
Introduction
Advanced liver disease is associated with portal hypertension, leading to the development of gastroesophageal varices. There is a strong correlation between the severity of liver disease and the development of esophageal varices. Esophageal varices (EVs) are seen in 30-40% of patients with compensated cirrhosis and up to 80% of those with decompensated cirrhosis [1]. Bleeding from esophageal varices occurs at a rate of 5-15%/year, which varies with the size of the varices, the presence of red wale marks on varices, and the severity of liver dysfunction (Child status C) [1, 2]. Endoscopic variceal ligation (EVL) is the mainstay therapy for managing acute variceal bleeding [1, 2]. In patients who are intolerant of non-selective β-blockers (NSBB), EVL is the preferred therapy for primary prophylaxis, while for secondary prophylaxis, it is used in combination with NSBB [1, 2]. However, the pathophysiology of portal hypertension is not affected by EVL. Hence, recurrence of esophageal varices and rebleeding are common after endoscopic therapy [1, 2]. The reported rebleeding rate after emergency EVL is up to 15% within 5 days and 17% within 6 weeks [3-5]. Both variceal hemorrhage and post-EVL ulcers can contribute to post-EVL bleeding or rebleeding [6]. Although post-EVL ulcer is an uncommon complication of EVL, it is associated with significant mortality [7].
Currently, there is no consensus on the predictors of early bleeding after EVL and its prevention. Multiple studies have been conducted for deriving predictors of early post-EVL bleeding. However, there is significant heterogeneity among the studies concerning the risk factors. To ensure their general applicability, instead of deriving them from a single study, it was sought to determine the predictors across multiple populations. Hence, this systematic review and meta-analysis (SMA) aimed to assess the incidence, associated risk factors, and outcome of early bleeding after EVL.
Material and methods
The current meta-analysis was conducted as per the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) [8] and the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [9]. This SMA has been registered with PROSPERO.
Database search
Electronic databases of MEDLINE and ScienceDirect were searched from 2000 to November 2021 for all relevant studies using the keywords: (Varices) AND (“Band ligation” OR EVL) AND (Bleeding OR Rebleeding OR Ulcer). Screening of the title and abstract of studies retrieved using the search strategy was done by two independent reviewers. Studies that potentially met the inclusion criteria were extracted. Two researchers independently assessed the full texts before including them. The bibliography of the included studies was also searched for any relevant studies. In case of any disagreement, it was resolved by a third reviewer.
Study inclusion
Studies included in this analysis were prospective cohort and retrospective case-control studies fulfilling the following criteria: 1) study population – patients with portal hypertension and esophageal varices; 2) intervention – EVL for acute variceal bleeding control or prophylaxis; 3) outcomes – early bleeding after EVL and associated mortality. Conference abstracts, case reports, case series, studies on pediatric patients, review articles, correspondences, editorials and studies in languages other than English were excluded. Studies without relevant clinical data or with incomplete data were also excluded.
Data extraction and quality assessment
Data was collected into a structured data extraction form by two independent reviewers. The form contained the following parameters of each study: title, first author, year of publication, country, number of patients, age and gender, clinical presentation, inclusion and exclusion criteria, outcome measures, and duration of follow-up. Two independent reviewers assessed the quality of the included studies using the Newcastle-Ottawa scale for cohort studies [10]. A study with a score of 7-9 has high quality, 4-6, high risk, and 0-3 very high risk of bias. A third independent individual was consulted to determine the best score based on any discrepancy in the study quality assessment.
Outcomes assessed
The primary outcome was the incidence of early bleeding, which was defined as bleeding or rebleeding related to portal hypertension within 8 weeks after EVL (but not within the first 5 days). The secondary outcomes included mortality related to the episode of early bleeding and the various predictors of early bleeding significant on univariate or multivariate analysis.
Data analysis
The pooled proportions were computed using a random-effects inverse-variance model with DerSimonian-Laird estimate of t2 [11]. The heterogeneity was assessed by I2 and the p-value of heterogeneity. P < 0.10 was taken as statistically significant while I2 values of < 30%, 30% to 60%, 61% to 75%, and > 75% were considered as low, moderate, substantial, and considerable heterogeneity, respectively. The pooled odds ratios (pOR) and their associated 95% confidence intervals (95% CI) were obtained for all variables selected as significant by at least two multivariate analyses or three univariate analyses. pOR were calculated by including the raw data and the results of all the studies regardless of whether the variable was significant. The continuous variables were analyzed using mean difference and inverse variance. The heterogeneity was assessed by I2 statistics, with values < 25%, 25% to 50% and > 50% being considered as low, moderate, and significant, respectively. The assessment of publication bias was done by evaluation of funnel plot asymmetry and quantified using Egger’s test. Sensitivity analysis was done by conducting leave-one-out meta-analysis, which excludes one study at each analysis to investigate the influence of each study on the overall effect-size estimate and to identify influential studies. The meta-analysis was performed using the Stata 17.0 software package (Stata Corp LP, College Station, TX, USA) and RevMan software (version 5.4.1, Cochrane Collaboration).
Results
Study characteristics and quality assessment
A total of 879 records were identified, out of which 794 were screened after removal of duplicates. Thirty reports were assessed for eligibility and 16 studies [12-27] were included in the final analysis. Figure 1 outlines the detailed search strategy as per the PRISMA guidelines. Table 1 summarizes the characteristics of the included studies. The sample size of the studies varied from 146 to 4579. The pooled mean age of the patients was 56.0 ±9.7 years. Only 3 studies included patients undergoing elective EVL [12, 19, 26] while the other 13 studies reported data on patients undergoing EVL for both elective and emergency indications [13-18, 20-25, 27]. The duration of follow-up varied from 2 weeks to 6 weeks. Among the included studies, 6 were of high quality [12, 13, 16, 19, 23, 26], while 10 had high risk of bias [14, 15, 17, 18, 20-22, 24, 25, 27].
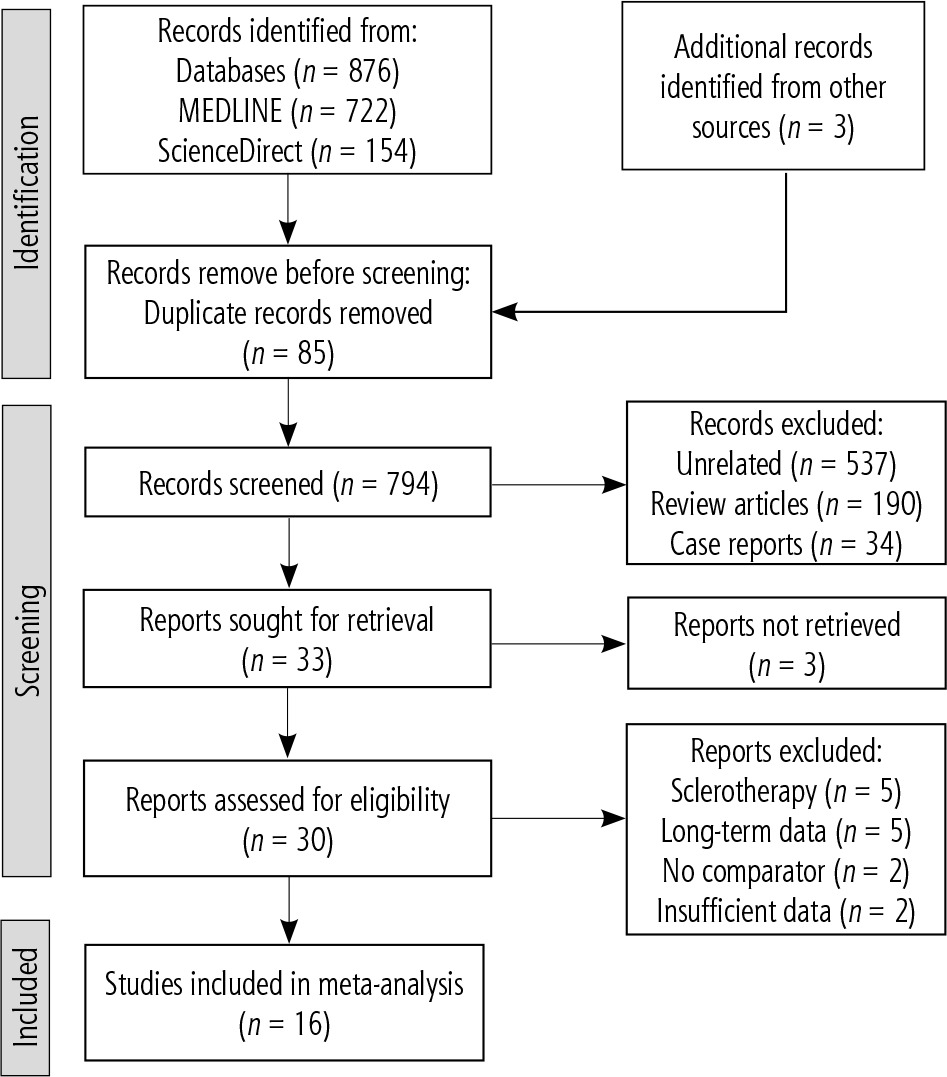
Table 1
Characteristics of included studies
| Author | Country | Study design | No. of patients | Male/female | Age (years) Mean (SD) | Indication of EVL# | Follow-up | No bleeding | All-cause rebleeding | Post-EVL ulcer bleeding | Interval of bleeding | Study quality* |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vieira da Rocha 2009 [12] | USA | Prospective | 150 | 92/58 | 54 ±13 | Elective | 6 weeks | 139 | – | 11 | 9.4 ±4.5 | 8 |
| Petrasch 2010 [13] | Germany | Retrospective | 255 | 165/90 | 57.3 ±12.6 | Combined | 2 weeks | 225 | 30 | 14 | 7.0 ±3.2 | 7 |
| Vanbiervliet 2010 [14] | France | Retrospective | 605 | – | 57.5 ±14.1 | Combined | 4 weeks | 584 | – | 21 | 13.5 ±7.3 | 5 |
| Xu 2011 [15] | China | Prospective | 342 | 242/100 | 52.7 ±10.9 | Combined | 2 weeks | 316 | 26 | – | 8.0 ±2.3 | 6 |
| Ripoll 2013 [16] | Spain | Retrospective | 292 | 217/75 | 66.2 ±12.3 | Combined | 6 weeks | 260 | 32 | – | – | 7 |
| Mostafa 2014 [17] | Egypt | Prospective | 146 | 105/41 | 51.8 ±10.5 | Combined | 6 weeks | 116 | 30 | – | – | 6 |
| Sinclair 2015 [18] | Australia | Retrospective | 347 | 251/96 | 55 ±7.0 | Combined | 2 weeks | 309 | 38 | 18 | – | 6 |
| Kang 2016 [19] | Korea | Retrospective | 505 | 388/117 | 53.6 ±10.6 | Elective | 6 weeks | 491 | – | 14 | – | 7 |
| Cho 2017 [20] | Korea | Retrospective | 430 | 363/66 | 59.5 ±11.1 | Combined | 6 weeks | 397 | – | 33 | 8.5 ±5.1 | 5 |
| Duenas 2019 [21] | Spain | Retrospective | 170 | 136/37 | 57.7 ±12.8 | Combined | 6 weeks | 139 | 31 | 21 | 12 ±5.6 | 6 |
| Elhawari 2019 [22] | Egypt | Prospective | 126 | – | – | Combined | 2 weeks | 116 | – | 10 | 9.2 ±3.7 | 6 |
| Jamwal 2019 [23] | India | Retrospective | 3854 | – | 46.6 ±11.3 | Combined | 6 weeks | 3713 | – | 141 | – | 8 |
| Kundumadam 2020 [24] | USA | Prospective | 454 | 278/176 | 57.1 ±11.1 | Combined | 4 weeks | 430 | 24 | – | 12 ±7 | 5 |
| Reji 2020 [25] | Australia | Retrospective | 336 | 235/101 | 56.0 ±11.5 | Combined | 3 weeks | 317 | – | 19 | 11 ±1.6 | 6 |
| Drolz 2021 [26] | Germany | Retrospective | 787 | 550/237 | 58.5 ±4.6 | Elective | 4 weeks | 749 | 38 | – | 12.75 ±2.58 | 8 |
| Hu 2021 [27] | China | Retrospective | 4579 | 3536/1043 | 54.9 ±9 | Combined | 6 weeks | 4191 | – | 388 | 11.4 ±2.3 | 5 |
Incidence of early bleeding after EVL
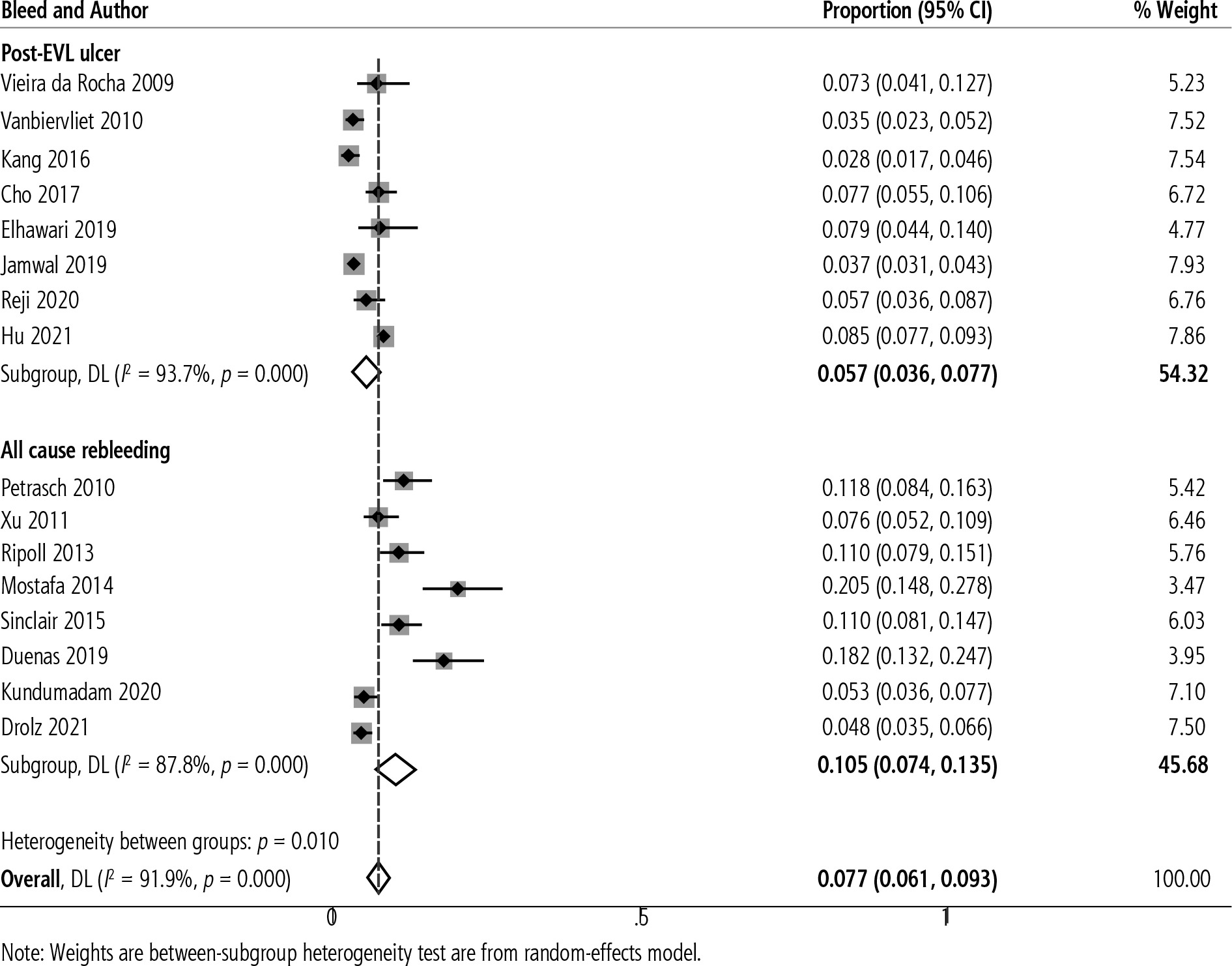
The pooled incidence of early post-EVL bleeding was 7.7% (95% CI: 6.1-9.3, I2 = 91.9%) with data from 16 studies [12-27] (Fig. 2). The pooled mean interval from EVL to bleeding was 11.2 ±3.2 days. On subgroup analysis, the incidence of all-cause bleeding was 10.5% (95% CI: 7.4-13.5, I2 = 87.8%) while the incidence of bleeding due to post-EVL ulcer was 5.7% (95% CI: 3.6-7.7, I2 = 93.7%) with heterogeneity between the two groups (p = 0.010).
Predictors of early post-EVL bleeding
Figure 3 shows a summary of all the predictive factors analyzed in the included studies. A total of 34 factors were analyzed, among which 14 parameters were found to be significant predictors of early bleeding after EVL. Seven factors were significant on multivariate analysis in 2 or more studies (use of proton pump inhibitor [PPI] after EVL, peptic esophagitis, presence of gastric varices, use of higher number of bands, presence of hepatocellular carcinoma [HCC], lower hemoglobin at admission, MELD score) and 7 factors were significant on univariate analysis in 3 or more studies (age, emergency indication for EVL, large esophageal varices, presence of high-risk stigmata, higher serum bilirubin, lower serum albumin, Child-Pugh C status). Table 2 summarizes the relative effect of various parameters for risk of bleeding with subgroup analysis based on type of bleeding (all-cause bleeding or post-EVL ulcer bleeding). Figures 4-7 show the forest plot for significant factors associated with risk of bleeding or rebleeding with subgroup analysis.
Fig. 3
Parameters evaluated for association with early bleeding/rebleeding after endoscopic variceal ligation
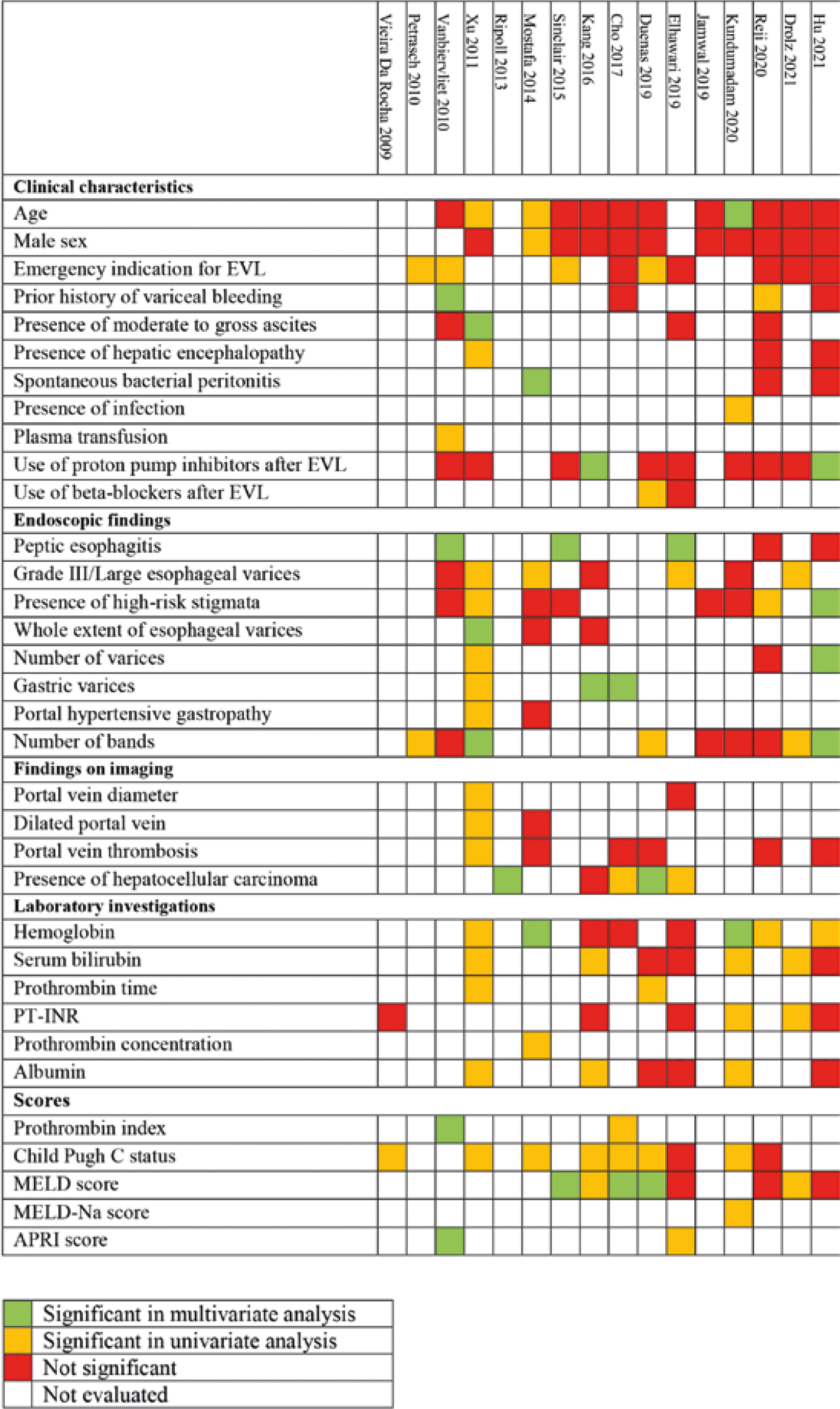
Fig. 4
Forest plot showing the odds of rebleeding with (A) presence of peptic esophagitis and (B) gastric varices
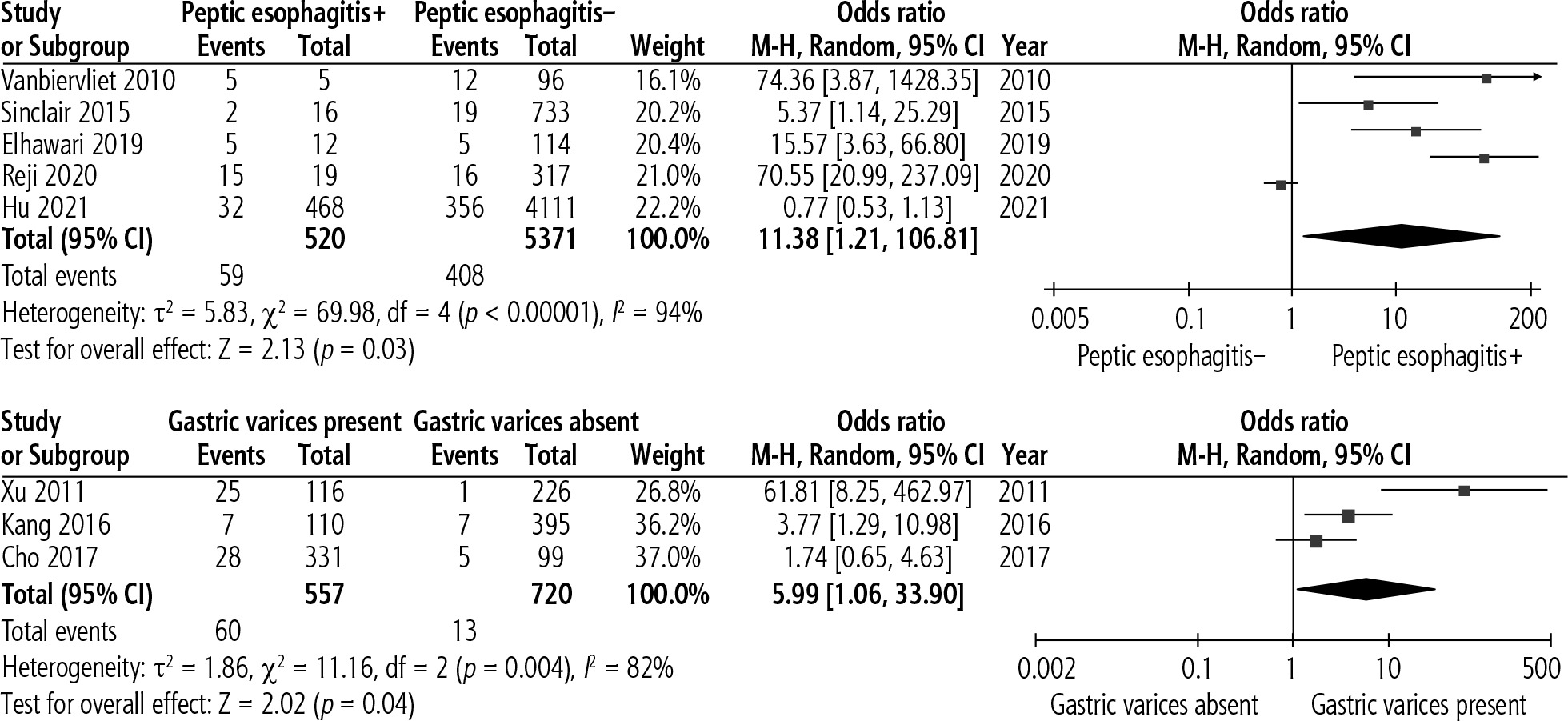
Fig. 5
Forest plot comparing the difference in number of applied bands between early bleeders and non-bleeders
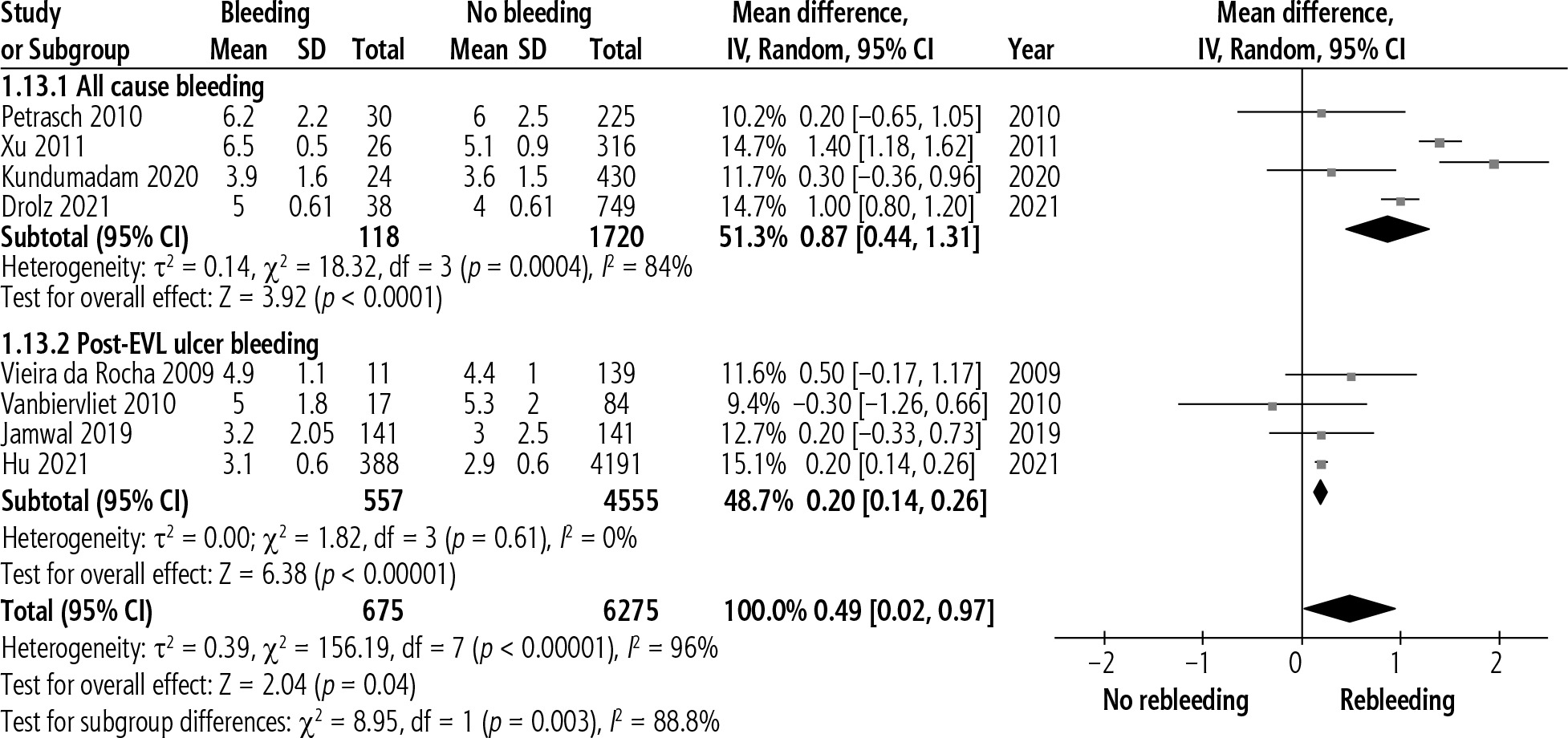
Fig. 6
Forest plot comparing the difference in mean hemoglobin between early bleeders and non-bleeders
Table 2
Summary table of risk factors associated with early bleeding with subgroup analysis
Mortality with rebleeding after EVL
A total of 12 studies [14, 15, 18-27] with 753 patients reported on mortality after development of early post-EVL bleeding. The pooled incidence of mortality was 25.2% (95% CI: 14.0-36.3, I2 = 90.8%). The incidence of mortality with all-cause bleeding was 27.2% (95% CI: 17.9-36.5, I2 = 0.0%) while the incidence of mortality with post-EVL ulcer bleeding was 24.5% (95% CI: 11.2-37.8, I2 = 91.9%) with no heterogeneity between the two groups (p = 0.741).
Assessment of publication bias, meta-regression, and sensitivity analysis
Visual examination of the funnel plots showed publication bias with the incidence of post-EVL bleeding but not associated mortality. Among the predictors, the presence of peptic esophagitis, use of PPI after EVL, and presence of HCC were associated with publication bias. Meta-regression to analyze the source of heterogeneity associated with the incidence of post-EVL bleed showed insignificant associations with the year of publication, sample size, mean age, and follow-up duration. Leave-one-out meta-analysis showed a significant change in the odds ratio for the outcomes of peptic esophagitis, high-risk stigmata, serum albumin, and MELD score with exclusion of influential studies.
Discussion
The present analysis showed a pooled incidence of 7.7% for early post-EVL bleeding and 5.7% for bleeding due to ulcer development at the EVL site after a mean duration of 11.2 ±3.2 days. The presence of peptic esophagitis, associated gastric varices, deployment of a higher number of bands, lower hemoglobin level, and higher MELD score were the most important predictors of early bleeding after EVL. Child-Pugh C status, associated HCC, higher serum bilirubin level, presence of high-risk stigmata, and emergency indication for EVL were other less important factors that were found to be associated with an increased risk of post-EVL bleeding.
Variceal bleeding is known to occur more often in those with poor liver function, primarily due to uncontrolled portal hypertension [1]. The present analysis showed a significant association between poor liver function and post-EVL bleeding. Higher MELD score, Child-Pugh C status, and serum bilirubin level but not serum albumin were associated with an increased risk of early bleeding. However, post-EVL bleeding can be caused either by variceal hemorrhage or post-EVL ulcers. Usually, after EVL, the band remains attached to the esophageal wall for 3 to 7 days, and thrombi develop in the strangulated vessels [28]. Premature band detachment before variceal thrombosis exposes the vessel inside a post-EVL ulcer, leading to bleeding. On subgroup analysis, no significant association could be established between MELD score, bilirubin level, or serum albumin with bleeding due to post-EVL ulcer. Thus, contrary to variceal bleeding, post-EVL ulcer bleeding may not always be associated with the underlying liver dysfunction.
Changes in coagulation parameters are common in patients with cirrhosis, especially those with decompensation. However, the present analysis did not show any association of bleeding with the value of prothrombin time-international normalized ratio (PT-INR) or platelet count, which a rebalanced coagulation system may explain due to a reduction in both prothrombotic and anti-thrombotic factors. Vieira da Rocha et al. [12] found no difference in factor V, fibrinogen, protein C, protein S, von Willebrand factor, or thromboelastography between post-EVL bleeders and non-bleeders. In the study by Drolz et al. [26], peri-interventional use of coagulation products did not reduce the risk of bleeding complications after EVL.
Hepatic venous pressure gradient (HVPG) is known to be higher in patients who have had a variceal bleed than in those who have not [29]. Patients who undergo EVL for emergency indications tend to have higher HVPG and hence a higher risk of rebleeding. This finding is substantiated in our study as well. The risk of first variceal bleeding correlates independently with the size of the varix [29]. Contrary to the results of multiple studies, the present analysis did not show any association of the size of varices with the risk of early post-EVL bleeding. However, there was an increased risk of post-EVL bleeding with the presence of high-risk stigmata. It is hypothesized that high-risk stigmata indicate increased wall tension leading to weak mucosa, which provides an unstable site for the band placement. This results in premature band detachment followed by ulcer formation and bleeding.
Among the other endoscopic parameters, concomitant gastric varices was significantly associated with early post-EVL bleeding. EVL leads to a reduction in the blood vessel size but not blood volume and pressure. In the absence of gastric varices, the increased blood volume or pressure in the EVs can be compensated by diverting to cephalad collaterals (e.g., splenic vein) until the EVL-induced ulceration heals, to prevent rebleeding from the ulcer sites, which are more fragile than the original mucosa. However, in the presence of gastric varices, with retrograde blood flow and high pressure in the splenic vein, compensation cannot occur properly, and the remaining blood volume and pressure overload in the EV may result in rebleeding at the more vulnerable ulcer sites (EVL-induced ulcer bleeding) [20].
Another important finding was the association of HCC with an increased risk of bleeding. HCC can lead to increased portal pressure due to neovascularization, arteriovenous shunting within the tumor, and liver architecture modifications [30]. In turn, this may impact the risk of initial bleeding and rebleeding from esophageal varices. In the study by Ripoll et al. [16], analyzing the outcome of variceal bleeding in patients with HCC, 5-day failure was similar, but the 6-week rebleeding rate (16% vs. 7%, p = 0.025) and mortality rate (30% vs. 15%, p = 0.003) were higher in the HCC group. On multivariate analysis, Child-Pugh score, presence of HCC, presence of portal vein thrombosis (PVT), and lack of secondary prophylaxis were independent predictors of mortality.
In their landmark paper, Villanueva et al. [31] defined a hemodynamic response in HVPG by reduction > 10% after administration of NSBBs as predictive of decreased bleeding risk. Thus, reducing portal pressure by using NSBB may be a therapeutic option for preventing variceal bleeding. Dueñas et al. [21] observed a negative association between the dose of NSBB and the risk of rebleeding. However, the same has not been reported in other studies. The role of NSBBs in preventing early rebleeding after EVL is yet to be elucidated.
Currently, there are no guidelines recommending routine PPI usage after EVL. In the present analysis, peptic esophagitis was associated with an increased risk of early bleeding after EVL, but PPI use did not reduce the risk of bleeding. It is possible that the dose or duration of PPI may have been suboptimal. In a previous meta-analysis [32], the use of PPI was found to reduce the risk of bleeding after variceal endotherapy (OR = 0.52, 95% CI: 0.35-0.77), and this benefit of PPI was seen only when it was prescribed for > 1 month. Meanwhile, PPI use was not found to impact bleeding-related mortality. However, the studies included in the previous meta-analysis were heterogeneous, including EVL and sclerotherapy for esophageal varices and cyanoacrylate glue injection for gastric varices. Hence, further studies are needed to determine the optimal dose and duration of PPI to prevent early bleeding after EVL.
In the present analysis, the pooled incidence of mortality with early bleeding after EVL was 25.2%. However, we could not assess the predictive factors of mortality associated with post-EVL bleeding. Most studies reporting mortality have not accounted for competing risks. The present presumption that bleeding was the precipitating event underestimates mortality secondary to other competing risks in cirrhosis. This is an inherent shortcoming for most studies describing early rebleeding and also reporting mortality. In the study by Jamwal et al. [23], post-EVL bleeding ulcers (PEBUs) were classified based on their endoscopic appearance as types A (ulcer with spurting), B (ulcer with oozing), C (ulcer with clot or pigmented base), and D (ulcer with clean base). Type A and B ulcers were responsible for around 70% of mortality associated with PEBUs. Hence, endoscopic classification of PEBUs may help in deciding treatment strategies. However, this classification needs further validation.
The strengths of our study are that we were able to assess the incidence of post-EVL bleeding with associated mortality in a large cohort of patients. Also, the study was able to establish associations between various risk factors and bleeding after EVL. There are a few limitations to our meta-analysis which need discussion. First, the analysis included both prospective and retrospective studies, which may have limited data quality. However, due to the limited number of prospective studies, we would have missed important results by not including retrospective studies. Secondly, as a few parameters were not evaluated as they were not significantly predictive, we could have missed some potentially prognostic variables. However, the objective of the analysis was to determine the most consistent and reliable variables to predict post-EVL bleeding, and thus we included only variables that were strong predictors. Lastly, we could not assess the predictors of early post-EVL bleeding in non-cirrhotic patients, which remains a future area of research.
To conclude, early rebleeding after EVL is a common event occurring in 7.7% of patients. The presence of a lower hemoglobin level and higher MELD score at admission, associated gastric varices, and use of a higher number of bands during endoscopy, and peptic esophagitis on follow-up endoscopy, were the most important predictors of early bleeding after EVL in this meta-analysis. A higher index of suspicion for rebleeding must be kept in this cohort of patients after EVL for esophageal varices. Mortality secondary to rebleeding is high and occurs in 25% of patients. Close monitoring of high-risk patients who undergo EVL for the first 2 weeks is necessary to reduce mortality due to rebleeding.





