
Introduction
Liver transplantation (LTx) is the most curative therapy for end-stage cirrhosis of all etiologies. It has improved the life quality and expectancy of patients with end-stage liver disease [1]. However, both patients and physicians should be aware of the postoperative complications, which might be deleterious. With the longer achieved post-LTx survival, the incidence of metabolic disorders had increased [2]. Multiple factors have been incriminated in the pathogenesis of bone loss after transplantation [3]. Unconjugated bilirubin was reported to cumulatively enhance osteoblast proliferation. The well-defined insulin-like growth factor-1 (IGF-1) reduction in advanced cirrhosis had deterred bone remodeling and maintenance [4]. Additionally, post-menopausal hypogonadism might trigger the condition in females [5]. Moreover, deficiency of vitamin D in advanced liver disease might significantly affect the health of bones [6]. Other underrated risk factors including smoking, physical inactivity, alcohol consumption, older age, and low body mass index (BMI) have also been incriminated [7]. Corticosteroid use, common after transplantation and in patients with autoimmune liver disease, was reported to increase the risk not only of osteoporosis but also of avascular necrosis [8]. The adverse effects of glucocorticoids (GCs) and calcineurin inhibitors (CNIs) on bone remodeling have been reported [9]. The cumulative effects of advanced liver disease on bone osteodystrophy have been defined as an attribute [10]. Since some of these variables might be modifiable, identifying vulnerable groups is of importance. Accordingly, this study aimed to define the frequency of metabolic bone diseases (osteopenia and osteoporosis) after LTx by recruiting recipients who had undergone bone mineral density (BMD) measurement by DEXA, as well as the associated pre-operative and postoperative risk factors.
Material and methods
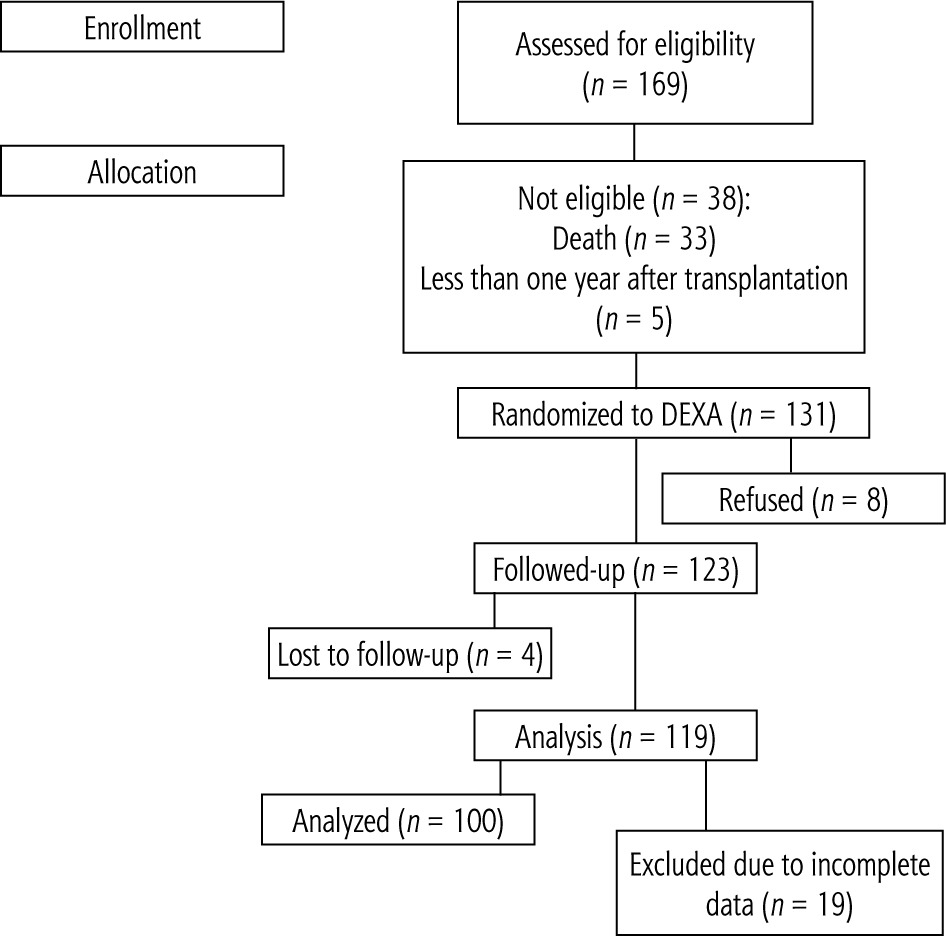
This observational prospective hospital-based study was conducted on one hundred consecutive adult patients (age ≥ 18 years) who underwent LDLT in the National Liver Institute, Menoufia University (NLI), and survived longer than one year. Enrolled cases were observed before, intra-operatively, and after liver transplantation with follow-up for at least one year (Fig. 1).
Donors were evaluated according to the NLI protocol (Kyoto University) [11].
Recipients were subjected to the following:
Informed consent: All enrolled patients had signed informed consent. The study was carried out according to good clinical practice (GCP) and the Helsinki Declaration of 1975 [12].
Calculation of BMI (kg/m2): BMI = kg/m2 where kg is a person’s weight in kilograms and m2 is their height in meters squared. A BMI of 25.0 or more is overweight, while the healthy range is 18.5 to 24.9. BMI applies to most adults aged 18-65 years.
Laboratory investigations (at post-transplantation discharge, 3 months, 6 months and one year after LTx): liver function tests (transaminases, albumin, alkaline phosphatase, γ-glutamyl transferase), complete blood count, renal function tests (urea, creatinine, uric acid, Na and K).
Diagnosis of diabetes mellitus (DM) according to the 2016 American Diabetes Association (ADA) criteria (2016): fasting plasma glucose (FPG) ≥ 126 mg/dl, or 2-h plasma glucose (PG) ≥ 200 mg/dl, or A1C ≥ 6.5%, or in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random PG ≥ 200 mg/dl.
Calculation of Model of End-Stage Liver Disease (MELD): according to the following formula: MELD = 3.78 × ln [serum bilirubin (mg/dl)] + 11.2 × ln [INR] + 9.57 × ln [serum creatinine (mg/dl)] + 6.43.
BMD measured by dual-energy X-ray absorption (DEXA): For all patients (once) one-year after LTx. The WHO has defined osteoporosis as a T-score of less than or equal to –2.5 and osteopenia as a T-score between –1.0 and –2.5. BMD is measured at both the spine and hip [13, 14]. Baseline BMD was not included in the study as it is not a routine pre-transplantation test according to the Kyoto University protocol.
Statistical analysis
Data were collected and entered into the computer using the SPSS program for statistical analysis. Quantitative data are shown as mean (M), standard deviation (SD), and range. Qualitative data are expressed as frequency and percent at the 95% confidence interval (95% CI). A χ2 test was used to measure the association between qualitative variables. Student’s t-test was used to compare means and standard deviations of two sets of quantitative normally and non-normally distributed data respectively. A logistic stepwise regression model was used to give an adjusted OR and 95% CI of the effect of the different independent and dependent risk factors for bony metabolic complications after liver transplantation. Two-tailed p (probability) values were considered statistically significant if less than 0.05.
Results
The frequencies of osteopenia and osteoporosis were found to be 14% and 8% among patients after LTx (Fig. 2). Seven recipients of the osteoporotic group were male. The mean values of age, and BMI before and after LTx in this group were 49.5 ±7.4 years, 24.1 ±4.7 kg/m2 and 22.8 ±1.5 kg/m2, respectively (Tables 1 and 2).
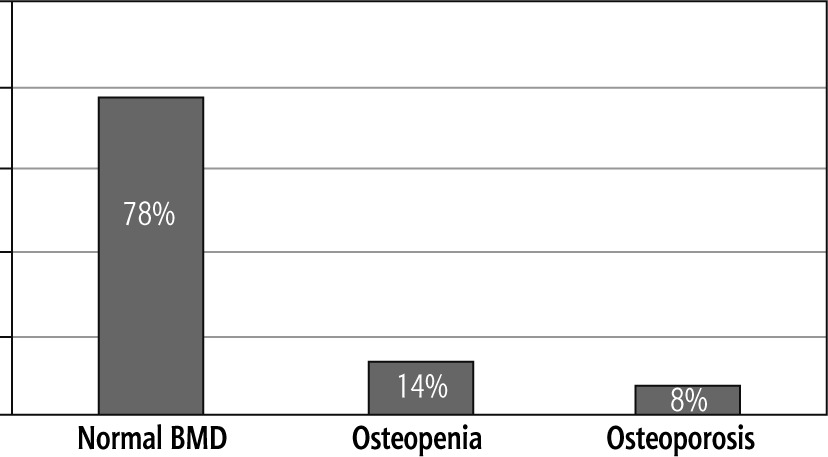
Table 1
Pre-liver transplantation (LTx) factors affecting bone disease (BD) occurrence after LTx
Table 2
Post-liver transplantation (LTx) factors affecting bone disease (BD) occurrence after LTx
A significant association was found between liver disease severity according to CTP score at the time of LTx and post-LTx MBD. In the osteoporotic group, 3 recipients were Child B, and 5 recipients were Child C (p < 0.05, 0.006). Alcoholism also was significantly linked to decreased bone mass (p < 0.05, 0.000) (Table 1).
The most common cause of cirrhosis in the osteoporosis patients was HCV in 5 recipients with a significant difference with the other two groups (p < 0.05, 0.000) (Table 1).
A significant difference was detected between those with and without bone disease regarding post-LTx development of DM and weight gain (p < 0.05, 0.028 and p < 0.05, 0.004) (Table 2).
The relation between immunosuppressive drugs and osteoporosis was found to be significant in post-LTx BD for both basiliximab (p < 0.05, 0.019) and pulse steroid therapy (p < 0.05, 0.000) (Table 3).
Table 3
Frequency of post-liver transplantation (LTx) bone mineral density (BMD) according to the immunosuppressive drugs
The binary logistic regression revealed that post-LTx occurrence of DM (p = 0.012, OR = 0.099), the severity of liver disease (p = 0.023, OR = 0.217), and HCV (p = 0.011, OR = 0.173) are the primary independent predictors of MBD occurrence one year after LTx (Table 4).
Table 4
Binary logistic regression of predictors of bone disease occurrence after liver transplantation (LTx)
Discussion
Metabolic bone diseases are not an infrequent presentation of liver transplantation. A collaboration of multiple factors including liver cirrhosis per se might be incriminated in the evolution of this disorder. Bone disorders especially if associated with higher frequencies of fractures have major impacts on health-related quality of life after LTx.
In the current study on Egyptian liver transplanted patients, evaluation of post-LTx bone disorders distinguished bone mass reduction in 22% of subjects: 14% with a low bone mass (osteopenia) and 8% with osteoporosis after a minimum follow-up of one year after LTx. However, no fractures were reported at any stage of follow-up. The sunny climate in Egypt might be responsible for the relatively good bone health in Egyptians, with lower fracture rates despite the presence of osteopenia.
Females with MBD represented 44.4%, while only 19.8% of the males in the cohort were affected. This reported higher occurrence in females than males could be attributed to the age-related osteoporosis due to loss of endocrine reserve. Another additional factor might be the lack of direct sun exposure for females as they always wear the Islamic veil outdoors.
In a similar vein were the results of Isoniemi et al. and Giannini et al., who reported that osteoporosis was found among 25% to 50% of women receiving a liver transplant [13, 14]. Fahrleitner et al., in a cross-sectional study, investigated 15 patients (10 male, 5 female) 20 ±6 months after LTx. Osteoporosis was present in 67% of the patients. Vertebral fractures were seen in 33% [15].
Segal and his associates tried to evaluate BMD, bone turnover, and calcium-regulating hormones in 29 patients (17 men, 12 women) from 2-12 years following LTx for non-alcoholic liver diseases and found bone mass changes in 65.5% of cases [16]. Baccaro et al. reported that approximately 21% showed osteoporosis and 35%, a low bone mass in a prospective, cross-sectional study of 23 female outpatient transplant recipients [17].
In the current study of the association between old age at transplantation, we did not observe a significant correlation between ages at the time of LTx and decreased bone mass. Baccaro et al. observed a significant association of older patient age at the time of liver transplantation with a decreased bone mass [17]. In contrast, Ninkovic et al. and Guichelaar et al. found an inverse relationship of age to decreased bone mass [18, 19].
In a metanalytic study, HCV was postulated to augment C-terminal cross-linking telopeptide of type I collagen (CTX), with subsequent boosted bone resorption endeavors [20]. However, the direct pathogenic effect of HCV virus infection on bone is still questionable.
As HCV is the main cause of liver transplantation in Egypt, and as an Islamic country, alcohol is not a main cause. However, this fact does not exclude presence of a few cases with alcohol-related liver cirrhosis.
Being alcoholic was a risk factor for an increased prevalence of decreased bone mass after LTx in the present study, which is consistent with Meys et al. [21]. Reduced serum testosterone levels occurring in both actively drinking alcoholics and patients with cirrhosis probably contribute to osteoporosis [21]. Low vitamin D levels have also been reported in about one-third of alcoholics with a low BMD, and vitamin D supplementation has been shown in one study to improve BMD at the wrist in some patients [22]. But, again the limited number of alcoholics included constrained thorough analysis of this point, added to the scarcity in the literature.
In the current study, a positive correlation was found between both excessive post-LTx weight gain and a family history of obesity with decreased bone mass. There are lots of speculations about adipose tissue production of adipokines, such as leptin, resistin, and adiponectin, which may negatively modulate BMD [23]. There is a scarcity of studies elucidating more clearly the role of previous variables in bone mass changes after LTx.
Development of diabetes after transplant also was reported as a risk factor in our study. Interestingly, there was evidence of interplay between diabetes and the potential mechanisms responsible for osteoporosis. Diabetes is often associated with changes in bone health, and the term “diabetic osteopathy” needs to be more precisely defined. Pathogenesis is related to insulin and subsequently IGF-1 deficiency (both have anabolic effects on the bone) [23].
In the current work, in agreement with Meys et al. and Diaz-Guerra et al., cholestatic disorders were associated with a greater prevalence of osteoporosis, although limited numbers (2 recipients) were due to malabsorption of calcium and vitamin D, in addition to the interference of bilirubin levels in osteoblast function [21, 24]. The study of Baccaro et al. questioned this as a cause-and-effect relationship [17].
In this study, the severity of liver disease as measured by the CTP score at the time of LTx was ultimately related to decreased bone mass. Reduced bone formation in chronic liver disease has been linked to low levels of IGF-1 in serum [25]. In osteopenic rats, treatment with IGF-1 results in increased BMD. However, a direct causal link between IGF-1 levels and osteoporosis in chronic liver disease in humans has not yet been established [26].
A confirmed deleterious effect of GCs on bone mass was proved in the current study, as with Morris et al. and Diaz-Guerra et al. [24-27]. In contrast were the studies conducted by Segal et al. [16], Guichelaar et al. [19], and Baccaro et al. [17], who claimed that the use of corticosteroids as an immunosuppressive drug did not affect the bone mass.
The pathophysiology of GC induced bone disorder is multifactorial. Bone formation is inhibited by decreased proliferation, function (by reducing levels of type I collagen, IGF-1, and osteocalcin), and lifespan (by induction of osteoblast apoptosis). GCs also promotes osteoclastogenesis by increasing levels of the receptor activator of the nuclear factor-κB ligand (RANKL) system. Other indirect effects of GCs also play a role in the mechanisms of bone loss (e.g. decreased intestinal calcium absorption, renal calcium wasting, and impaired gonadal hormone production). Furthermore, GCs may induce muscle weakness, which additionally delays post-transplant mobilization, with subsequent aggravation of bone loss [28].
The binary logistic regression has added substantial credibility to the post-LTx occurrence of DM, severity of liver disease, and HCV as independent predictors of MBD occurrence one year after LTx. These results had not been verified previously in similar studies.
Collectively, this study reported a significant association between the severity of liver disease as measured by the CTP score at the time of LTx, HCV, and post-LTx DM and decreased bone mass. However, the deleterious effects of GCs and basiliximab on bone mass that were suggested by univariate analysis were refuted by binary logistic regression. Compared with previous studies, this report had the advantage of the prospective design along with the fairly large sample, as well as dealing with the usually overlooked Middle East population. However, missed pre-LTx baseline bony evaluations constituted a flaw in the current study which might be an alarm mandating more concern in Egyptian adopted protocols. Further multicenter national studies are still needed to elucidate the potential contributing factors for post-LTx metabolic bone diseases over longer follow-up periods.
Conclusions
Metabolic bone disease is suggested to be one of the most overlooked consequences after LTx which might poorly affect a patient’s quality of life. Lifestyle modifications along with proper nutritional interventions are mandatory. DEXA scanning is recommended to be done yearly after LTx. Control of other metabolic complications after LTx might be worthwhile.
Ethics approval and consent to participate
The study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institutional review board of the National Liver Institute (NLI IRB 00003413), Menoufia University. Written informed consent was obtained from both donors and recipients regarding surgery and research.
All included patients have approved publication.
Data used to support the findings of this study are included within the article.





