearance of ischemic stroke after CABG, advanced age, prolonged surgery duration, NLR, PLR, and RDW values are independent risk factors.
AF is an important cause of embolic ischemic strokes. In our patients, there was no statistically significant difference in terms of AF between the two groups with and without ischemic stroke. The embolic strokes that are associated with CABG are markedly caused by thromboembolisms and atheroembolisms and are released from aortic plaques [17]. Platelets play a role in the early stage of atherosclerosis that is associated with chronic vascular pathology [18] and plaque rupture [19]. The platelets in atherosclerotic plaque provide the replication of leukocytes via receptor-ligand interactions directly and increase leukocyte activity via chemokines [20]. Lymphocytes play an important role in healing with the induction of metalloproteinase-1 tissue inhibitor expression and mononuclear cell phenotype modulation [21]. Also, the stress in the chronic disease process causes activation of the hypothalamic-pituitary-adrenal axis. Activation of this axis causes cortisol secretion to increase, and a relative decrease in lymphocyte concentration [22]. For this reason, an increased PLR value can provide important data on inflammation and plaque instability.
Various immunological agents, such as interleukin (IL)-1, IL-3, and IL-6, which increase the number of platelets in the circulation as a result of megakaryocyte proliferation, are released in the proinflammatory stage associated with systemic inflammation [23]. In previous studies, it was found that the risk of thrombotic complications increases in patients with pathologically increased platelet counts, in other words, in patients with thrombocytosis [24]. It was found in experimental animal studies that platelets initiate atherogenesis and trigger complications [18, 25]. Previous studies also suggested that lymphopenia is associated with the progression of atherosclerosis and that lymphopenia may be caused by gradually increasing lymphocyte apoptosis with atherosclerotic load in atherosclerotic lesions, and decreased lymphocyte count was associated with poor prognosis [26].
The mechanism underlying the prognostic value of NLR, PLR, and RDW for IS following CABG is largely unknown. At least partially, we assumed that the prognostic value of routine hematological parameters might be explained by inflammation and stress. Previous studies showed that NLR, PLR, and RDW are inflammatory markers. Raised neutrophil counts and reduced lymphocyte counts are markers of worse outcomes in patients with acute coronary events and ischemic stroke [27, 28]. Post-surgery morbidity and NLR values were also closely associated. NLR was also seen as an independent predictor of increased risk of postoperative reintubation, atrial fibrillation, and amputation [29–31]. Associations between NLR and C-reactive protein (an inflammatory marker) were also observed [32]. Another study’s key finding is that neutrophil counts, alone or in combination, have the greatest impact on long-term death prediction, as measured by NLR or systemic inflammatory response index (SIRI) [33]. Inflammation plays a fundamental role in the development and progression of atherosclerosis [34].
Studies have shown that RDW has a positive correlation with inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) [35]. There are also several other studies showing that preoperative RDW is strongly related to surgical outcomes in cardiac surgery [36]. PLR increases with the inflammatory process and is used to predict the outcomes and independent mortality in cardiovascular diseases [37]. A study conducted by Idil Soylu et al. supports a good correlation between HS-CRP and PLR and that PLR is a good inflammatory marker [38]. As a result of all these studies, it may be speculated that both PLR and RDW are inflammatory markers.
In a study conducted by Taşoğlu et al. in patients with critical leg ischemia, they found that PLR was an independent risk factor for leg amputation [39]; and in another study, they found that preoperative high RDW in patients undergoing coronary bypass surgery was associated with increased long-term mortality [36]. Furthermore, the important conclusion in a study by Urbanowicz et al. is the strong relationship between inflammatory markers including monocyte-lymphocyte ratio (MLR), NLR, and PLR in off-pump coronary artery bypass grafting (OPCAB) patients and their mortality risk [40].
We found in our study that PLR and RDW values were higher (p < 0.001) in patients with ischemic stroke after CABG, and these high values were independent risk factors for ischemic stroke risk in patients admitted with CABG. These findings are important because no similar studies were found in the literature before.
We know that advanced age and prolonged operation time are important risk factors for stroke after CABG. This study showed that NLR, PLR, and RDW are independent risk factors for ischemic stroke in the multivariate model, except for operation time and age. The findings are important in this context.
Inflammatory markers, such as CRP, myeloperoxidase, and IL-6, were not examined and compared with RDW-PLR. The biggest limitation of this study is that it was a retrospective and single-centered study. The low number of cases is another limitation of this study.
Conclusions
The present study found that preoperative high PLR and RDW values may be considered as useful and independent risk factors for postoperative ischemic stroke prediction in patients presenting with CABG. RDW and PLR values obtained with a blood count, which is a low-cost test, can be used as a cheap and objective tool to predict the occurrence of adverse events such as postoperative ischemic stroke in patients presenting with preoperative CABG.









